
Abstract
Introduction
Japanese men with type 2 diabetes mellitus (T2DM) usually encounter work-related difficulties when engaging in dietary modifications. Hence, healthcare providers must understand the psychological factors, such as the needs and goals, that motivate them to engage in dietary modifications.
Objective
We aimed to describe the psychological factors motivating male Japanese workers with T2DM to engage in dietary modifications.
Methods
Using a qualitative descriptive design, we conducted semi-structured interviews with 11 male Japanese workers with T2DM and identified categories based on semantic differences using qualitative content analysis.
Results
The following eight categories emerged: (I want to) demonstrate my skills at work, be able to engage in dietary modifications on my own, avoid unpleasant symptoms caused by eating, avoid burdensome treatment, maintain my healthy life, get positive results in medical examinations, maintain my relationships with others, and enjoy healthy food.
Conclusion
The factors motivating the participants to engage in dietary modifications were realistic and sincere desires rooted in their ideal lives. Their desire to prioritize work emerged as an important factor. Healthcare providers should identify an individual's ideal daily life, including work aspects, and encourage individuals to set realistic and valuable goals.
Introduction
Diabetes is a major health issue worldwide, including in Japan (International Diabetes Federation, 2019). Although dietary modifications are necessary to treat diabetes (Evert et al., 2019), individuals with type 2 diabetes mellitus (T2DM) in the workforce face conflicts between work demands and diabetes self-care, including challenges in timely food consumption (Cleal et al., 2019). Japanese men with T2DM tend to be more concerned about career performance than do their female counterparts (Tsutsui et al., 2016); therefore, Japanese men with T2DM in the workforce may experience greater work-related challenges in making dietary modifications than do Japanese women with T2DM. However, no effective support for their dietary modifications has been established. In the face of such difficulties, Japanese men with T2DM in the workforce engage with dietary modifications in their own way, such as finding strategies that do not conflict with their valued lifestyle elements like work, implementing plans strictly and patiently if the social environment is supportive, and evaluating meal choices based on objective or subjective evaluation criteria (Morinishi et al., in press). To establish support for their dietary modifications, healthcare providers must understand why Japanese men with T2DM in the workforce engage in dietary modifications despite difficulties unique to workers.
Review of Literature
Despite their difficulties and struggles with dietary modifications, recommendations for balancing work and treatment in workers with T2DM focus only on coordination of hospital visit time, management of blood glucose monitoring and insulin therapy, and management of hypoglycemia (American Diabetes Association [ADA], 2014; Japan Organization of Occupational Health and Safety, 2017).
When healthcare providers support dietary modifications in people with T2DM, it is necessary to consider their needs and goals to create a tailored support plan ( ADA, 2023b). Thus, to provide effective dietary modification support for people with T2DM in the workforce, healthcare providers must understand the psychological factors, such as the needs and goals, that motivate people with T2DM to engage in dietary modifications.
In studies involving individuals recently diagnosed with T2DM, it was observed that the main motivational factors for making lifestyle changes, particularly dietary modifications, were driven by external sources. These external factors included feelings of food restriction and the incentive of preventing a worsening of their T2DM (Sebire et al., 2018). However, these findings are not sufficient to establish tailored support for Japanese men with T2DM in the workforce because these studies included only newly diagnosed patients and deductive analyses and did not focus on employment status, gender, or national culture. Therefore, this study aimed to describe the psychological factors that motivate Japanese men with T2DM in the workforce to engage in dietary modifications.
Methods
Design
A qualitative descriptive design was used in this study, which aims to provide a comprehensive summary of an event in everyday terms. This design is suitable when straightforward descriptions of phenomena are desired (Sandelowski, 2000). We used this design to describe psychological factors that motivate dietary modifications in participants’ daily lives from their perspectives.
Research Question
The research question was, “What are the psychological factors that motivate Japanese men with T2DM in the workforce to engage in dietary modifications?”
Sample
Using purposive sampling, we recruited participants from a diabetes outpatient department at a university hospital from August to December 2019. The participants in this study were the same as those in the previous study that described actual dietary modifications (Morinishi et al., in press) because identifying what dietary modifications were made by the participants and subsequently conducting in-depth interviews about the reasons for such behaviors may be necessary to identify psychological factors motivating dietary modifications. The attending physician introduced the study to patients meeting the criteria during their outpatient visit. For those who expressed a willingness to hear a detailed explanation, the first author explained the study and obtained consent. The sample size for qualitative research should be small enough to permit deep and case-oriented analysis and large enough to provide a new and richly textured understanding of experience; hence, a sample size of 10 may be considered adequate for certain types of homogeneous case sampling (Sandelowski, 1995). Therefore, while targeting approximately 10 participants, we began recruiting participants and concurrently analyzed the data and concluded participant recruitment when we judged that the results were useful for understanding other similar cases.
Inclusion and Exclusion Criteria
Japanese men in the workforce, aged 20–65 years (because the age of adulthood and retirement at the time of recruitment was ≥20 years and 65 years, respectively, in Japan), who visited their physicians regularly for T2DM and were able to speak Japanese were included in this study. Exclusion criteria were a diagnosis of cognitive impairment and/or psychiatric disorders, being deemed by the attending physician to have difficulty speaking about the purpose of this study, and having a prescription of a diet plan for a disease other than T2DM.
Ethical Statements
This study was approved by the Kyoto University Graduate School and Faculty of Medicine Ethics Committee on July 12, 2019 (approval number: R2030). With the explanatory document, the participants were verbally informed of the details of the study, expected risks and benefits, and their right to withdraw at any time. Written informed consent was obtained from all participants.
Data Collection
Demographic data were collected by asking participants to complete a questionnaire and by referring to their medical records. Narrative data were collected through semi-structured interviews conducted in a private room within the hospital. The first author, a female nurse who was not involved in the usual care of the participants, conducted all interviews. An interview guide based on questions that facilitated reflection on the participants’ actions and underlying needs (Korthagen, 2010) was used during these interviews. After initially asking, “What dietary modifications are you engaging in?”, which is what the previous study (Morinishi et al., in press) aimed to describe, the interviewer asked them, “Why do you engage in that behavior?”, “What were you thinking and feeling at the time?”, or “What were your hopes?” The interviewer also asked them about their situation and life background when they engaged in the behavior. Each interview lasted for approximately 30–60 minutes. When needed, follow-up interviews were conducted to ask participants additional questions or confirm the meaning of narratives. All the interviews were recorded using voice recorders.
Data Analysis
Demographic data were described by counting the number of people in each category of characteristics. Narrative data were analyzed using qualitative content analysis. This method facilitates the subjective interpretation of the content through a systematic classification process with attention to the text's contextual meaning (Hsieh & Shannon, 2005). We used this method because we aimed to describe subjective content that was still unclear from the participants’ narratives while emphasizing the participants’ values or contexts. The procedure was based on Graneheim and Lundman (2004): (1) the audio recorded data were transcribed verbatim; (2) data were read several times to obtain a sense of the whole; (3) text related to the purpose of the study was extracted, including participants’ background and meanings of narratives as meaning units; (4) meaning units were condensed while retaining the core meaning, abstracted, labeled for meaning, and referred to as codes; (5) codes were compared based on differences and similarities and sorted into subcategories; and (6) subcategories were sorted into categories in the same way. The analysis proceeded concurrently with data collection and was revised based on the newly obtained data. We used NVivo11 (QSR International, Melbourne, Australia) to code the data.
Rigor
To ensure the trustworthiness of the study (Lincoln & Guba, 1985), the following procedures were conducted. (1) To ensure credibility, the meaning of the participants’ narratives was confirmed in a follow-up interview; two researchers independently analyzed the data, disagreements were resolved through discussion, and three participants validated the results. (2) To enable readers to judge transferability, the study's procedures and participants’ characteristics have been described in detail. (3) To ensure dependability, the method used in this study is described in detail. (4) To ensure confirmability, the method of this study was decided through discussion with researchers who have experience in qualitative research, and the analysis was conducted while examining the raw data.
Results
Sample Characteristics
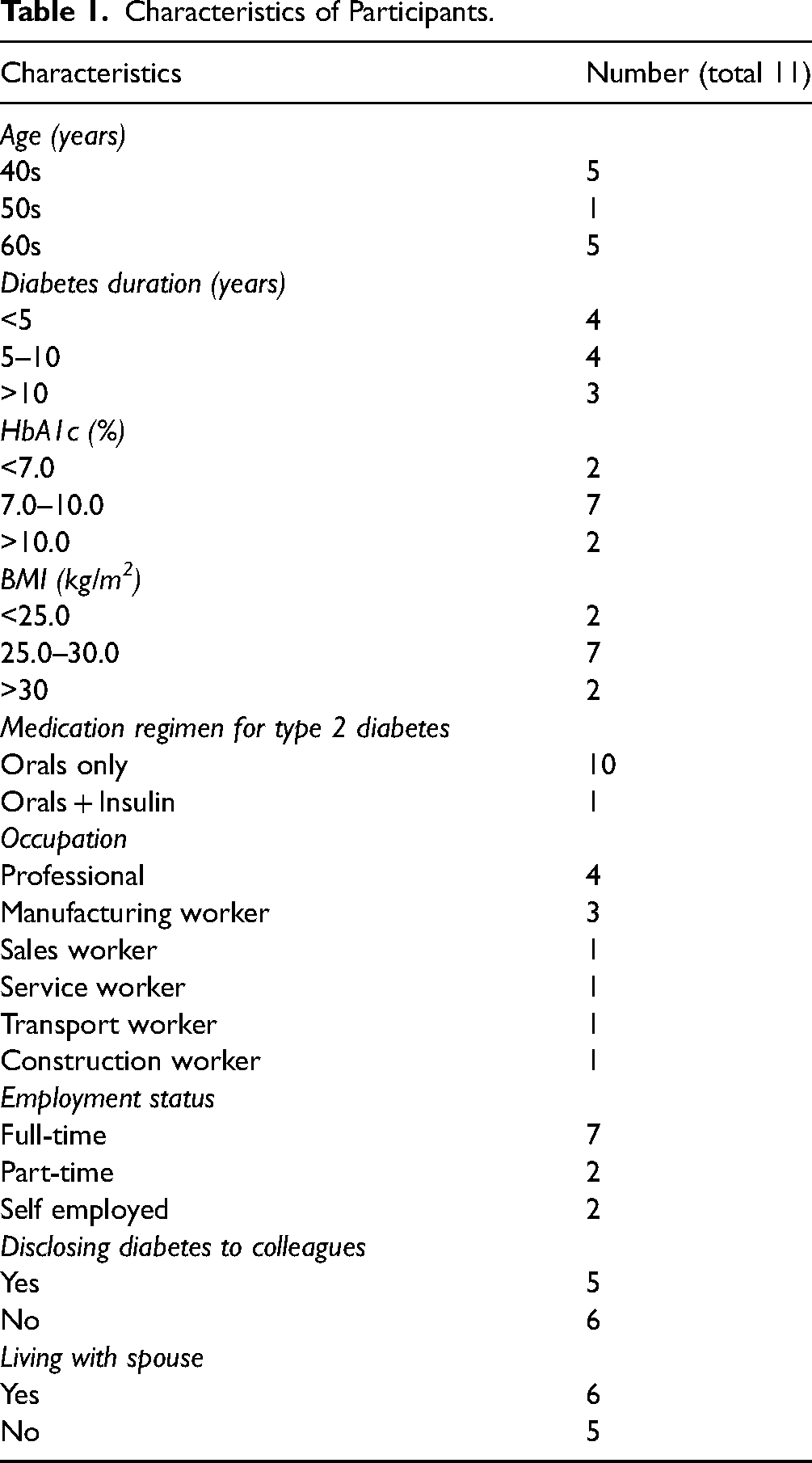
Eleven Japanese men with T2DM in the workforce participated in this study. Participants’ characteristics are presented in Table 1. Details of each participant are documented in a previous report in Japanese (Morinishi et al., in press).
Characteristics of Participants.
Research Question Results
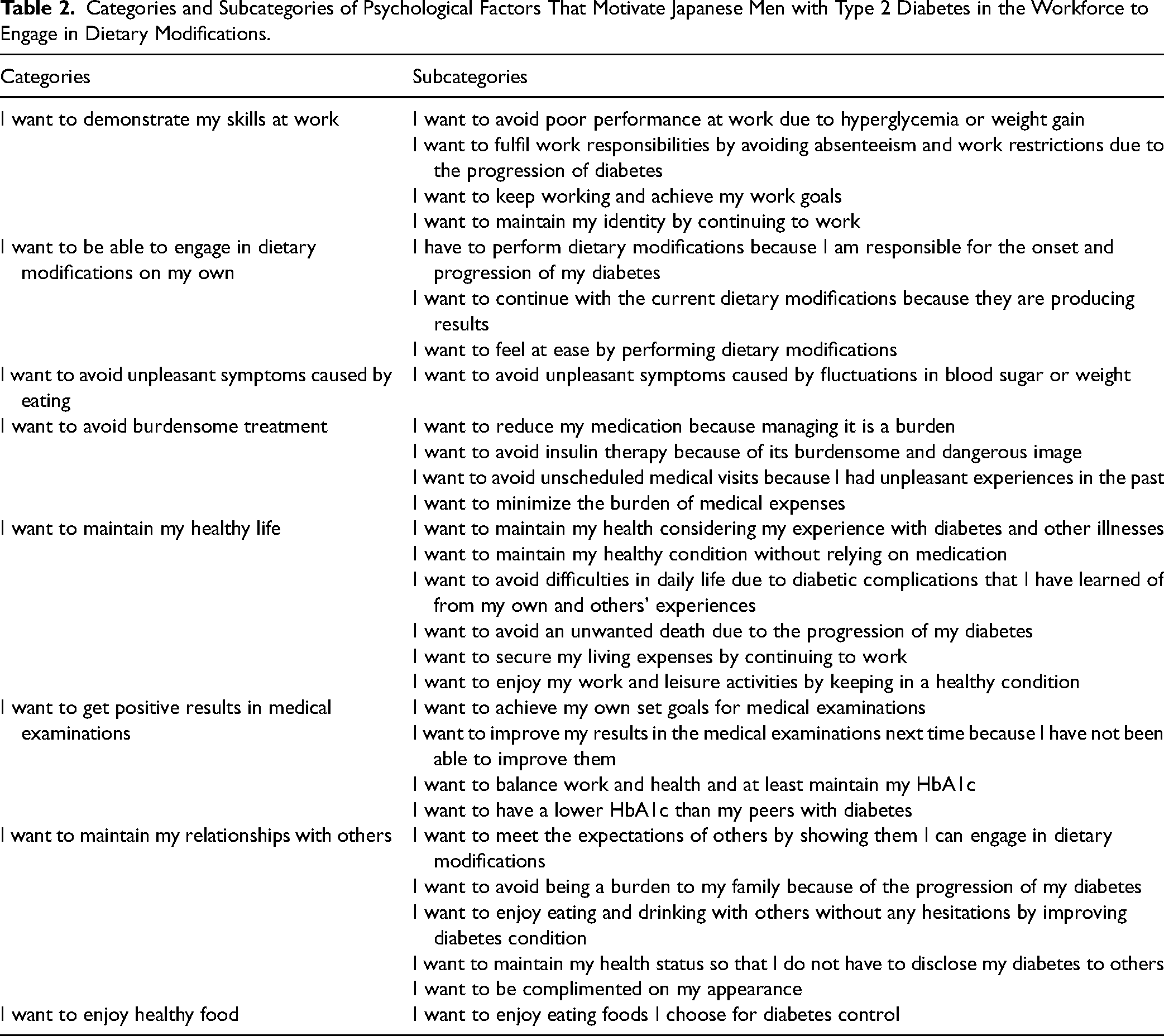
A total of 206 codes, 28 subcategories, and 8 categories emerged from the data analysis of psychological factors that motivate participants to engage in dietary modifications. Table 2 presents the categories and subcategories. Below, the categories are shown in bold, and the representative narratives are shown in italics. In parentheses after the narratives, the participant's ID, age, and occupation are shown.
Categories and Subcategories of Psychological Factors That Motivate Japanese Men with Type 2 Diabetes in the Workforce to Engage in Dietary Modifications.
I Want to Demonstrate My Skills at Work
The participants reported that maintaining their physical condition by engaging in dietary modifications was necessary to continuously demonstrate their skills at work. I knew that gaining weight would make me tired when I was working. This affects the quality of the work. (Participant B, 40s, Professional).
I do not want to be hospitalized (due to worsening diabetes control). I cannot take a day off from work. (Participant C, 40s, Professional)
I Want to be Able to Engage in Dietary Modifications on My Own
Because participants felt remorse for the onset or progress of diabetes and experienced positive results from dietary modifications, they found value in engaging in dietary modifications by themselves. (After being hospitalized for diabetes educational admission) I finally realized that my usual eating behaviors are absolutely inappropriate. (omission) I told my wife that I don’t need her support for my diet. (omission) It's all my own responsibility. (Participant J, 60s, Transport worker)
I Want to Avoid Unpleasant Symptoms Caused by Eating
Participants experienced unpleasant symptoms associated with eating; therefore, they engaged in dietary modifications to avoid these symptoms. When my blood sugar level is low, I feel fuzzy or lifeless. I feel better when my blood sugar level reaches 130 (mg/dL). On the other hand, when my blood sugar rises higher than that, I feel hyper and tired. (Participant H, 60s, Manufacturing worker)
I Want to Avoid Burdensome Treatment
The participants engaged in dietary modifications because they wanted to reduce the burden of treatment they experienced daily. In addition, they feared that enhanced treatment, such as increasing the dose of medication, starting insulin therapy, and hospitalization, would increase the burden on their lives. I had a colleague who always carried the insulin device and some candies. He often said, “Oh,” and then gave himself an injection, and after a while, he also said, “Oh,” and then ate candies. (omission) It looked quite troublesome. (Participant G, 60s, Professional)
I Want to Maintain My Healthy Life
Because participants experienced the onset or progression of diabetes, diabetic complications, or other diseases, they redefined their “health.” They engaged in dietary modifications to maintain their “health.” Their definition of “health” was constructed not only by their own experiences but also by images generated by media or others with diabetes, including their family members. In addition, their wants, regardless of whether they had diabetes, included the desire to enhance leisure activities, thereby motivating dietary modifications. It is better to be healthy for me. (omission) But there is a contradiction between wanting to be healthy and having elevated blood sugar levels. I think “healthy” for me is to be able to live a usual life. (Participant D, 40s, Manufacturing worker)
I play basketball. I cannot have fun unless my body moves vigorously. This is my motivation (for dietary modification). (Participant A, 40s, Professional)
I Want to Get Positive Results in Medical Examinations
Participants did not simply set goals based on the recommended HbA1c values to prevent diabetic complications; they set their goals based on their age, changes in their laboratory values, balance with their work, and comparisons with peers who have diabetes. Their obsession with their target values motivated them to engage in dietary modifications. I think (HbA1c) 7% would be fine if I were older. But I do not think I am old yet, so I am not sure if 7% is good enough. (Participant B, 40s, Professional)
I hope to be able to maintain (my HbA1c level while I am working overseas), but it is difficult for me. However, health comes first, right? Without my health, I could not work. (Participant C, 40s, Sales worker)
I Want to Maintain My Relationships With Others
Participants reported that engaging in dietary modifications would affect their relationships with others and how others perceived them. They believed that engaging in dietary modifications would improve their relationships. I engaged (in dietary modifications) because I was scolded (by a nutritionist). (I engage in dietary modifications) because the medical professionals work hard for me. (Participant D, 40s, Manufacturing worker)
I am hesitant to tell (colleagues that I have diabetes). If I had to take several days off, I think I would have had no choice but to tell them. (Participant B, 40s, Professional)
I Want to Enjoy Healthy Food
Because participants were able to gain pleasure by eating the foods they chose for diabetes control, they were willing to engage in dietary modifications. I like noodles, so I always eat carbohydrate-free noodles. They are delicious. (Participant A, 40s, Professional)
Discussion
This is the first study to describe the psychological factors that motivate Japanese men with T2DM in the workforce to engage in dietary modifications from their perspectives, emphasizing their values and life background.
The results showed that Japanese men with T2DM in the workforce were motivated by psychological factors related to various values in their daily lives, such as prioritizing work, their own experiences, images obtained from others, and relationships with others, to engage in dietary modifications. The finding unique to the participants of this study was that their desire to prioritize work could be a motivating factor if they perceived dietary modifications to be beneficial for their daily work; previously, such a desire was considered an obstructive factor.
Psychological Factors That Motivate Japanese Men with T2DM in the Workforce to Engage in Dietary Modifications
The first category, “I want to demonstrate my skills at work,” was a unique factor for workers. This category and the fact that these participants implemented dietary modifications, such as finding ways that do not conflict with work (Morinishi et al., in press), indicated that they valued their work, which could motivate dietary modifications. This category reflects that approximately 80% of Japanese people value work in their lives (Haerpfer et al., 2022). In contrast, in previous studies, it has been reported that the willingness to prioritize work leads to inadequate self-management among workers with T2DM (Ruston et al., 2013). This study suggests that willingness to prioritize work can not only inhibit but also facilitate dietary modifications in Japanese men with T2DM. Additionally, if the individual is aware of the beneficial effects of dietary modifications on daily work, such as the subcategory “I want to avoid poor performance at work due to hyperglycemia or weight gain,” they would be more aware of the benefits and consequently, would be motivated to engage in dietary modifications. The willingness to prioritize work can also be a motivating factor in the lives of people from other cultures who prioritize work.
The second category, “I want to be able to engage in dietary modifications on my own,” showed that participants wanted to modify their diet because of remorse related to the onset or progression of diabetes. The same remorse could also be associated with these participants’ engagement in dietary modifications, such as implementing dietary plans strictly and patiently if the social environment was supportive (Morinishi et al., in press). The remorse may be augmented by the stigma caused by diabetes; for example, people with diabetes are considered by society to be “lazy” or “overeaters” (Browne et al., 2013), and Japanese workers with T2DM perceive a stigma of being “unable to work” because of their diabetes (Nakao et al., 2015). Japanese men with T2DM in the workforce may experience stigmatization in the workplace, and the remorse generated by stigma would force them to engage in dietary modifications strictly and patiently.
The third, fourth, and fifth categories, “I want to avoid unpleasant symptoms caused by eating,” “I want to avoid burdensome treatment,” and “I want to maintain my healthy life,” were related to individual's desires to fulfill ideal lives generated by their own experiences with T2DM or by images generated by others who experienced diabetes-related burden. Previous studies have shown that people with newly diagnosed T2DM are mainly motivated to change their lifestyles by external factors, such as feeling restricted (Sebire et al., 2018). Because this study targeted a specific group, focused on participants’ values and life contexts, and performed inductive analysis, this study could identify novel factors that are more sincere and relevant to ideal daily life, as shown in the subcategory “I want to minimize the burden of medical expenses,” in Japanese men with T2DM in the workforce.
The sixth category, “I want to get positive results in medical examinations,” could be a motivating factor if participants had difficulty feeling the effects of dietary modifications internally. Actually, participants with few subjective symptoms implemented dietary modifications such as evaluating meal choices based on objective evaluation criteria (Morinishi et al., in press). In many people with diabetes, the recommended glycemic target to prevent diabetic complications is an HbA1c level of <7% (ADA, 2023c; Araki et al., 2020). However, as shown in the subcategory “I want to achieve my own set goals for medical examinations,” the participants did not simply set goals based on the recommended HbA1c values for preventing diabetic complications but set their goals based on their age, changes in their laboratory values, balance with their work, and comparisons of laboratory values with those of their peers. It has been demonstrated that rather than motivation based on external demand, motivation based on recognizing the behavior as personally important is more likely to lead to high-quality behaviors and persistence (Ryan & Deci, 2000). Therefore, when participants use objective indicators such as HbA1c as evaluation criteria for dietary modifications, they can more effectively implement dietary modifications if they set evaluation criteria based on their own meaningful goals rather than general external evaluation criteria.
The seventh category, “I want to maintain my relationships with others,” could be a strong factor for Japanese workers. One reason is that, as shown in the subcategory “I want to meet the expectations of others by showing them I can engage in dietary modifications,” Japanese people have a marked tendency to be motivated by expectations from others (Tokuoka et al., 2015). Moreover, The subcategory “I want to maintain my health status so that I do not have to disclose my diabetes to others” could relate to the stigma among Japanese workers. More than half of the participants hid that they had T2DM from coworkers because of a fear of stigmatization, such as being “unable to work” (Nakao et al., 2015). Compared to workers in other countries, Japanese workers place high importance on the evaluation of and relationships with others (Nishida & Terashima, 2019). Therefore, Japanese workers could be particularly keen to avoid stigma, which can negatively affect their evaluation and relationships with coworkers and motivate them to engage in dietary modifications.
Whereas the categories mentioned above were factors related to outcomes separate from the diet itself, the eighth category, “I want to enjoy healthy food,” was the only factor that indicated intrinsic motivation, defined as motivation by interest, enjoyment, or inherent satisfaction of the activity itself (Ryan & Deci, 2000). Conversely, in people with chronic illnesses, many self-care behaviors are driven by extrinsic motivations, that is, the motivation for predetermined desirable outcomes (Riegel et al., 2012). However, long-term healthy diet adherence is more motivated by intrinsic rather than extrinsic factors (Pelletier et al., 2004). This category suggests that if participants who implement strict dietary modifications establish ways to make them enjoyable, they are more likely to continue strict dietary modifications in the long term, driven by their intrinsic motivations.
As mentioned above, because the psychological factors shown by these categories were realistic and sincere desires based on the workers’ values or ideal lives, addressing these factors can empower individuals to engage in dietary modifications.
Strength and Limitations
The strength of this study was the description of the psychological factors that motivate Japanese men with T2DM in the workforce to engage in dietary modifications from their own perspectives, emphasizing their employment status, gender, national culture, values, and life background. As a result, the psychological factors that were the realistic and sincere desires of the workers, based on their values or ideal lives, were revealed.
This study had two limitations. First, no participants were in their 20s or 30s; therefore, these age groups could not be assessed. Second, because most participants were prescribed only oral medication, data related to insulin therapy or self-monitoring of blood glucose may be insufficient. However, we judged these results to be sufficiently useful for understanding dietary modifications in the target population.
Implications for Practice
These new findings suggest that Japanese men with T2DM in the workforce are more motivated to engage in dietary modifications by setting realistic and valuable goals in their daily lives. Setting proximal goals has been reported to be effective in ongoing endeavors because the process involves frequent feedback and is perceived to be more psychologically “real” (Bandura, 1997; Strecher et al., 1995). Based on the results in the subcategory “I want to avoid poor performance at work due to hyperglycemia or weight gain,” goals that allow the workers to feel they can accomplish their daily work could be effective. This is because this sense of accomplishment provides frequent internal feedback, and the willingness to work was potentially a strong factor in this study. Although people with T2DM at earlier stages often cannot notice the classic diabetes symptoms (ADA, 2023a), people with diabetes that is mild enough that they can work may easily perceive any discomfort or changes in performance due to weight fluctuations.
Conclusions
This study describes the psychological factors that motivate Japanese men with T2DM in the workforce to engage in dietary modifications, focusing on their values and life contexts. A total of eight categories emerged: (I want to) demonstrate my skills at work, be able to engage in dietary modifications on my own, avoid unpleasant symptoms caused by eating, avoid burdensome treatment, maintain my healthy life, get positive results in medical examinations, maintain my relationships with others, and enjoy healthy food.
Because these psychological factors were realistic and sincere desires based on the workers’ values or ideal lives, they can be enabled to engage in dietary modifications even if they are working. Also, their desire to prioritize work can be a motivating factor, whereas such desire has previously been considered an obstructive factor. Our results suggest that healthcare providers should identify an individual's ideal daily life and encourage them to set realistic and valuable goals.
Footnotes
Acknowledgments
The authors thank Ms. Wakako Kitakubo, the chief nurse of Kyoto University Hospital, and the staff of the hospital for helping with data collection. Moreover, they thank all the participants for taking time out of their busy schedule and to share interesting narratives. They would like to thank Editage (![]() ) for its assistance with English language editing.
) for its assistance with English language editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statements
This study was approved by the Kyoto University Graduate School and Faculty of Medicine Ethics Committee on July 12, 2019 (approval number: R2030). With the explanatory document, the participants were verbally informed of the details of the study, expected risks and benefits, and their right to withdraw at any time. Written informed consent was obtained from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.