
Abstract
Introduction
The medical staff involved in adverse events, referred to as second victims, usually suffer second victim syndrome endangering their health. Still, there are few organizational support projects in this area in China.
Objective
To explore the effect of mindfulness meditation on the level and needs of organizational support, and mindfulness awareness among nurses as second victims.
Methods
Forty-six nurses from a comprehensive tertiary hospital in Wuhan, China were selected to participate in the study. This study was conducted using a convenience sampling method for eight weeks of mindfulness meditation intervention. The Second Victim Experience and Support Tool and Mindfulness Attention Awareness Scale were used to assessing the need for support and mindfulness awareness of nurses prior to intervention, during the fourth and eighth weeks of intervention, and at the conclusion of the intervention course.
Results
The difference between the scores measured before the intervention, in the fourth week, and in the eighth week of intervention showed that the need for the second victim support from work-related organizations was significant (F = 34.513, p = .000); there was no significant difference in the scores related to the need for nonwork-related support of the second victim in the participating nurses (F = 1.373, p = .257); the scores of the level of mindfulness awareness were (64.85 ± 11.41), (68.63 ± 11.33), and (71.20 ± 8.41), a significant difference (F = 18.848; p = .000) was found in terms of before and after the intervention; nurses’ second victim support needs gradually shifted from evasion to confronting problems appropriately.
Conclusion
Mindfulness meditation intervention is applicable to the second victim population of nurses. It is an effective way to support second victim nurses and can effectively improve their level of mindfulness and awareness.
Keywords
Introduction
Background
Medical errors in health care negatively impact patients, medical staff, and medical institutions (Jang & Lee, 2016). The medical staff involved in adverse events, referred to as second victims (Second Victim), may be physically and psychologically traumatized, causing them to feel pain and lose confidence in their professional abilities (Edrees et al., 2016; Han et al., 2017). The second victims usually suffer second victim syndrome (SVS) featuring increased heart rate and breathing, anxiety, depression, sleep disorders, and other ailments (Zarabian et al., 2020), which may develop into severe anxiety, depression, and potential burnout and turnover (Burlison, Quillivan et al., 2021; Van Gerven et al., 2016). All of these seriously endanger the health of the second victims (Chen G et al., 2019a). Edrees et al. (2016) show that 86.3% of second victims needed to return to duty for effective organizational support within two days.
Review of the Literature
With the gradual development and expansion of organizational support projects for second victims abroad, the phenomenon of medical personnel succumbing to the aftermath of medical errors in China has attracted widespread attention. There has been an increasing number of investigations on nurse mindfulness training in China but few intervention studies. For example, one study demonstrates that mindfulness has a clear correlation between personality traits and burnout among Chinese clinical nurses (Zhao et al., 2019). These findings suggest the potential benefits of tailor-made mindfulness interventions in reducing burnout in Chinese nurses (Zhao et al., 2019). Based on Zhao's research, this study expected to confirm the impact of mindfully based stress reduction measures on the second victim group through an intervention study. Busch et al. (2020) found through a meta-analysis that the five most frequent coping strategies by second victims were changing work attitude; following policies and guidelines more accurately and closely; paying more attention to detail; problem-solving/concrete action plans and criticizing or lecturing oneself. A study confirms that these nurses may require ongoing psychosocial support during and after the pandemic (Erkin, Konakçı, & Duran, 2021). However, further clarification is needed on the impact of relevant interventions on the psychological status of medical personnel before the COVID-19 pandemic.
Purpose and Research Questions of the Study
In order to understand whether mindfulness meditation (MM) can effectively improve the level of mindfulness and awareness of the second victim group, this study conducted an intervention study with nurses as the research subjects. If the expected results of this study are achieved, it will provide a reference basis for improving the mental health of nurses.
Methods
Study Subjects
Participants were selected among volunteer nurses who encountered an adverse event from January to June 2019, and all participants signed an informed consent form. The research was consented by the Ethics Committee of a third-class A comprehensive hospital in Wuhan, the affiliation of the researchers with the approval of the ethics committee, and all participants of subjects were approved by the ethics committee. The research confirmed with the Declaration of Helsinki.
Inclusion and Exclusion Criteria
Inclusion criteria: (a) clinical nurses directly involved in patient care; (b) provided informed consent for voluntary participation in this study; (c) held a nurse's qualification certificate from the People's Republic of China; (d) faced exposure to adverse events in the past six months and for disclosure and discussion. Exclusion criteria: (a) refresher or intern nurses; (b) level IV incidents; and (c) noncompletion. Before the study was carried out, all participants were informed that they needed to commit to completing the entire intervention process and spending 20 to 30 min for self-training every day during the training course. A total of 46 subjects, 43 women and three men, were enrolled in the study.
Study Design
This study used convenience sampling to select nurses who had experienced adverse medical events within six months (from July to December 2019) as the study subjects. The researchers conducted an eight-week MM intervention on the study subjects. The Second Victim Experience and Support Tool (SVEST) and Mindfulness Attention Awareness Scale (MAAS) were used to evaluate the level of organizational support and mindfulness attention awareness of the study subjects before, at weeks 4 and 8, and at the end of the intervention course. The contents of this study include four parts: the construction of intervention courses, preparation before the intervention, implementation steps of intervention, and effectiveness evaluation.
Construction of the Intervention Course
The theoretical model of the intervention course was drafted at the “The 2017 Resident Wellness Expert Consensus Summit” in Las Vegas, Nevada on May 15, 2017. Resident participants of 31 programs participated in the “Educator Toolkit” group cooperation (Chung et al., 2018). In the seven months before the summit, the workgroup convened the Wellness Think Tank composed of emergency medicine residents from 100 different training programs from 14 organizations in two North American regions, all of whom conducted a literature review and drafted three core wellness topics curricular plans. The three evidence-based toolkits included SVS, mindfulness and meditation, and positive psychology (Chung et al., 2018). These toolkits provide educators with necessary resources, such as reading materials and training curricula, for practicing mindfulness. The MM toolkit contains four-course modules: the MM introduction course, the MM framework course, the longitudinal guided meditation planning course, and the MM inquiry and reflection course. Based primarily on the toolkits, the researchers built MM training courses, including outlines of MM training, the mechanism of MM, common practices of MM, tools related to MM, and group discussions of the experience of adverse events. The course lasted one month and was guided by two professional tutors.
Preparation Before the Intervention
The research team received theoretical and practical training in MM-related courses in the preparation stage and the course was conducted under the guidance of a qualified counselor. The researchers involved all the participants in a WeChat group set up specifically for organizing, communicating, and issuing questionnaires related to the course. Two weeks before the course, the researchers issued course notices to remind all enrolled nurses to set aside time for the training. The content, purpose, and benefits of the course were introduced to all participants so that they could fully understand and cooperate with the training requirements. The “Now Meditation” App was then downloaded to help participants finish their training at home. All participants were distributed with brochures to better understand the principle and technique of psychological intervention methods of MM and were also provided with notepads to record meditation diaries of classroom discussion, self-exercise notes, and group discussions in the eighth week. For participants absent due to special reasons, the researchers organized online training by initiating meetings through the Tencent Meeting App. The Tencent meeting applet was sent to the WeChat group so that the absent participants could identify the applet and enter the conference for online lectures through audio and video conversations and PPT lectures. The preparation phase lasted two months, including two months of training for study team members, and two weeks of a presurvey conducted for all trainees before the formal intervention.
Intervention Implementation Steps
The MM training course was composed of four-course modules, which were deepened gradually as shown in Table 1, and was carried out by two trained chief nurses. Each course consisted of two parts, each lasting approximately 30 min, and was performed once a week for eight weeks. Enrolled Nurses were gathered in the first part, which focused on theoretical lectures and on-site MM exercises. They were then divided into five subgroups which consisted of eight to nine persons for discussion and a consolidation exercise in the second part. After training, participants were required to meditate for 20 to 30 min at home every day with the help of the “Now Meditation” app and send screenshots of the practice records of the app to the WeChat group in the eight weeks. At the end of the eight-week intervention, the notepads were collected, and the participants could choose whether to record their names. The absent participants were gathered for a group study and were given the same homework.
Schedule of Mindfulness Meditation Training Course.

Effect Evaluation
The researchers took a general data questionnaire and two scales to evaluate the influence of the intervention. (a) The general information questionnaire consisted of the subject and adverse event characteristics questionnaire. The general information questionnaire designed by the researcher included the nurse's age, gender, education level, marital status, positional titles, employment forms, working department, working years, and whether they were engaged in the direct care of patients. The adverse event characteristics questionnaire included event type, occurrence time, event level, event duty, department discussion, nursing department discussion, punishment form, and support form. (b) SVEST (Burlison et al., 2014). The team of American scholars Jonathan D. Burlison and Susan D. Scott developed the scale in 2016 and officially published it in 2017 after verifying its reliability and validity. The scale included seven dimensions (psychological distress, physical distress, professional self-efficacy, colleague support, superior support, institutional support, and nonwork-related support) and two outcome variables (turnover intentions and absenteeism), for a total of 29 items. The scale was measured by Likert's 5-point scoring method, ranging from 1 for strongly disagree to 5 for strongly agree. The higher the SVEST score, the more serious the impact of the patient safety incident on the second victim's personal and career, and the less support the second victim can get. In a preliminary study by our team (Chen et al., 2019b), the researchers tested the scale and confirmed that it is reliable and valid in the second victim group of nurses with a Cronbach's α of .892. In this study, the second victim's support level and needs were measured by selecting the terms of different dimensions of organizational support (colleague support, senior worker support, and institutional support), the independent dimension of nonwork-related support, and additional items of support needs for measurement. (c) The Chinese version of the Mindful Attention Awareness Scale (MAAS). This scale was developed by Brown and Ryan to measure the level of mindfulness based on the concept of “current attention and awareness.” The single-dimensional structured scale includes a total of 15 items involving the individual's cognition, emotion, and physiology in daily life (Brown & Ryan, 2003). The Chinese version of the scale was transformed by Chen et al. (2012) and the reliability and validity of the scale were tested on college students. The Cronbach's α was .890, and the retest reliability was 0.870. The scale was scored using Likert 6-level scoring method. The total score was the sum of the 15 items’ scores. The score ranged from 15 to 90 points. A higher score indicates that the individual had higher awareness and attention being present in daily life.
Statistical Analysis
All data were reorganized in Excel and imported into a database for further analysis by the SPSS 23.0 software package. The statistical methods involved are as follows: The classification variables are statistically described by frequency and percentage, and quantitative data were expressed in the form of mean ± standard deviation. Single-factor repeated measures analysis of variance was used to compare measurement data at different time points. The variance analysis results are subjected to Mauchly's method of spherical verification. If p < .05 in the spherical test, Greenhouse–Geisser (Epsilon <0.75) or Huynh-Feldt (Epsilon ≥0.75) was used for correction.
Results
Characteristics of Participants
The general demographic information of the participants is shown in Table 2. The general data of second victims show that nurses are significantly more likely to be women than men; ages were concentrated between 20 and 30 years old; most of the participants’ educational level was undergraduate; positional titles are mainly low seniority nurses; married is about the same as unmarried within the marital status; the position is mainly general nurses; the form of employment is mainly the contract employment system; <within 10 years is common and >10 years rare within the working years; all the second victims had direct contact with the patients.
General Information on the Second Victim and Adverse Events (n = 46).

*The event level is based on Adverse Events Management Measures from Hong Kong Hospital Authority.
Pipeline events, also known as pipeline-related adverse events, include pipeline twisting, folding, detachment, displacement, scratches, and blood leakage at joints and tees.
Analysis of Adverse Events
The general data analysis of adverse events is shown in Table 2. There were 46 nurses involved in the study. The most common types of medical adverse events were nine pipeline events, accounting for 19.56%, 10 drug errors accounting for 21.73%, and 16 other types accounting for 34.78%. All adverse events included 37 level III events, accounting for 80.43%. Thirty-two nurses are the main responsible person for adverse events accounting for 69.57%, nine nurses are the secondary responsible person accounting for 19.60%, and the other five nurses are irrelevant personnel. A total of 95.65% of the adverse events were department-discussed, and 58.7% of the adverse events were discussed by the nursing department. Twenty-one nurses were punished through the deduction of bonuses, and 25 nurses were verbally criticized. All the second victims received support in different forms after the incident.
Results of SVEST
The second victim support level and each dimension score are shown in Table 3 and Figure 1. Nurses’ second victim's support level is measured by four dimensions of the SVEST scale, including work-related organizational support (colleague support, superior support, and institutional support) and nonwork-related support. The higher the SVEST score, the more severe the impact on the second victim in the adverse event, and the less support they receive. The nurses’ second victim's support score and each dimension score gradually decreased before and after the intervention, indicating the higher level of support the second victim received. Comparison between measurements at different time points was significant (p < .01) except for nonwork-related support (P = .257).

The requirements of second victims for organizational support of the three dimensions.
The Second Victim Support Level and Mindfulness Attention Awareness Level.
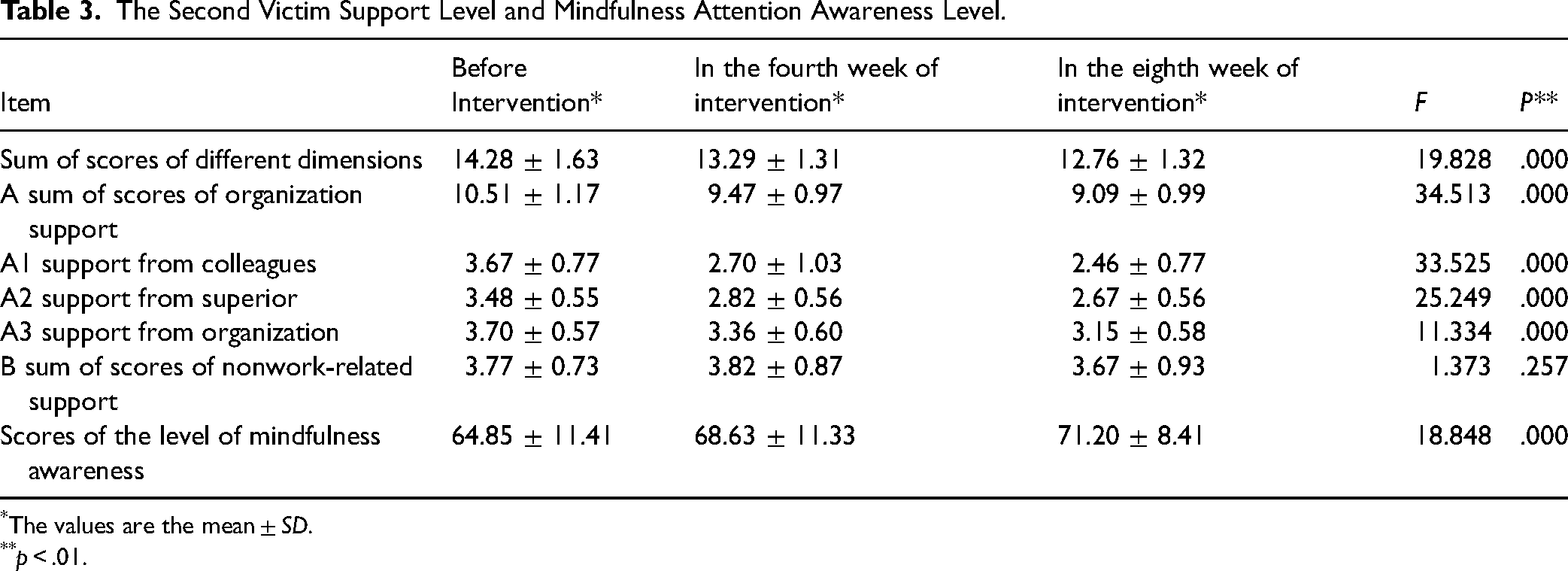
*The values are the mean ± SD.
**p < .01.
Requirements of the Second Victim Support
The second victim support requirements are shown in Table 4. The nurses’ second victim's support requirements in this study were measured by seven additional items of the SVEST scale. The results show that the top two support requirement scores before the intervention were Item 2 and Item 1. The lowest two support requirements scores were Item 7 and Item 4. After eight weeks of intervention, the ranking of requirement scores changed. The top two support requirement scores were Item 3 and Item 5. The second victim's support needs are changing over time, and requirement scores were statistically significantly different when compared between measurements at different points in time (p < .01). The results showed that after eight weeks of MM intervention, the support needs of the second victim gradually shifted from avoidance (quiet place and leave immediately) to correct handling of problems (discussing details with peers and superior supervisors).
The Second Victim Support Requirements.

Results of MAAS
The second victim's mindfulness attention awareness level is shown in Table 3 and Figure 2. The total level of awareness gradually increased before and after the intervention, suggesting that the second victim gained a stronger level of mindfulness awareness. The differences between the measurements at different time points were statistically significant (p < .01).
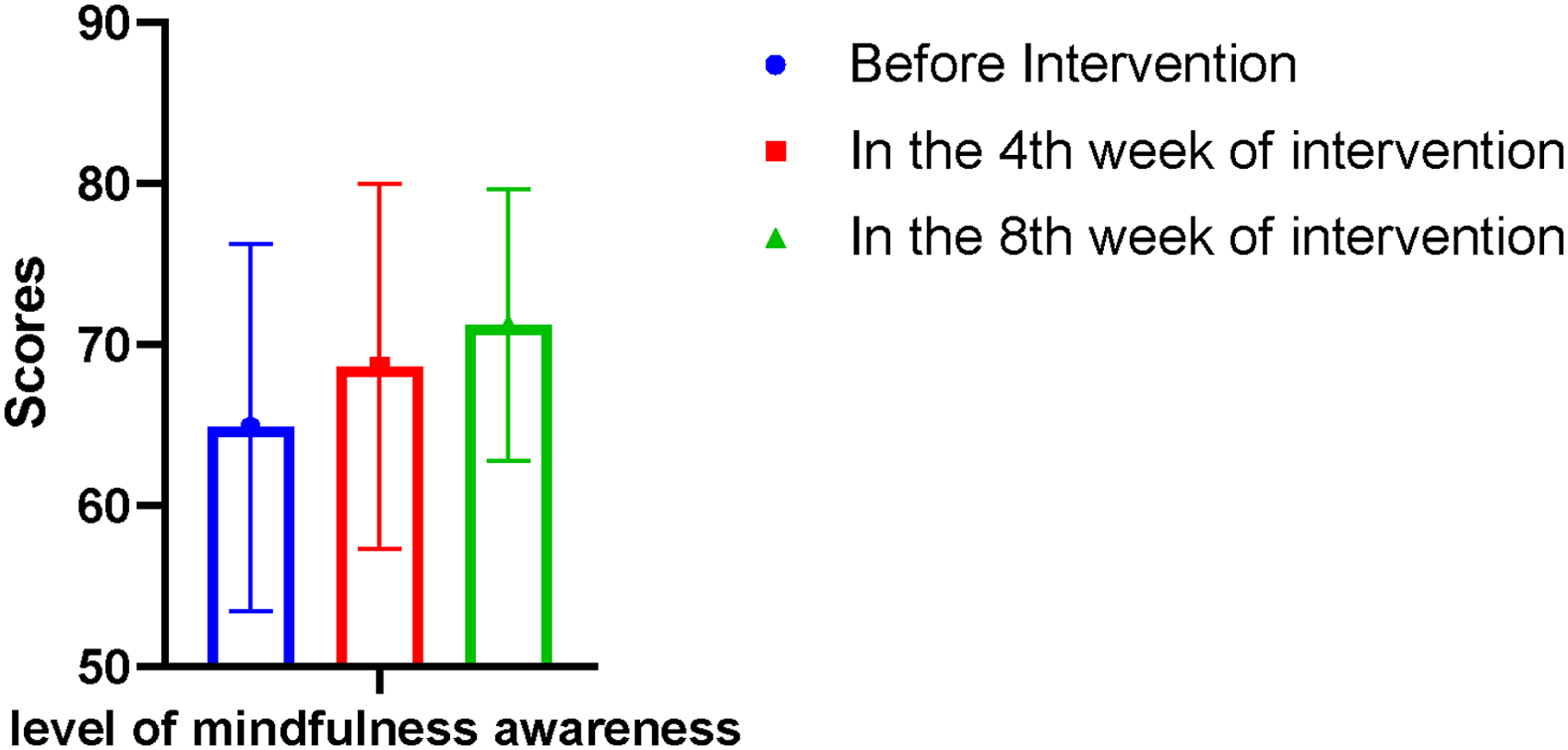
The level of mindfulness changes in three time points.
Discussion
The mindfulness intervention enhances the support of nurses as second victims
In this study, the need for support of the second victim nurses was measured by four dimensions in the SVEST scale, which were work-related organizational support (colleague support, senior worker support, and institutional support) and nonwork-related support (family and friends). The results presented in Figure 1 show that the requirements of second victims for organizational support of the three dimensions related to the work significantly decreased after the intervention, indicating improved quality of organizational support of the second victim nurses. A previous study (Zhang et al., 2019) showed that patient safety culture reduces the pain associated with medical error, absenteeism, and turnover intentions by enhancing organizational support.
Based on a literature review of intervention methods in positive psychology, this study created for the first time a formal employee support plan and an organization management model to adapt MM for clinical intervention in the treatment of the second victim nurses, which was shown to be significantly effective in helping them manage the stress and emotions in the aftermath. The results of the training in the recovery period of the participants indicate it can improve their cognitive ability and control over negative emotions, as well as allow them to learn from adverse events.
The fact that there is no significant difference in the scores of nonwork-related support between measurements may be explained by the following factors. In the special environment of clinical work and conservative social culture, nurses tend to keep their secrets to themselves instead of sharing them with their family and friends in the aftermath of adverse events. The phenomenon may result from the gap between professions in communication and their concerns that their friends would be worried. Relevant research shows that providing emotional support plays a key role in the recovery of the second victim both physically and psychologically, while the highest scored emotional support that the second victim most desires is support from colleagues and discussion of the incident with colleagues (Lewis et al., 2015).
MM Intervention Changes the Support Needs of the Second Victim of Nurses
The second victim's needs for support in this study were measured by seven additional items in the appendix of the SVEST scale. The study shows that the two items with the highest scores before intervention were Item 2 (a private and quiet place for second victims to restore calm in the aftermath) and Item 1 (the ability to leave the unit immediately for a period of time). The two items with the lowest scores for support needs were Item 7 (24 h contact with a specific person to discuss experience) and Item 4 (employee assistance programs provided a free consultation to employees after work). After eight weeks of intervention, the order of demand scores changed. The two items with the highest support scores were Item 3 (the opportunity to discuss the details of the incident with a respected peer) and Item 5 (the chance to discuss what happened in the event with a senior colleague). The switch shows that eight weeks of MM intervention changed the second victims’ attitudes from avoidance to confronting problems correctly. After adverse events, in the face of the traditional “blame culture” and punishment for errors in the health system, nurses habitually cower, choose to avoid, and even have a tendency to leave (Chen, Yang et al., 2019).
Research on the mechanism of MM suggests (Tang, 2018) that mindfulness intervention can enhance the functional connectivity between different brain regions related to executive functions during meditation and activate the cerebral cortex. MM training can guide practitioners to recognize themselves and the world around them through an objective developmental perspective using the control of metacognition, thereby helping them adjust their response to stress in the face of adverse events and promoting problem-solving and stress management. Some scholars designed an eight-week training plan with full reference to the intervention content of mindfulness-based stress reduction therapy and mindfulness-based cognitive therapy, which included both mental and physical exercises. The research results confirmed that mindfulness-based stress reduction was beneficial to the mental health growth of the second victim of nurses and could improve the level of professional identity of the second victim of nurses (Hofmann et al., 2017). Thus, in this study, after eight weeks of intervention, their need for support gradually shifted to discussion, analysis, and learning from the details of the event with their peers and senior colleagues. The need for Items 4 and 6 significantly changed before and after the intervention, but the absolute differences were small. This can be explained by the fact that the hospital has not yet provided psychological counseling for the second victim.
MM Intervention Improves Mindfulness Awareness Level of Mindfulness of the Participants
The regulating effect of MM on attention and emotion is a key factor in improving the level of individual mindfulness awareness and promoting physical and mental health. MM interventions purposefully focus the subject's attention on the present moment, without analysis, judgment, definition, unconditional acceptance, and objective experience of perception (Bostock et al., 2019; van der Riet et al., 2018). A number of studies have found that both temporary and long-term MM training can alleviate the individual's psychological and physical pain, and improve cognitive levels and the individual's ability to regulate emotion (Cheli, De Bartolo & Agostini, 2019; Tang, 2018; Vella & Mciver, 2019). MM training can enhance the mindfulness traits of the practitioner, and these traits help the practitioner stay calm and optimistic in the face of complaints, accusations, and self-blame. MM can help individuals focus on their work and improve their problem-solving ability and the ability to perceive themselves from the heart (Liu, Zhao & Lu, 2021). Hospitals can benefit from mindfulness interventions by improving the awareness of leaders and nurses. Nobel et al. (2019) conducted a four-week seminar about mindfulness for four medical and six nursing students. They found that all students’ abilities to cope with stress, attention, and adaptability significantly improved following the seminar (Nobel et al., 2019). The results of this study show that MM intervention significantly improves the level of mindfulness awareness of second victim nurses. The change in the support needs of the second victim also verifies the improvement of mindfulness awareness levels of the second victim nurse participants.
The evolving COVID-19 pandemic is placing unprecedented pressure on health systems. Accumulative studies suggest that nurses are more likely to develop negative psychiatric problems following a public health disaster than other medical staff due to their more frequent and closer contact with patients. A large number of studies show that after the COVID-19 pandemic, nurses developed many symptoms of anxiety, depression, sleep disorders, and posttraumatic stress disorder (Cui et al., 2021; He et al., 2021; Li et al., 2022). Thus, nurses need more mindfulness training to improve their awareness levels, especially in the COVID-19 era.
Strengths and Limitations
The strengths of this study were that it was the first study to investigate the implementation of the MM intervention in relation to supporting second victim nurses and that the intervention was carried out systematically and in accordance with the “Educator Toolkit” from the “The 2017 Resident Wellness Expert Consensus Summit.”
The first critical limitation is the absence of a control group. This study developed its own before and after controls but was not randomized due to practical difficulties. As some nurses were absent due to the night shift, although they had participated in the online training, the researchers noticed that there is still a certain gap in the effectiveness and convenience between in-person and online courses. Additionally, a majority of the study sample consisted of females; thus, the results may not be generalizable to male nurses. Self-reported measures may be prone to expectancy bias/underreporting/overreporting. This study did not intervene with a single adverse event type or severity, and there may be notable differences in event types themselves and their effects on a second victim.
The most important thing is this study is a single-center study, all the subjects are from the same center, and the results of this study are not well generalized. However, this study is one of the few in China to carry out such research. Moreover, the hospital, which undertakes this study, is a domestic third-class A hospital with advanced medical equipment, excellent service quality, and rich scientific research experience. At the same time, this study was highly supported by the leadership of the hospital, and the study was successfully completed. The research results can provide a reference for the follow-up of relevant studies.
Implications for Practice
Through this MM training for 46 nurse victims of adverse events, the researchers summarized the experience and deficiencies of the training and carefully considered how to widely promote the use of mindfulness in hospital organizations. The researchers found that it is actually difficult to gather a large number of nurses together in training, which requires extensive coordination (including personnel scheduling, appointments at large meeting venues, logistics, services, etc.) Therefore, in the later stages, the researchers also explored methods that are more suitable for clinical nurses, anytime and anywhere within the department, to conduct organized and planned mindfulness training.
Mindfulness can actually be an idea embedded in our daily lives and work. For example, at the morning meeting, perform simple breathing training in a short 5 to 10 min, a mindful walk after lunch, or do not hurry home from work, rest or take a nap, listen to music, conduct a 10-min body scan, and so on. In addition, after the adverse event, the researchers can immediately provide a nurse with appropriate care and teach them to adjust their mood and breath to manage the matter. The rest of this work includes the use of mindfulness of the mind.
Following the implementation of these strategies for a period of time, the researchers found that nurses were able to accept this free form of mindfulness practice. This suggests that mindfulness training sometimes does not require intensive practice and that it can be applied both to clinical patient nurse groups or to nursing student groups. The therapy not only reduces stress but can also lead individuals to share common core values as many mindful philosophies and nursing practices of MM do. For example, through mindfulness training, nurses can cultivate clearer insight and more empathy for patients, as well as tolerance, compassion, and gratitude.
Conclusion
For second victims, a support system connected to a medical institution or department is necessary for psychological support and external assistance. MM intervention is applicable to the second victim population of nurses and can serve as an effective method of second victim support. It can assist in effectively improving the level of nurses’ second victim's mindfulness awareness and can be applied and promoted in medical institutions.
Further studies of randomized controlled trials or a fixed specific type of adverse events and long-term follow-up are required to clarify the effect of the intervention. Objective evaluation indicators, such as neuroimaging methods of functional magnetic resonance imaging or neuroendocrine mechanism studies, should be actively sought to demonstrate their effectiveness. In addition, the feasibility study may be more meaningful.
Footnotes
Acknowledgements
Thanks are due to Xiaomin Ding for assistance with the study and to Shihua Pan for valuable discussion. The authors thank all participants in the invention. In addition, I would like to thank the editor and anonymous reviewers, who have helped to improve the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chinese Nursing Association Annual Research Funding (grant number ZHKY201902) and by Zhongnan Hospital of Wuhan University Science, Technology and Innovation Seed Fund, Projectznpy2019102.
Ethics Statements
The research was consented by the competent department of the hospital, affiliation of the researchers with the approval of the ethics committee and all participation of subjects was approved by the ethics committee (ethics batch number: 2019355). The research conformed with the Declaration of Helsinki. Ethics Committee of Zhongnan Hospital of Wuhan University (Zhongnan Hospital of Wuhan University).