
Abstract
Introduction
Workplace violence (WPV) is a growing concern that constitutes a major threat to occupational health and safety, thereby comprising a priority issue for policymakers. Given the increasing prevalence of chronic diseases and comorbidities among the Lebanese population, nurses working in critical care settings encounter intense workloads and high-risk interactions, potentially increasing the risk of WPV.
Objectives
This study aimed to investigate the traumatic and psychological reactions of Lebanese critical nurses who have been exposed to WPV, and the risk factors for depression and anxiety.
Methods
The study utilized a cross-sectional descriptive correlational design; 112 critical care nurses from diverse departments took part in this study during the period of June to July 2021.
Results
A positive, significant correlation between WPV exposure and self-reported anxiety was observed, p = .03 with high levels of WPV, especially among patients and their families. Although verbal abuse was found to be more prevalent among critical care nurses in Lebanon compared to physical and sexual violence, the severity of the situation and its impact on the nurses’ mental health and well-being cannot be ignored.
Conclusions
WPV for critical care nurses is a serious issue that needs to be considered. Policy-makers should develop the politics of regulating the nursing profession, especially for critical care nurses in Lebanon.
Introduction/Background
Workplace violence (WPV) is becoming a major threat to occupational health and safety, resulting in a wide range of concerns for policymakers and employers (Rayan et al., 2019; Wyatt et al., 2016). According to the National Institute for Occupational Safety and Health, violence is defined as “any act of assault directed against people at work or while performing work-related duties, ranging from aggressive or threatening language to murder” (Martinez, 2016). Violence and abuse against health workers by clients or visitors are recognized as a global public health issue, primarily in the client-on-worker abuse (Cowman et al., 2017). This problem can negatively impact the delivery of quality patient care and decrease productivity in the healthcare environment (Al-Ghabeesh & Qattom, 2019).
WPV among healthcare professionals has been reported in various studies around the world, including, the United States (Phillips, 2016), Asia (Ambesh, 2016), England, and the majority of Europe (Cowman et al., 2017). In the United States alone, it is estimated that there are 900 deaths and 1.7 million preventable incidents annually as a result of occupational abuse (Crawford et al., 2019). Over 50% of healthcare professionals in the healthcare industry, one of the most vulnerable industries to violence in the world, have reported experiencing violent incidents at work, with figures reaching up to 70–80% for emergency personnel, nurses, and physicians (Meacham et al., 2020). Likewise, occupational abuse among health professionals has become prevalent in Chinese facilities (Zhao et al., 2018).
WPV can be categorized into two types: vertical or horizontal. Vertical violence involves both healthcare workers and patients, while horizontal violence occurs between healthcare workers and patients themselves. In addition, it could be categorized as physical or psychological (Bernardes et al., 2020). Physical violence can include actions such as but not limited to shoving, punching, and jabbing. However, psychological violence, such as verbal abuse has been reported to be one of the most common forms of violence among healthcare workers. A previous study, for instance, documented that 61.9% of healthcare workers reported exposure to WPV, 42.5% experienced psychological violence, and 24.4% suffered from physical violence. Verbal abuse was the most prevalent form of psychological violence (57.6%), followed by threats (33.2%) and sexual harassment (12.4%) (Liu et al., 2019).
Review of Literature
Nurses are the healthcare workers most frequently exposed to WPV and abuse, which has become a daily reality (Bernardes et al., 2020). For example, a recent study found that 89.6% of Iranian nurses experienced some form of violence, with 68.4% experienced more than one type of violence. Verbal abuse was the most common type of violence (83.9%) (Honarvar et al., 2019). The high-risk nurses for workplace-related violent exposures are those who are working in critical care units (Bernardes et al., 2020). Nurses working in critical care units, such as intensive care and emergency departments, are at higher risk of violent exposure (Bernardes et al., 2020; Speroni et al., 2014). Physical and verbal abuse among nursing staff in critical care units has been reported to be on the rise (Pinar & Ucmak, 2011), and these professionals encounter approximately one to ten instances of violence a year (Lu et al., 2019). Bernardes and colleagues (2020) reported that 88.9% of emergency nurses reported WPV, with 38% experiencing verbal abuse, 25.4% suffering from mobbing, 11% reported physical violence, 9.1% experiencing sexual harassment, and 5.4% enduring racial discrimination. In Jordanian emergency nurses, studies demonstrated that 90% of the nurses experienced bullying (Al-Ghabeesh & Qattom, 2019). Moreover, Albashtawy and Aljezawi (2016) indicated that verbal violence was the most common form (63.9%) compared to physical violence (48%) among Jordanian emergency nurses.
There are various causes of WPV in critical care units and can be attributed to both patients and nurses. The most common sources of aggression come from patients and their relatives (Viottini et al., 2020). Patient-related factors contributing to WPV in critical care units include age (particularly those in their 20s and 30) (Abualrub & Al Khawaldeh, 2014), gender (Abualrub & Al Khawaldeh, 2014; Maran et al., 2019), psychological comorbidities (Abualrub & Al Khawaldeh, 2014; Itzhaki et al., 2018), substance abuse, physical comorbidities (Abualrub & Al Khawaldeh, 2014), and ethnicity (Maran et al., 2019).
Factors associated with WPV in critical care units that pertain to nurses include, having less experience (five years) and working in public hospitals (Sousa et al., 2021). Less experienced nurses might be more vulnerable to abuse in the practice environment, and this could be associated with the lack the awareness to identify signs of violence (Albashtawy, 2013). Environmental factors such as inadequate security, unrestricted public movement, unfavorable conditions, delays in service or care, poor working conditions, and overcrowding (Eurofound & International Labour Organization, 2019) can also have a significant impact on violence.
WPV can have a negative impact on the physical and psychological well-being of nurses, resulting in depressive symptoms (Baran Aksakal et al., 2015; Fang et al., 2018), anxiety (Baran Aksakal et al., 2015; d’Ettorre et al., 2018), feelings of insecurity and fear, reduced productivity, social withdrawal (Moffa & Longo, 2016), and decreased self-esteem and confidence (Cordenuzzi et al., 2017; Moffa & Longo, 2016). Also, it can impact job performance and career advancements (Al-Ajarmeh et al., 2021; Liu et al., 2018), resulting in occupational stress (Itzhaki et al., 2018), burnout (Liu et al., 2018), and high turnover rate (Choi & Lee, 2017). This abuse has been linked to an increased risk of developing type 2 diabetes (Xu et al., 2018), and a decreased quality of life for healthcare professionals (Itzhaki et al., 2018). It can also cause negative emotions such as anxiety and depression anxiety (Theorell et al., 2015), and this may contribute to sleep difficulties (Sun et al., 2017).
Keep in mind that nurses make up 70% of the healthcare professionals in Lebanon, a Middle Eastern country that has experienced conflict and political unrest. Nurses are subject to a range of workplace stressors as frontline healthcare providers. Studies around the globe have shown that the levels of emotional distress among nurses are concerning (Alameddine et al., 2015). Verbal abuse was found to be the most prevalent form of violence for 70.6%, followed by bullying and mobbing 29.4%, physical assault (11%), and sexual harassment (6.6%) (Zainal et al., 2018). Another study also reported that four out of five Lebanese emergency room (ER) personnel documented verbal harassment, and one out of four confirmed physical aggressions (Alameddine et al., 2011). Concerning Lebanese nurses, Alameddine and colleagues (2015) reported that two-thirds of the nurses experienced verbal abuse and 10% reported physical aggression. However, Lebanon has been aware of the impact of WPV on healthcare services.
With the rising incidence of chronic diseases and comorbidities among the Lebanese population, nurses working in critical care units are being encountered due to excessive workload and frequent exposure to hazardous situations, which is highly likely to result in an increase in WPV accidents. Therefore, healthcare systems need to collaborate in reducing violence and abuse among healthcare workers. Violence has significant consequences for employers, staff, and patients. Therefore, policy-makers, administrators, and healthcare personnel need to work collaboratively to take an action, create, and enforce preventive measures to alleviate and control this issue. It should be guaranteed that nurses, especially in critical care units, have the best environment and safety measures during their shift at their health institutions. It is very necessary to study WPV among Lebanese nurses in critical care units, which will assist in developing health policies that will provide protection to nurses and contribute to the prevention and management of violence.
Purpose of the Study
This study aims to assess the WPV and psychological reactions (depressive and anxiety symptoms) of Lebanese nurses working in critical care units.
Methods
Design
This study used a cross-sectional, descriptive, and correlational design between June and July 2021.
Sample
The study population included critical care nurses at a private hospital in Lebanon. A convenience sample was selected to recruit the study participants. This sampling technique was appropriate due to the small and limited number of nurses working in critical care units.
This study was conducted in critical care units, specifically the Cardiac Care Unit (CCU), Cardiac Catheterization Laboratory, Intensive Care Unit (ICU), ER, Neonatal ICU, and Pediatric Intensive Care at a private hospital in Lebanon. This hospital is designed to provide the most innovative treatments using the most advanced technologies in a safe and compassionate environment. The hospital has a capacity of 200 beds and employs around 125 specialized doctors, 322 nurses, and 353 administrative staff members.
Inclusion/Exclusion Criteria
The inclusion criteria for the study involved full-time nurses who had a minimum of six months of working experience in critical care units, graduates of an English language–based nursing program, thus proficient in the English language, and willing to participate in the study. However, the exclusion criteria included nurses in administrative positions.
Ethical Considerations
Official permission to conduct this study was obtained from the institutional review board at Beirut Arab University and the chosen private hospital. Informed consent was obtained from the nurses who met the inclusion criteria after an explanation of the aim of the study. The participants were assured that their participation was voluntary and that they could withdraw at any time without risk. Confidentiality was maintained throughout all stages of the study.
Instrument for Data Collection
The information was gathered through the use of a self-reported questionnaire that included the following sections: sociodemographic and professional data, the WPV against nurses’ scale, the self-rating depressive scale (SRDS), and the self-rating anxiety scale (SAS).
The first section was sociodemographic data that included the participant's gender, age, marital status, and work unit. The second section was the WPV against Nurses Survey, developed by Lin and Liu (2005) to measure WPV against nurses. This scale consists of items that address the frequency and pattern of WPV (frequency of violence, sources of violence, type of violence, place, time, and reaction to violence) and items that address the consequences of violent incidents and satisfaction with incident handling. Physical and nonphysical assault were the two broad categories of violence. Physical assault was defined as the deliberate use of force (hitting, kicking, slapping, choking, biting, or pushing). The nonphysical assault included verbal harassment and abuse (including threats and sexual comments), including any humiliating and undignified comments based on age, sex, race, color, disability, language, religion, and economic or social status. Sexual harassment was defined as any unwanted sexual verbal or physical gestures (Lin & Liu, 2005). This tool is valid and reliable, where Cronbach's alpha was 0.81 and the content validity index produced by consulting two experts in the field of nursing administration was CVI = 0.85.
The third section was the SRDS that was developed by Zung (1965) to measure depressive symptoms over the past week. This scale is comprised of 20 items. Each item is rated on a 4-point Likert scale and ranges from 1 (never or some of the time) to 4 (most of the time). The total possible standard score, ranging from 25 to 100, was obtained by multiplying the total original score by 1.25. A total score of 53 was considered the cutoff for the experience of depressive symptoms (Zung, 1965). A standard score of 53–62 indicates mild depression, 63–72 reflects moderate depression, and >72 indicates severe depression. This tool has good validity and reliability with Cronbach's equals 0.89, and the content validity index which was produced by consulting two experts in the field of clinical psychology was CVI = 0.89.
The fourth section was the SAS that was developed by Zung (1971) to measure the self-reported anxiety symptoms of nurses over the previous week. This scale is comprised of 20 items rated on a 4-point Likert scale and ranges from 1 (never or some of the time) to 4 (most of the time). The total standard score ranged from 25 to 100, and the total standard score of 50 was considered to have anxiety symptoms. In addition, the anxiety symptoms were classified as follows: the total standard score ranged between 25–55 for minimal anxiety, 56–73 for mild to moderate anxiety levels, 74–93 for marked to severe anxiety levels, and >94 for extreme anxiety levels. The Cronbach alpha coefficient was 0.92 and the CVI = 0.9.
A pilot study of ten critical care nurses was conducted to assess the adequacy of research instruments, assess the feasibility of a full-scale study, determine whether the research protocol is realistic and workable, and identify logistical issues that may arise when using the proposed methods. Ten nurses who met the inclusion criteria were recruited to be included in the pilot study. The consent form was signed by all participants who were informed about the objectives of the study. Participants were provided with instructions about the study procedure and questionnaires completing the process. Participants reported that study questionnaires were clear, relevant, appropriate, and understood. Nurses who participated in the pilot testing were not included in the full-blown study.
Data Collection Procedures
Meetings were arranged with the head nurses of each unit in the hospital. The purpose of the study and instructions regarding the questionnaire were clarified to them. Also, an agreement to distribute the questionnaires by head nurses was obtained. After that, the questionnaires were given to the head nurses associated with envelopes in order to put the answered questionnaires in these envelopes. After one to two weeks, the envelopes were collected from each unit.
Data Analysis
Data were entered and analyzed using SPSS, version 24. The sample characteristics were described using descriptive statistics (mean, SD, frequency, and percentage). An independent t-test was carried out to determine whether there was a difference in the level of experiencing WPV according to gender, anxiety, and depressive symptoms. A Kruskal–Wallis test was carried out to determine whether there is a significant difference in the level of WPV according to age and working unit. A bivariate correlation was carried out to determine whether there is a relationship between WPV, absenteeism, career changes, anxiety and depression, and WPV experiences. A linear regression test was conducted to detect the predictors of WPV. The alpha value was significant at 0.05.
Results
Sample Characteristics
A total of 150 questionnaires were distributed, and 112 were returned, with a response rate of 74.6%. Concerning sociodemographic data, the majority of the participants were females. The gender distribution in the sample was roughly equal. In addition, 50% of the participants were aged between 18 and 25 years old, and 69.6% of the nurses were single. Moreover, 51.85% of the participants have worked in the ICU (Table 1). Eighty-eight nurses (78.6%) were worried about violence in the workplace, and 60.7% of the nurses were encouraged to report violent incidents. In addition, 75% of the nurses who received encouragement regarding WPV reported management/employers as the most encouraging factor. The results also showed that 87.5% of the nurses had not taken any WPV prevention training in the past 12 months. Moreover, 80.4% of the nurses did not miss a working day after the violent incident, and 76.8% did not experience any career changes after that incident (Table 1). The study findings showed that one-half (50%) of the nurses endorsed the incident reporting. The most common reason for failure to report was a lack of organization in the incident reporting system (16.1%) (Table 1). Safety rate, 39.3% of the nurses reported that their work was not safe at all; 33.9% of the nurses reported that the measures taken by the organization to prevent WPV were not effective at all (Table 1).
Sociodemographic Data (N = 112).

This study found that the mean score of anxiety symptoms level was 19.73 (SD = 9.84) and 64.3% of the participants reported moderate to extreme anxiety. Also, the mean score of depressive symptoms was 20.67 (SD = 8.80) and 100% of the nurses were normal (free from any depressive symptoms) (Table 1).
Almost one-third of the nurses (33.9%) reported being occasionally subject to verbal abuse, and 17.9% reported being frequently subject to threats. However, 17% of the nurses more frequently experienced verbal abuse. Also, 46.4% of the nurses reported rarely being subject to physical abuse and 19.6% of the participants reported a rare occurrence of sexual violence (Table 2).
Frequency and Sources of Workplace Violence.

Additionally, 28.6% of the nurses experienced threats mainly from the family or friends of patients, while 48.2% of them experienced verbal abuse from the same source. In addition, 32.1% of the nurses experienced physical abuse from patients’ families or friends, while 25% of them experienced physical abuse from the patients themselves. Concerning the experience of sexual harassment, almost 68% of the nurses did not experience it; however, 8.9% experienced it from patients and 16.1% experienced it from family or friends of the patient (Table 2).
The findings revealed a significant difference in violence (p = .001), with males (M = 4.74) experiencing more violence than females (M = 2.96). However, there was a significant difference in the rating level of the institution's safety (p = .05), with females scoring higher than males (M = 0.96) and males (M = 1.31) (Table 3). On the contrary, there were no significant differences between males and females in the level of encouragement to report the incident (p = .76), in the level of actual incident reporting (p = .70), in depressive symptoms (p = .20), and anxiety symptoms (p = .65).
Differences According to Gender.

Significant at the 0.00 1 level.
Significant at the 0.05 level
Furthermore, a nonparametric Kruskal–Wallis test was employed to examine differences in experienced types of violence according to age groups. The results showed that there was no difference in threats and sexual harassment; however, a significant difference exists in experiencing verbal abuse (χ2 = 9.692, df = 3, p = .02) and physical violence (χ2 = 9.010, df = 3, p = .03) (Table 4). The pairwise comparisons showed that in verbal abuse the significant difference is between the group of nurses aged between 26–35 and 36–45 (p = .02) (Table 5), where the former had a higher mean rank (Figure 1). In experiencing physical abuse, a significant difference was found among the same two age categories (p = .008) where the former also had a higher mean rank (Figure 1). As for work unit, another nonparametric Kruskal–Wallis test was employed and it showed that there was a significant difference in the frequency of experiencing sexual harassment (χ2 = 16.474, df = 4, p = .002) (Table 6). The pairwise comparisons showed that there is a significant difference between nurses working at the ER and those at the ICU (p = .00), where ICU nurses reported a significantly higher frequency of sexual harassment evidenced by a higher mean rank (Figure 2). This was also the case between ICU and CCU nurses (p = .02), where also ICU nurses had a higher mean rank (Table 7).

Mean ranks of age groups relating to verbal abuse and physical violence (left to right).

Mean ranks of work units relating to sexual abuse.
Kruskal–Wallis Test According to Age Group.

Pairwise Comparisons of Age.

Significant at the 0.05 level.
Kruskal–Wallis Test According to Work Unit.

Pairwise Comparisons of Unit of Work.

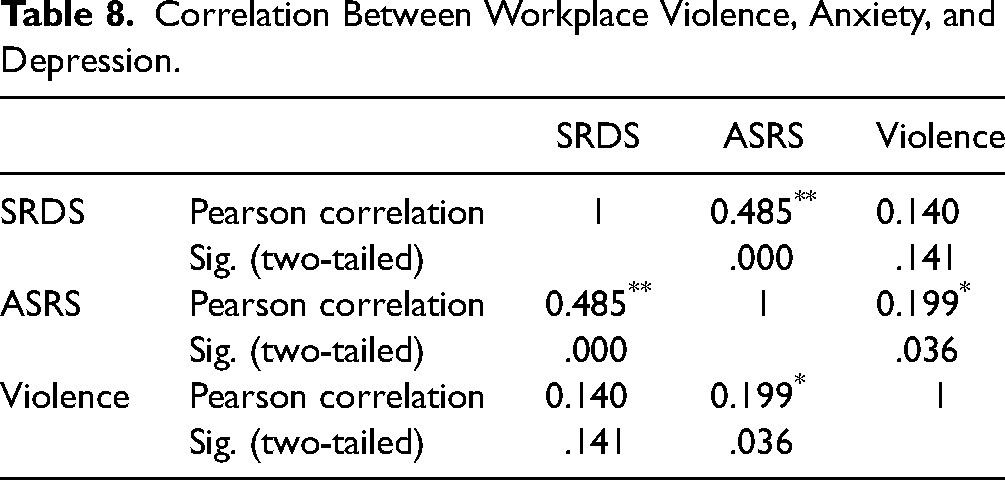
The results of the Person's bivariate correlation showed that there was a significant positively moderate linear association between self-reported anxiety and depression (r = 0.485, p = .00), while a weak significant positive linear association was found between experiencing WPV, and self-reported anxiety (r = 0.199, p = .036) (Table 8).
Correlation Between Workplace Violence, Anxiety, and Depression.
A linear regression analysis was used to examine the predictors for WPV. The model included gender and working unit. The male gender was coded “0” as a reference group and the female gender was coded “1”. Considering that working unit is a categorical variable with multiple subgroups, dummy variables were created in order to be able to include this variable in the linear regression model and enhance interpretability of the results. The ER unit was designated as a reference group. The results showed a significant Y-intercept of b0 = 5.61 (p = .00). The model suggests that being a male increases the odds of exposure to violence by b1 = 1.57 (p = .00) times, and in comparison to nurses working in the ER, the odds of those working in the CCU to be exposed to violence are less by b2 = −1.81 (p = .01). The coefficient of determination R2 = 0.18, thus indicating that this model predicts only 18% of the changes to WPV exposure. Thus, this suggests that there are other variables to consider in predicting the exposure of critical care nurses to violence (Table 9).
Predictors of Workplace Violence.

Discussion
Lebanon's health care system has suffered from a severe deficiency in the nursing workforce, which has resulted in increased levels of stress for nurses already practicing, particularly in critical care units, where nurses tend to deal with difficult cases that require time-consuming and effort-consuming measures of significant risk. On the other hand, in any institution, occupational violence is a significant concern. In the healthcare workplace, harassment and aggression limit the quality of patient care. For most nurses, abuse is a part of their daily lives. More specifically, critical care nurses operate in high-risk settings and might be more prone to experiencing various types of violence. It should be guaranteed that nursing professionals should have a secure environment and the nurses should be respected for their practice at any health organization to provide high-quality care, health of the nursing workforce, and retain the experience that has been built in such a work environment. Therefore, to get a more profound understanding of this phenomenon, this study highlights the critical care nurses’ experiences with violence and the psychological reactions they experience.
The results of this study showed that the vast majority of the critical care nurses reported experiencing worries regarding WPV, even though they had not received any violence prevention training in the workplace. The results also showed that a significant proportion of the critical care nurses regularly experienced threats and verbal abuse, mainly from patients and relatives, while some even experienced physical abuse and sexual harassment from the same category of aggressors. These results are consistent with a previously published research paper that assessed the violent experiences of critical care nurses in Lebanon and found that a notable proportion of the nurses reported exposure to mainly verbal violence and threats such as shouting and angry outbursts, which have been instigated by patients’ family members and patients due to long waiting times (Alameddine et al., 2011). The current study results are also in line with a previous study that has been conducted in hospitals in 16 Chinese provinces among practicing nurses and found that the vast majority were subjected to WPV (Li et al., 2019). Pourshaikhian et al. (2016) found that critical care nurses were highly exposed to WPV, particularly verbal abuse from patients and their relatives, which corroborated this study's finding. Furthermore, Zhang et al. (2017) found that 63.7% of nursing professionals were subjected to verbal violence, 25.8% to physical violence, and 2.8% to workplace sexual harassment, which is similar to this study's finding. The findings of the current study were also supported by AlBashtawy and Aljezawi (2016), who discovered that verbal abuse is the most common type of WPV experienced by critical care nurses. Also, Han et al. (2017) have found that patients’ relatives are the most frequent perpetrators of violent exposures among critical care nurses, even more than patients themselves, which also resounds with the present study findings.
The results of this study showed that there was a significant difference in the experiences of violence among the critical care units, where emergency department nurses had the highest means. This is consistent with Zhang et al. (2017), as the study designated the ER as a particularly high-risk healthcare environment for violence. In addition, a recent review published by Spector et al. (2014) has indicated that the ER scored the highest number of WPV in comparison to all other healthcare practice settings, where a figure of 49.5% of the nurses working in the ER was subject to physical violence, and even a more shocking number, or 81.3%, were subject to verbal violence.
The findings in this study revealed that half of the nurses did not report incidents of violence to management, owing to a lack of an effective reporting system and the need to become more efficient in managing these episodes. This was in line with the findings of Xing et al. (2015), who found that the majority of nurses who experienced WPV did not report it to management due to a lack of effective reporting systems, embarrassment, and the belief that reporting is pointless. The present study results were also consistent with AlBashtawy (2013), who found that despite the occurrence of WPV among nurses, the majority of them did not report it, as they were used to the violent exposure and believed they were able to handle it by themselves and that any reporting and judgment would not be in the favor of the nurse.
Furthermore, the findings of this study revealed that the nurses significantly rated their institution as unsafe, with males reporting lower levels of safety perception than females, and a significant percentage of them reporting that the hospital’s prevention measures are ineffective in combating violent exposures. This is consistent with the findings of Alameddine et al. (2011), who found that the majority of respondent nurses reported that violence prevention measures at their respective hospitals were ineffective. In addition, various previous studies have similar findings to the current study where it was shown that regardless of the preventive measures that have been implemented by their institutions to prevent WPV against critical care nurses, the rates of reported violence were still high, thus rendering the established preventive measures ineffective and critical care units insecure for clinical practice (Zhao et al., 2016). Moreover, the findings in this study are highly consistent with those of Xing et al. (2015), who have indicated that a very low number of nurses have received occupational training against workplace aggression.
The results of this study also showed that the majority of the critical care nurses who participated in this study experienced substantial levels of self-reported anxiety, which have been significantly correlated with violent exposures. These findings are consistent with Alameddine et al. (2011), who have also found that nurses in critical care departments have experienced emotional exhaustion due to the recurrence of violence. In addition, Li et al. (2019) also found that PTSD symptomatology started to appear due to violent exposures, which establish the results of this study in terms of severe psychological influences such as anxiety. Jeong and Kim (2018) also had similar results to this study, where the study found that exposure to WPV by critical care nurses has led to the development of intense emotional responses and mainly increased stress and anxiety, which called for evaluating the coping mechanisms of designated nurses. In addition, Lee and Lee (2021) have found comparable results to the present study, where their study evaluated the relationship between WPV and emotional responses among nurses and has found that exposure to verbal abuse among nurses increased their work stress, higher absenteeism, and poor psychological health. Moreover, the results of this study were consistent with that of Hassankhani et al. (2018) who have found that abuse in the workplace can have sustained effects on the well-being and efficiency of nurses; those who witnessed it stated that they had adverse impacts on their physical and mental health, and career advancement. Furthermore, the results of various previous studies have supported the current study findings, where it has been found that WPV whether verbal or physical has led to an increase in stress levels among critical care nurses and yielded long-term anxiety (Graham, 2017; Harb et al., 2021).
However, the results of this study showed that few changes to career choice have been prevalent due to violent exposures, mainly transferring work units, which is inconsistent with Graham (2017), who has found that the violence experienced by nurses has led to high levels of turnover, job dissatisfaction, and intent to leave. The results of this study might be explained by the commitment and responsibility the critical care nurses in Lebanon have been practicing; thus, they either stayed in their jobs or asked for a transfer to another unit. Another factor that might have contributed to the lack of turnover among critical care nurses is the economic situation in Lebanon, which might have obliged the nurses to stick to their jobs in the light of high unemployment rates in the country.
Finally, the results of the current study found that gender and working unit are predictors of exposure to WPV. This is consistent with the results of Abed et al. (2016), who evaluated the prevalence of WPV among healthcare workers and found that gender is a significant predisposing factor to WPV. Similarly, job demands in the critical care unit have been identified as a predictor of WPV by Wu et al. (2015), which is also in line with the findings of the current study.
Strengths and Limitations
Regardless of the significant results, this study has some limitations, including small sample size and the fact that the sample was selected from one single medical center.
Implications for Practice
The findings of this study demonstrated how healthcare organizations must comprehend the current condition of their nursing workforce. Furthermore, it is particularly critical that nurse leaders offer or strengthen resources to manage the risk factors of abuse in the workplace. Nurse administrators, for example, should include extra measures and enhanced reporting systems for critical care nurses and ER nurses who specifically are subject to high levels of WPV. Effective policies and procedures should be put in place to ensure that any violent incident is handled appropriately in order to protect critical care nurses and protect their practice and the quality of services provided. Furthermore, regular training sessions will be held to educate staff on the measures to be taken, from dealing with aggression and perpetrators to reporting the incident and encouraging them to report it while assuring them that it is for their benefit. Specifically, nurse leaders and hospital administrators should put extra emphasis on ER and ICU nurses as it seems they are more prone to violent exposures. Sexual harassment policies are highly in need in these institutions as evidenced by the results of this study, and male nurses are to be focused on as much as female nurses in policies that target violence prevention.
Moreover, strict measures should be enforced regarding the interaction with relatives of patients, such as limiting visiting hours to enable security systems to prevent aggression. Furthermore, psychological and legal assistance and care should be provided to critical care nurses in the case of violent exposures so that proper action will be taken and nurses will start to believe in the system and rely on it in such cases.
Conclusions
Workplace violence for critical care nurses is a serious issue that needs to be considered. Policy-makers should develop the politics of regulating the nursing profession, especially for critical care nurses in Lebanon. Verbal abuse was the most common type of violence among critical care nurses in Lebanon. The high incidence of WPV and the reluctance to report and take action were alarming findings. This study sheds light on the high levels of WPV recorded by critical care nurses and the prevailing psychological consequences of violence in the absence of proper policies and procedures for reporting as well as prevention and training measures. Further research is needed to examine the protocol models for reporting and dealing with aggression through longitudinal studies and qualitative exploration of violent exposures.
Footnotes
Authors’ Note
The present research was conducted in accordance with the general ethical guidelines, and the ethical approval was obtained from the Institutional Review Board (IRB) of Beirut Arab University. Written informed consent was obtained from all participants prior to the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.