
Abstract
Introduction
Nurses and respiratory therapists working on the frontline during the pandemic surge were short-staffed and worked extended hours while adding new tasks to already demanding workloads. As the world watched news covering COVID-19's effect, nurses and respiratory therapists lived through the daily stress of treating each patient with care, dignity, and compassion. Limited studies have focused on this population, which is vital to providing care and saving lives; research is needed to understand nurses’ and respiratory therapists’ experiences during the COVID-19 pandemic.
Objective
The study aimed to understand nurses’ and respiratory therapists’ experiences during the COVID-19 pandemic.
Methods
A qualitative descriptive study, informed by naturalistic philosophy, was designed to obtain a detailed account of participants’ experiences during the pandemic surge. A purposive sample was recruited and enrolled from the community through professional organizations and snowball sampling from December 2021 to September 2022. Data was analyzed using thematic analysis.
Results
Participants were seven registered nurses and six respiratory therapists employed full-time in an intensive care unit, step-down intensive care unit, emergency department, or medical-surgical unit; seven (53.8%) with an associate degree, and six (46.2%) with a bachelor's degree. Eight (66.7%) self-identified as White, one Asian, one non-Hispanic Black, and two Pacific Islanders. The mean age was 40, and 10 (76.9%) were female. Six primary themes emerged: (a) the work–life experience before the COVID-19 pandemic, (b) the work–life experience during the COVID-19 pandemic, (c) the personal life experience during COVID-19, (d) the coping period, (e) the professional role change, and (f) the work and personal life experiences post COVID-19 surge.
Conclusion
The knowledge gained from this study can help improve understanding of the professional quality of life, the need for organizational and community support, and for healthcare professionals to seek help and practice self-care to prevent burnout and secondary traumatic stress.
Introduction
The SARS-COV-2 (COVID-19) pandemic has caused drastic changes globally since its emergence in late 2019. Nurses and respiratory therapists helped navigate countless patients and families through unimaginable conversations and healthcare decisions during the ever-changing circumstances. As millions watched news covering COVID-19's effect, nurses and respiratory therapists lived through the daily stress of treating each patient with care, dignity, and compassion while supporting family members who were angered at their current situation. Notably, many family members were locked out and unable to see loved ones during their last moments, leaving the nurses as the bridge to comfort both. Nurses and respiratory therapists working on the frontline during the pandemic were short-staffed and worked extended hours while adding new tasks to already high workloads. This increased workload with higher acuity patients, short staff, and knowing their lives were in jeopardy made the situation challenging (Ardebili et al., 2021; Cadge et al., 2021). Many healthcare providers were outside of their comfort zone, performing jobs they had not performed since graduation. They were required to learn new and evolving protocols, sometimes even changing within the same shift (Liang et al., 2021). Further research is needed to elicit a comprehensive understanding of nurses’ and respiratory therapists’ experiences during the global pandemic.
Review of Literature
The incidence of stress and its potential impact on healthcare providers is a known occupational hazard. Areas of higher acuity with repeated exposures to high-stress situations, particularly during the COVID-19 pandemic, placed healthcare providers in unsustainable situations. At the start of the novel COVID-19 pandemic, many experts lacked the knowledge and experience to address the increasing number of hospitalizations and deaths. Patients’ care was delayed due to the overwhelming number of COVID-19 cases being treated in the emergency department, acute care, and outpatient settings (Liang et al., 2021; Trachtenberg et al., 2023). Medical procedures were postponed due to the overwhelming number of hospital-occupied beds.
The uncertainty and inherently unpredictable developments generated by COVID-19 have implications for the well-being of healthcare providers and the global population (Baptista et al., 2021; Ghahramani et al., 2022; Janitra et al., 2023). Notably, during the early phase of the pandemic, many healthcare providers did not clearly understand the virus, how to manage it, were faced with ethical dilemmas, and were unaware of the consequences of the decisions they made caring for the patients (Shin & Yoo, 2023). Consequently, patients admitted to the hospital were incredibly ill. Healthcare providers were overwhelmed with stressful situations, a lack of staff support and medical supplies, and fear for their health and the health of their loved ones (Ghahramani et al., 2022; Liang et al., 2021).
Recent research has identified a significant preponderance of insomnia, stress, and anxiety throughout the COVID-19 pandemic among health professionals and the general population (Ghahramani et al., 2022; Janitra et al., 2023; Trachtenberg et al., 2023). Baptista et al. (2021) examined primary care physicians’ burnout during the COVID-19 pandemic. Findings indicated that female practioners and long years in practice were associated with increased levels of burnout. Shin and Yoo (2023) conducted a study with nurses working in tertiary hospitals’ intensive care units and internal medicine wards in Seoul, Korea. The nurses who provided patient care during COVID-19 had a sense of calling.
Liang et al. (2021) phenomenological study examined Taiwanese nurses’ experience caring for patients during the COVID-19 pandemic. Their study findings support nurses’ value of learning and innovation when faced with a rapidly changing work environment. Notably, they can improvise to protect themselves and care for their patients effectively. Nonetheless, the lack of support from the hospital administration affected their mental wellness, leading to burnout.
Trachtenberg et al. (2023) explored nurses (n = 16) and respiratory therapists’ (n = 4) experiences providing direct care to COVID-19 patients in the ICU during the first surge of the pandemic at a large academic medical center in the Northeastern United States. Five major themes characterized the providers’ experiences: a fear of the unknown, concerns about infection, perceived professional unpreparedness, isolation and alienation, and inescapable stress and distress. Data revealed the importance of individual-level self-care, resiliency, practical coping skills, and providing adequate and consistent support for staff before, during, and after times of crisis by healthcare institutions.
Limited studies have focused on the lived experiences of nurses and respiratory therapists during the pandemic surge and populations vital to providing care and saving lives. Additional research is required to elicit an inclusive understanding of nurses’ and respiratory therapists’ experiences during the global pandemic. The study reported here provided a unique opportunity to speak with healthcare providers who experienced the effects of the COVID-19 pandemic on their professional lives and well-being to gain a deeper understanding of the causes of distress and strategies for coping with stress and loss experienced during the pandemic in Southern California. The study aimed to understand nurses’ and respiratory therapists’ experiences during the global pandemic.
Methods
Design
A qualitative descriptive study informed by a naturalistic philosophy was designed to obtain a detailed, vivid representation of the participants’ experiences with little interpretation and to understand the complexity of the human experience during the pandemic (Lincoln & Guba, 1986; Sandelowski, 2000, 2010).
Interview Questions
The following open-ended questions guided the semi-structured interview:
When did you become a nurse/respiratory care practitioner (RCP), and what drove you to the profession? What was your daily work life before the COVID-19 pandemic? Did you enjoy your work life before the COVID-19 pandemic? What was your everyday work life like during the peak of the COVID-19 pandemic? In what way did COVID-19 affect your personal life? How has your work/personal life changed post-COVID-19 pandemic surge? How have your relationships with your co-workers changed since the COVID-19 surge? Now that the surge has subsided, how do you feel about your role as a nurse/RCP?
Setting and Sample
A purposive sample of nurses and respiratory therapists was recruited and enrolled from the community, a large urban setting with diverse populations, including Hispanics, Asian Americans, Pacific Islanders, Blacks, American Indians, Caucasians, multiracial, veterans, military, and foreign-born through professional organizations and snowball sampling, from December 2021 to September 2022.
Inclusion Criteria
Eligible participants had to have worked in the hospital or the outpatient setting during COVID-19, be 18 years or older, participate in a semi-structured interview, and be proficient in English. Seven registered nurses and six respiratory therapists who had direct contact with patients before and during COVID-19 provided data for this study. We excluded healthcare administrators who had no direct contact with patients.
Procedure of Data Collection
Potential participants were contacted by phone or email to inform them about the study. Participants completed informed consent and a demographic questionnaire, with the forms returned via email or handed to the investigator before the scheduled interview. Interviews were scheduled per participants’ preference and conducted via Zoom with audio recording to collect data for transcription; video recording was not activated during the interviews. Participants were encouraged to use reflection and to talk openly about their experiences pre-COVID, during COVID, and post-COVID surge. Interviews lasted between 10 and 15 min with each participant, and each participant received a $20 gift card to acknowledge their time. To maintain confidentiality, only the interviewers had access to the data.
Rigor
The study was conducted with a research protocol reviewed and followed by the investigators. The investigators included three Ph.D. nurses working in academia and one clinical nurse specialist in a step-down unit in a tertiary hospital. The investigators followed a script and conducted the semi-structured interview bias free by examining and addressing their biases before the interview. During the interviews, at least two investigators were present; each transcript was reviewed by investigators independently for accuracy. At the end of the interview, the investigators allowed the participant to reflect on the interview to warrant credibility. The study utilized the Standards for Reporting Qualitative Research (SRQR) to guarantee trustworthiness. The transcript was imported into the NVivo program and coded thematically by the investigators. The investigators used the codebook for both inductive and deductive analysis. The research team met regularly to review coded excerpts and develop themes collaboratively.
Ethical Considerations
The university Institutional Review Board reviewed and approved all study procedures to protect human subjects. The study details were provided to the participants, including assurance that participation in the study was voluntary and that they had the right to withdraw at any time during their participation. Consent forms were emailed to participants and returned to the researcher either in person or via email prior to the initiation of the scheduled interview. Confidentiality of the collected data was maintained.
Data Analysis
The data analysis was conducted using the interpretative analysis approach. Interviews were transcribed verbatim and next organized and analyzed using the NVivo program. The investigators reviewed the transcription analyses for common themes and concepts. The thematic analysis examined the meaning of the experience operating within the societal influence (Braun & Clarke, 2006). The themes are represented through an inductive analysis dependent on the providers’ context. This analytical approach is a process where data is coded without trying to fit it into a pre-existing template or preconception of the researcher (Braun & Clarke, 2006). It is consistent with the purpose of the study to explore and richly describe the effect of the COVID-19 pandemic on nurses and respiratory therapists in Southern California with a low level of abstract interpretation (Vaismoradi et al., 2013). The research team met regularly to review coded excerpts and develop themes collaboratively. After highlighting key concepts and words from each interview, six primary themes emerged: (a) the work–life experience before the COVID-19 pandemic, (b) the work–life experience during the COVID-19 pandemic, (c) the personal life experience during COVID-19, (d) the coping period, (e) professional role change, and (f) the work and personal life experiences post-COVID-19 surge (Table 1). For this study, data saturation was evident when no new information was discovered in data analysis, signaling that data collection may cease after interviewing 13 participants.
Examples of Primary Themes and Meaning Units.

Note. COVID-19, SARS-COV-2; P : Participant.
Results
Participant Characteristics
Participants were evenly distributed, registered nurse (n = 7, 53.8%) and respiratory therapist (n = 6, 46.2%). Two-thirds (n = 8, 66.7%) reported race/ethnicity as White, one Asian (8.3%), one non-Hispanic Black (8.3%), and two Pacific Islanders (16.7%); one no response. The mean age was 40.25 (SD = 9.86, range 28–60 years); three quarters, 76.9% (n = 10) self-identified female; 7 (53.8%) reported having an associate degree, 6 (46.2%) a bachelor's degree (46.2%), 100% were employed full-time, with 11 (84.6%) staffing the day shift. Six nurses worked in the step-down intensive care unit (ICU), one in the emergency department (ED); respiratory therapists worked in ICU, ED, step-down ICU, and medical-surgical units. Regarding social history, 8 reported drinking alcohol 1–3 time a week (valid percent = 61.5%), with 5 no response; 11 denied smoking or vaping. Nine (81.8%) reported their primary support was a spouse or a family member, and two (18.2%) indicated friends provided immediate support (Table 2).
Participants’ Sociodemographic Characteristics (N = 13).
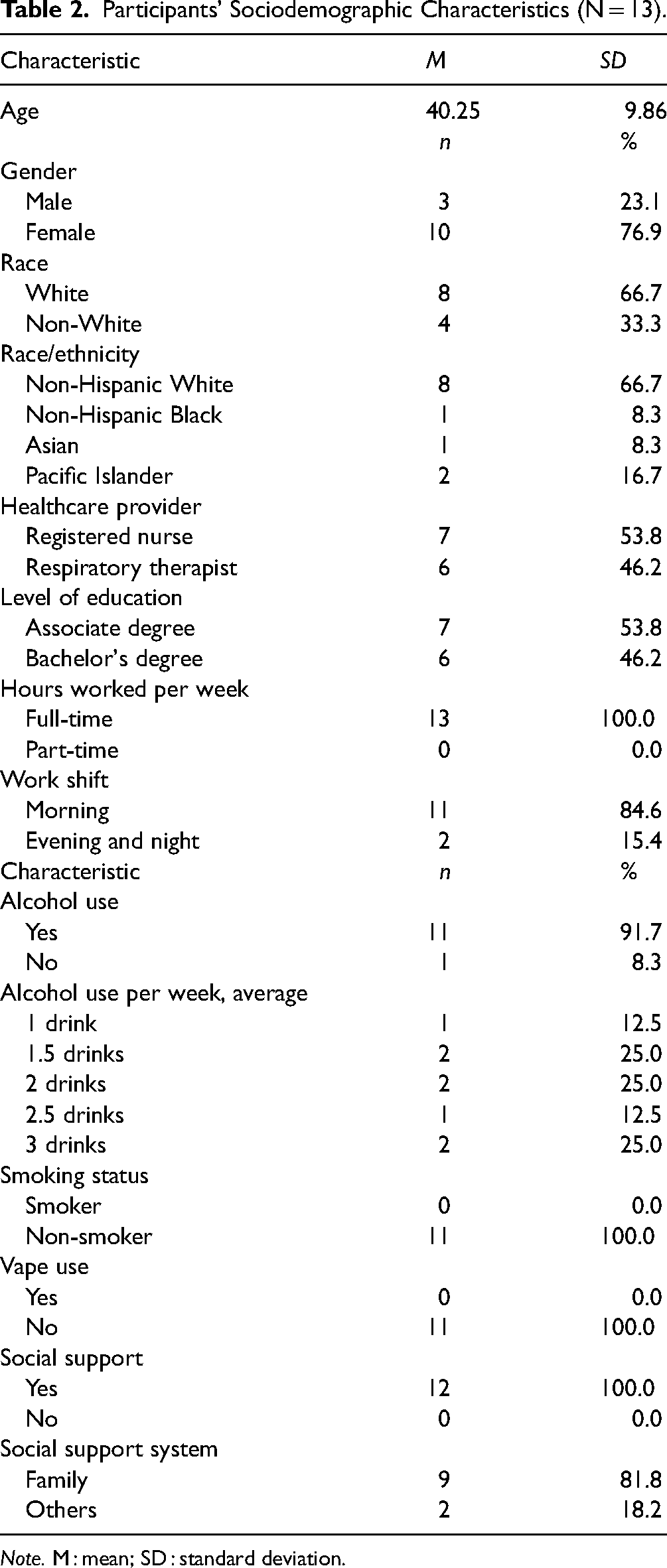
Note. M : mean; SD : standard deviation.
Thematic Findings
The Work–Life Experience Before the COVID-19 Pandemic
Participants enjoyed work life and liked what they did before the pandemic. Pre-pandemic, participants had a satisfying work–life balance. They described their life as less hectic, spent more time with family, socializing more, and were able to handle the patient load. I socialize with friends, family, and co-workers. Yes, I enjoyed life before COVID-19 since I am a people person. (Participant 1)
Yeah, I love going to work every day and I didn’t have anxiety going to work every single day. (Participant 2)
The Work–Life Experience During the COVID-19 Pandemic
Participants described their experience as stressful, caring for critically ill patients, and busy. The participants with hectic and stressful work described their environment as chaotic, short of staff, and faced with difficult life-and-death decisions, which made some afraid and unhappy. Both intense emotions and physical exhaustion led to their loss of compassion. The increased number of high-acuity patients fueled a high-stress environment with minimal supplies and special devices to treat patients. Feelings of stress, anxiety, fear, suffocation, and sadness were expressed. Working during the pandemic, it's just extremely stressful you know, we had no idea what to expect walking into work, or whether we’re going to be out of ratio. (Participant 2)
It was just going in just not knowing what was going to happen, I think, just the stress level was just off the charts and even being there and how critical patients were intubating patients left and right every day. It definitely took a toll. I definitely felt anxiety all the time. (Participant 5)
Suffocating really. Walking into work, we were overwhelmed with COVID patients, to the point where ICU took over our floor. We took over another floor or we were spread out in my particular unit, and we were spread out between other floors and floating everywhere, just to accommodate the patients. (Participant 4)
During the peak of it, it was scary because it was kind of unknown and then everything, I learned prior was kind of thrown out the window because we weren’t treating the patients like we would normally treat them. Nobody knew what was going on with the virus, therefore patients that were in respiratory distress, we weren’t doing nebulizer treatments, because they were afraid that the particles would spread in the air. (Participant 11)
Other comments include off-nurse-to-patient ratio, short staff, isolated, scared, sadness, loss of humanity, hard, unpredictability, still adjusting, chaotic, hectic, and there was better teamwork from the entire healthcare team. Healthcare providers expressed experiencing difficulties caring for sick patients, the hectic work environment, and the demand for increased working hours. During the pandemic's peak, limited treatments were available, and many patients died from COVID-19. The unpredictable and chaotic environment was challenging. It was very, very chaotic, unpredictable, and stressful when the pandemic first hit. It was very heartbreaking to see a lot of elderly patients come in who did not have any means of really fighting off COVID-19 infection. So, it was pretty sad, especially seeing family members dealing with them who could not go in and see their fellow family members. So, it was pretty stressful. (Participant 13)
They also had doubled up rooms, and they had to take over another unit. So, it was just a very large volume, very sick patients, and we did go off ratio at some points, so the nurses would have four patients instead of three, which is extremely rare for us to do here in a crisis emergency. Would that ever happen? And it did, and we doubled up our room. So, it was a very hectic time trying to care for all of these patients. (Participant 7)
Personal Life Experience During COVID-19
Participants emphasized the effect of COVID-19 on their everyday lives. They described their experience with COVID-19 as isolating, changed, having feelings of anxiety, coping difficulties, sleeping problems, physical exhaustion, frustration, depression, intense emotions, fear, and post-traumatic stress. Their descriptions of busy schedules, the restrictions during the pandemic isolated them from family and friends, the fear of giving COVID to loved ones, visitation restrictions, and the nurses being at the bedside to comfort patients who were sick and dying were factors that made their everyday lives difficult. Everything that goes on in the world, and just appreciate my life in general. I was healthy, and I was able to be out there in the medical profession and helping people. But it was pretty stressful. (Participant 13)
It definitely took a toll, again, like I mentioned earlier, anxiety. Even now, sometimes you get that very sick COVID patient and just the anxiety from it and feeling helpless, and I’ve been able to help them. I find myself taking it home quite a bit, especially with those cases where you make a connection with the patient. I have seen every single patient that I know critical that I have had to intubate that I knew didn’t make it. I have them ingrained in my head. You always wonder if there was something more that you could have done to help that patient. I feel like I do have, like many others, some post-traumatic stress from this pandemic for sure. (Participant 5)
Coming home pretty emotional at times and exhausted, and pretty much stripping down showering and crawling into bed and doing it all over the next day, and then not being able to get out or see other people, it's just us, our puppy dogs and not much. (Participant 3)
I spoke to my doctor. I had trouble sleeping. I just had dreams coming to work and I never knew I had anxiety until I saw a psychiatrist. I had trouble sleeping for about two weeks, especially during the peak. I was not sleeping at all, because of post-traumatic stress and the anxiety of work life. It was kind of crazy. (Participant 10)
Coping Period
Self-care. Participants described their self-care strategies and methods, including talking to colleagues and family members, participating in activities outside work, physical activities, staying calm, having a positive attitude, and socializing more. They found ways to deal with stress and fear congruent with their needs. Healthcare providers often neglect self-care. The pandemic taught new ways to care for self to help get through a stressful event. Caring for sick and dying patients made it difficult for nurses and respiratory therapists to think about themselves; instead, they put their time and energy into helping their patients feel comfortable. Self-care is a skill many providers must learn; without the knowledge and willingness to commit to self-care, burnout and secondary stress may ensue. Eventually, some adjusted to the pandemic, while others were still struggling with it. Well, it's something we work through. I’ve learned to do more self-care and. I learned to talk to people and learn to manage to get through that, so it has ups and downs. (Participant 5)
I think, for us to cope with the stress or the pressure we like to work out so we’d go to the gym if I needed to take a mental day from work, I just would utilize the paid sick day. That kind of stuff just kind of stays away from it for a day. (Participant 11)
I need to just usually just take a few minutes kind of away from it all, to gather my thoughts and take deep breaths and triage in my head what I need to do next. But yeah, I need a little bit of time to myself, just to gather my thoughts when it's super stressful. (Participant 7)
Well, I tried to run, I mean we all have always had a lot of stress in the emergency room. And we’ve had flu seasons that have been just as busy, as we saw with COVID, so I think just my spouse is an RN so somebody to come home and talk to about it and try to keep exercise running seems to help me quite a bit. (Participant 12)
Professional Role Change
Participants endorsed that they needed more appreciation and more organizational support. They described their professional role change as professional growth, content, trouble with patients’ family interactions, much appreciation from colleagues, learning a lot, role recognition, and considering a different profession. Participants felt they did their best in the situation, and the lack of organizational support made it more difficult to appreciate their role. Those who thought the stress was too much considered a career change. Nurses and respiratory therapists experienced the pressure and burden of caring for sick patients during the pandemic with limited staffing and a lack of personal protective equipment and medical supplies. They identified a need for greater support from management during these stressful times. Despite the stress, fear, anxiety, and lack of organizational support, they continued in their profession. I feel like we have made a great impact in the field at the beginning of the pandemic, they were calling us healthcare heroes. However, what I’ve noticed as of lately is, it feels like people are getting very aggressive towards nurses. I don’t know where it came from, but I guess it's just because they’re not able to visit their family members. (Participant 5)
I don’t feel much more appreciated, honestly, like I hate to say it, but I don’t feel like anybody should give me a gold medal because I signed up for this job, knowing that there is a chance that something like this would happen. (Participant 8)
The Work and Personal Life Experience Post-COVID-19 Surge
Participants describe their post-COVID-19 experiences as normal and less isolating, especially after the vaccine was available to the public. They were less anxious, fearful, and exhausted, had difficulty coping, less stressed, guilty, relieved, happy, and had better colleague relationships. Few expressed that their experiences mostly stayed the same. The experience with the pandemic made them better healthcare providers, and they were less worried about it because fewer patients were critically ill. Their experience working with COVID-19 patients prepared them to treat patients appropriately. I did feel my anxiety go down a little bit, and stress levels go down a little bit. But, of course, the surge went back up, so it's just a matter of going up and down for me. It still kind of affected me after the surge just thinking because, for me, I feel guilty not being able to help those patients that we weren’t able to help, so it's always that what if. But then it's realizing, I did everything that I could, everything in my power to do what I could do. (Participant 5)
It changed a little. I mean not a little, but I still do get anxiety coming into work, at times, but I feel like the pandemic taught us how to become better providers. I’m not stressed, because I was put in emergent stressful situations, and I feel like by being put in those kinds of situations, they just made me better my assessment skills, they just made me a better respiratory therapist. (Participant 10)
A conceptual research framework emerged from the collected interviews (Figure 1). In the analysis of the collected data, we found concepts of change in the work environment, emotional turmoil, and self-care. Nurses and respiratory therapists who participated dealt with ethical dilemmas during the pandemic. During the pandemic's peak and visiting restrictions, they comforted many patients who could not be with loved ones, developing a rapport with their patients. The nurses and respiratory therapists were faced with the fear of getting COVID. However, many continued to care for patients and saved lives. The changes in their work environment, unknowns about the pandemic, and lack of organizational support led to emotional turmoil. The healthcare workers who participated in some self-care eased their coping with the work stressors.
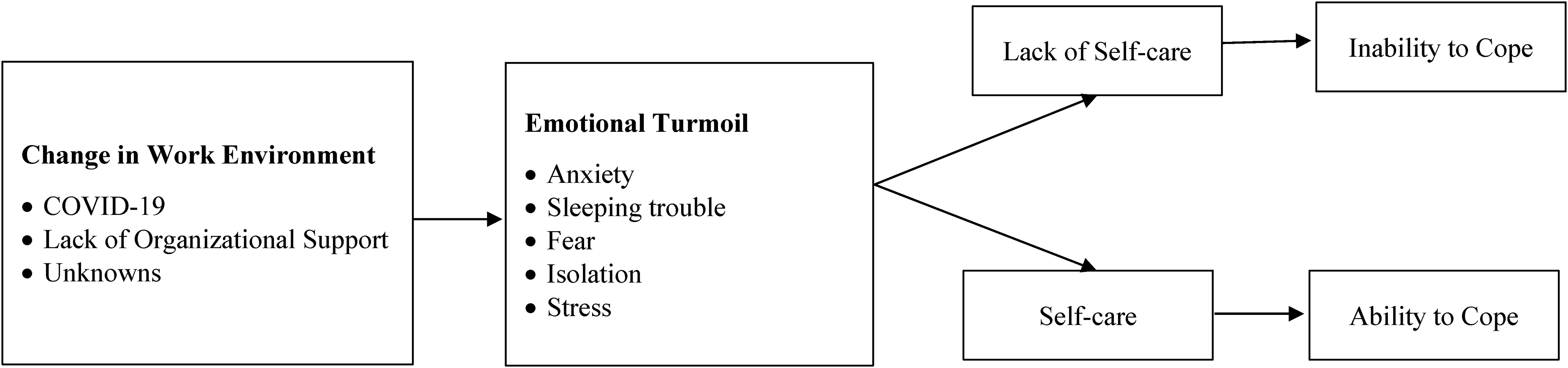
COVID-19 impact on work environment and quality of life among registered nurses and respiratory therapists: Research conceptual framework.
Discussion
In this study, we explored the lived experience of the effect of the COVID-19 pandemic on nurses and respiratory therapists in Southern California, experiences of distress, and strategies for coping with stress and loss experienced during the pandemic. Findings inform and understand the implications of change in the work environment, lack of organizational support, and unknowns about the pandemic can lead to burnout, anxiety, and secondary traumatic stress.
This study identified concepts of the impact of the work environment on healthcare providers and quality of life, which are similar to a previous study (Latsou et al., 2022). All participants verbalized that changes in the work environment influence their work and personal life. Although these findings were similar to previous studies, to our knowledge, it is only the second study to examine the pandemic's impact specific to nurses and respiratory therapists, specifically in Southern California. Participants in this study enjoyed working pre-pandemic. Nonetheless, changes in the work environment during the pandemic significantly impacted their lives. Latsou et al. (2022) and Niu et al. (2022) findings suggested that the effects of COVID-19 in the work environment increased burnout and secondary stress among healthcare providers. Ardebili et al. (2021) reported similar findings about fear, high-stress levels, and anxiety among the participants during the pandemic. Excessive work demands with inadequate resources can lead to moral distress. Findings in the study reported here are similar, and participants experienced extreme work demands leading to emotional turmoil, lack of self-care, and moral distress.
The nurses and respiratory therapists who participated in the study reported having a calling to their profession and enjoyed their job before the pandemic. Nurses and respiratory therapists mostly worked to care for patients at the bedside. Consequently, during the pandemic, they expressed similar experiences; working together to care for patients, that is, turning and positioning, assessing respiratory care needs, assisting with managing patients on mechanical ventilation, and “proning” patients to help with their breathing. Ultimately their work–life balance during the COVID-19 pandemic was disrupted. Participants worked many hours in response to increasing workload demands and had limited social interaction due to the COVID lockdown. They spent most of their working hours dealing with patients and families. The lockdown kept family members from seeing their loved ones who were dying. The healthcare workers comforted patients while communicating with family members via telephone or video call. Many hospitals could not secure enough personal protective equipment at the pandemic's beginning due to short supply and high demand. Hospital administrators were faced with short staff and requests from staff for support (Shin & Yoo, 2023). The unfamiliar work environments with increasing work demand and fear of getting COVID and giving to their loved ones made it difficult for healthcare providers to balance work and personal life. It supports the findings of Ayar et al. (2022), who identified gender, work addiction, people they live with, and working hours directly affecting healthcare professionals’ mental and work–life balance in Turkey. Participants living with more people experienced decreased work–life balance and increased mental health needs (Ayar et al., 2022); most identified their colleagues as their primary support system during the pandemic.
Munawar and Choudhry's (2021) study findings implied some of the healthcare workers’ coping strategies during the peak of COVID-19 were media exposure constraints, avoiding discussing work responsibilities with others, and prayers. One central theme in their study was frustration with public noncompliance and denial of religious scholars. In contrast to the study reported here, spiritual practices did not influence coping strategies; instead, they are influenced by talking to colleagues. Their coping strategy may differ due to cultural and governmental influences. The participants in this study questioned their desire to continue with their profession due to stress and burnout. It was reflected in the study by Ardebili and colleagues (2021), who found that despite improving knowledge and experience during the pandemic, most healthcare professionals would like to return to their pre-COVID life. Some considered leaving the profession, but most continued. In this study, participants individualized coping strategies to address their stress. Nonetheless, others were not successful in managing their mental health.
The last theme emerging from this study was the workand personal life experiences post-COVID-19 surge. As the world continues to post-COVID life, only a few studies examined post-COVID-19 life among healthcare workers. In this study, the participants were relieved when there was a decrease in hospitalization and deaths from COVID-19. Despite spreading false information about the vaccine, many people chose to get the vaccine (Loomba et al., 2021), reducing the death and hospitalization rates and, thus, reducing the work demands among healthcare providers. Unique to the study presented here, all participants enjoyed work–life balance pre-pandemic, yet they experienced emotional turmoil during the surge of COVID-19. These experiences have yet to be examined due to many unknowns about the pandemic.
Limitations and Strengths
The nurses and respiratory therapists were similar in age, education level, and employment status, which supports that both groups were exposed to similar stressors at one point. Future research is needed to look into this population regarding the impact of COVID-19 on healthcare providers in the United States. Most studies were conducted with physicians and internationally. Findings from this study add to knowledge regarding COVID-19's effects on healthcare and providers.
The findings of this study must be considered in the context of the study's limitations. Although there was adequate sampling to reach saturation, participants were a purposefully selected sample composed only of nurses and respiratory therapists with direct patient care during the pandemic. While the results of this qualitative research are not generalizable to the broader population, they may be transferable to practitioners in a similar context (Ritchie & Lewis, 2003). Future studies should focus on the COVID-19 pandemic effect, self-care, and quality of life in a larger sample size. It should also include other healthcare providers to understand their experiences. Due to the pandemic restrictions during data collection, the investigators conducted virtual interviews, limiting the ability to observe participants face-to-face. Steps were taken to ensure the trustworthiness of data collection and analysis. The analysis included all the collected data, and examples of the analysis process and quotations from the transcripts were presented. The investigators conducted the semi-structured interview bias free by examining and addressing their biases before the interview. They followed a strict protocol for data validity, with at least two investigators present during the interview and/or transcription review to assess the biases. Data analysis was conducted using the interpretative analysis approach, where data is coded without trying to fit it into a pre-existing template or preconception (Braun & Clarke, 2006). The research team met regularly to review coded excerpts and develop themes collaboratively. Consequently, the findings add to the body of knowledge on the participants’ experience of COVID-19 to our understanding.
Implications for Practice
This study examined nurses’ and respiratory therapists’ experiences during the COVID-19 pandemic. We understood that self-care was not a priority for some healthcare providers regardless of the stress they experienced at work and personal life. The results suggest the participants had difficulty with work–life balance, which may have contributed to their ability to cope and commit to self-care. The emotional turmoil they experienced during this time led to burnout, compassion fatigue, and secondary stress. The knowledge gained from the present study impacts further research in this population, addressing their mental health needs and commitment to self-care. Healthcare leaders can assist nurses and respiratory therapists in adressing organizational and community needs. Thus, the study contributes to knowledge of improving their quality of life and preventing burnout, compassion fatigue, and secondary stress trauma.
Conclusions
The results revealed the challenges nurses and respiratory therapists experienced during the COVID-19 pandemic. We gained a deeper understanding of the participants’ vulnerability in balancing work and life during the pandemic. The knowledge gained from this study can help improve understanding of the professional quality of life during the pandemic and encourage professionals to seek help and practice self-care. The study also improved our understanding that they live in a balancing act and may need organizational and community support. The lack of self-care for healthcare professionals may lead to burnout and secondary traumatic stress. Future research should focus on the professional quality of life and self-care to fully understand the impact of the COVID-19 pandemic on healthcare professionals.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding support from the University of San Diego School of Nursing Faculty Research Initiative Grant.
Ethical Considerations
The University of San Diego Institutional Review Board (IRB) reviewed and approved all study procedures to protect human subjects (IRB# 160111).