
Abstract
Introduction
The incidence of breast cancer in Indonesia is the highest among types of cancer in women, with an estimated pain prevalence of 40%–89%. More than 50% of cancer patients suffer from pain that has not been resolved. Cancer pain's impact will affect the comfort level and quality of life.
Objectives
The purpose of this study was to analyze the effectiveness of DRM Pain Relief on the degree of pain, comfort, and quality of life among breast cancer patients.
Methods
The research was a true experimental study with pre-test and post-test designs with a control group. The population was all breast cancer patients attending hospitals in Semarang and Pekalongan Districts. The research subjects were 64 respondents who met the inclusion and exclusion criteria. Respondents were selected randomly and divided into two groups, namely 32 in the treatment group (DRM Pain Relief application) and 32 in the control group (only received drugs as conventional therapy in the hospital). Data were analyzed using a multivariate test.
Results
The application of DRM Pain Relief was effective in reducing the degree of pain (p < .001), and effectively increasing comfort (p < .001), as well as improving the quality of life of breast cancer patients in the components of improvement in symptom status, functional status, and global quality of life with p-value <.001, .003, < .001, respectively.
Conclusion
The DRM Pain Relief effectively reduces the degree of pain, increases comfort, and improves the quality of life of breast cancer patients.
Introduction
The incidence of breast cancer ranks highest among cancers in women, which is 25% of all cancers in women with a proportion of 240 out of 100,000 female population (Arnold et al., 2022; Purwanto et al., 2015). Breast cancer is the most common cancer treated in hospitals (Suzanna et al., 2012). By 2040, the burden of breast cancer is predicted to increase to more than 3 million new cases and 1 million deaths each year due to population growth and ageing (Arnold et al., 2022).
The International Association for the Study of Pain (IASP) estimates the prevalence of breast cancer pain to be between 40% and 89% (Satija et al., 2014). More than 50% of cancer patients suffer from pain that has not been entirely resolved (Desen & Japaries, 2011). Unresolved pain causes discomfort and negative physical, psychological, and social effects in breast cancer patients’ lives, leading to decreased quality of life (Black et al., 2011; Cornell et al., 2020; Satija et al., 2014).
Three percent of advanced cancer pain management cases were classified as inadequately managed (undertreatment). This fact is supported by Satija et al. (2014), who states that even though breast cancer patients have received adequate breast cancer treatment, some patients still experience severe pain, either related to disease progression or the effects of anti-cancer therapy.
The main focus in solving the problem of cancer pain is to beat the pain, work on managing it, and not let the individual be weakened by it. Pain is often used to describe discomfort, and controlled pain is often used to represent comfort (Siefert, 2010). There is a decrease in comfort due to an increase in the degree of pain (Findik et al., 2013). Therefore, breast cancer pain is a complex phenomenon that makes pain management interventions a critical component in nursing and requires management with the right strategy.
Various nursing actions have been carried out to overcome the discomfort. Patients prefer not to use drugs because they think they have more harmful effects. One non-drugs procedure for treating pain is rubbing massage. Massage rubbing on the back is a method of reducing pain with massage and rubbing techniques. However, the nurse said it was very inefficient to massage the patient using their fingers every time a complaint of pain occurred.
On the other hand, electronic massage tools have not been specifically used to treat pain. Most of these massage tools are only for eliminating fatigue (aches, stiffness in the body, and increasing blood circulation). Therefore, innovation is needed. Combining the existing comfort-based pain management model with Digital Rubbing Massage-Pain Relief (DRM Pain Relief) is expected to relieve cancer pain effectively.
DRM Pain Relief tools use sine waves and binaural beats to produce the sensation of a rubbing massage. The development of a DRM Pain Relief tool is necessary because doing massage and rubbing simultaneously using your fingers is very inefficient and tiring because the appearance of pain can occur at anytime and anywhere. With the development of the DRM Pain Relief tool, it is expected that breast cancer patients will be able to deal with pain independently.
Researchers have developed DRMPain Relief but previously has not been validated and applied to breast cancer patients. This tool is expected to help breast cancer patients reduce pain, maximize comfort, and have an optimal quality of life. Thus, breast cancer patients can function optimally in their daily lives.
Review of the Literature
Breast cancer is an abnormal development of cells that occur in breast tissue. Breast cancer is the most common type of cancer and is the leading cause of death in women worldwide (Arnold et al., 2022). Indonesia's estimated mortality rate from breast cancer is 18.6 per 100,000 (Purwanto et al., 2015). Complaints of pain in cancer patients often indicate the existence of the disease. Breast cancer pain is a multidimensional unpleasant feeling and experience associated with real breast tissue damage or breast tissue that tends to be damaged and includes physiological, sensory, affective, cognitive, behavioral, and socio-cultural components (Edrington et al., 2010; Kwekkeboom et al., 2010; NCCN, 2021).
The prevalence of breast cancer pain after treatment based on the results of a systematic review showed 29.8% among 3746 patients (Group 1: 30 studies) post-surgery, 27.3% post-radiotherapy (Group 2: 41 studies, n = 15,019), and 21.8% among breast cancer survivors (Group 3: 106 studies, n = 135,437) after receiving various breast cancer treatments (Wang et al., 2018). The cause of cancer pain is multifactorial. Pain is caused by cancer cells that grow to infiltrate the surrounding tissue and metastasize to bone or other more distant tissues through blood vessels and lymph vessels. The tumor’s suppression on the surrounding organs results in the suppression of nerves or tissue damage. Breast cancer pain can also be a side effect of anti-cancer treatments. Decreased sensory nerves after chemotherapy can lead to pain. Radiotherapy can cause pain as a result of microvascular changes and nerve compression. Likewise, surgery can be painful due to damage to the intercostal-brachial tissues and nerves. Satija et al. (2014) stated that 20%–50% of women experience persistent pain after surgery. Side effects of hormonal therapy, such as aromatase inhibitors, are often found in vaginal dryness and pain (Purwanto et al., 2015). Types of pain experienced by breast cancer patients can be categorized as acute pain, chronic pain, including injuries due to the rupture of a lump in the breast, sudden pain (breakthrough pain), and mime pain.
Pain as a stimulus will cause various responses, and people try to find comfort. Comfort is an experience gained at this time that is supported by meeting the needs for liberation (relief), calm/serenity (ease), and being highly qualified (transcendence) in four contexts (physical, psychospiritual, sociocultural, and environmental) to the absence of pain or another physical discomfort (Alligood, 2021). Comfort is the result of interventions to relieve distress or causes of discomfort. The consequence of comfort is a feeling of peace, reduced symptoms such as reduced pain, reduced suffering, and freedom from discomfort (Siefert, 2010). Breast cancer patients’ psychological conditions and coping conditions affect comfort. Nurses respond well to the need for physical care and, with compassion, help reduce psychosocial distress and make patients feel cared for.
Pain is also a major factor affecting the quality of life of cancer patients. Pain affects the quality of life of cancer patients because pain affects individuals physically, socially, psychologically, and spiritually. Black et al. (2011) stated that pain correlated significantly with fatigue, anxiety, appetite, comfort, symptom control, and overall quality of life.
The development of innovative pain relief tools with rubbing massage with massage and rubbing techniques is needed. Massage rubbing the back with the hands is a pain reduction technique with gentle rubbing when pain occurs. Besides improving blood circulation, the benefits of back rubbing massage can also reduce pain through the gate control mechanism, including cancer pain. DRM Pain Relief reduces pain and increases comfort and the shorter active phase of labor in primiparous mothers (Sudirman et al., 2019). The use of DRM Pain Relief will provide a stimulus to the large nerve fibers. It will increase the activity of the substantia gelatinosa, which results in the closing of the pain control gate mechanism so that T cell activity is inhibited and causes the conduction of pain impulse stimulation also to be inhibited. Gelatinosa substance located at the dorsal end of the spinal cord nerve fibers acts as a pain control gate that can modify and change the pain sensation before it reaches the cerebral cortex (brain). The DRM Pain Relief tool is used to close the door of defense/gate of control based on the theory of gate control of pain so that pain impulses do not reach the brain and the patient does not feel pain. Thus, the patient is pain-free, feels comfortable, and improves the quality of life. This study aimed to analyze DRM Pain Relief tool effectiveness on the degree of pain, comfort, and quality of life among breast cancer patients.
Methods
Design
This study was a true experimental study with a randomized pre-test and post-test control group design to identify the effectiveness of DRMPain Relief on the degree of pain, comfort, and quality of life before and after being given treatment. The experiment group received conventional therapy and digital massage rubbing for about 30 min (2 × 15 min with a break time was about 15 min). Meanwhile, the control group received only conventional therapy (drugs).
Research Questions
The question of this study was “Does digital rubbing massage-pain relief (DRM Pain Relief) can reduce pain and increase comfort, and life quality among breast cancer patients?”
Sample
The research participants were 64 breast cancer patients attending the oncology ward of two hospitals in Pekalongan and Semarang District, Central Java, Indonesia and met the inclusion and exclusion criteria. They were randomly selected and divided into a treatment group (DRMPain Relief Application) and a control group (conventional intervention). The total sample of each group was 32. This sample size referred to the determination of the sample size for the difference in the mean of two paired groups because all the dependent variables were of numerical data scale, and data were taken from pre- and post-test groups (Sastroasmoro & Ismael, 2011). With a Type I error (α) of 5%, Zα: 1.96, power of test of 80%, Zβ: 0.842, standard deviation of the mean difference (Sd) from the literature, and the clinically important difference (d) of the mean of the two groups from clinical judgment. The formula for determining the sample size is:
n: required sample size in each group
Sd: standard deviation of the mean difference (Sd from the literature)
d: clinically important difference (clinical-judgment) of the mean of the two groups
Zβ: Z table value for β is 0.842
Zα: Z table value for α: 5% is 1.96.
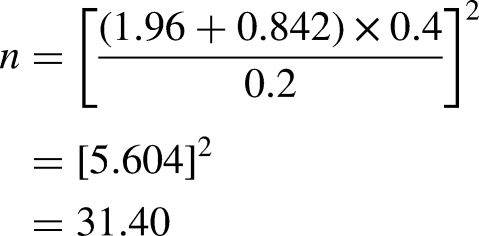
The standard deviation of the mean difference (SD) and the mean difference between two groups (d) used in the study conducted by Black et al. (2011) titled “The Relationships Among Pain, Nonpain Symptoms, and Quality of Life Measures in Older Adults with Cancer Receiving Hospice Care” was the variable degree of pain. The sample size in Black et al.'s (2011) study was 35 for the patient group and 36 for the caregiver group. The mean difference of the “average pain” reported by both groups (patient and caregiver) was 0.2 (mean: 2.45–2.43) and the standard deviation of the mean difference was 0.4 (SD: 2.74–2.34). If entered into the formula above, the sample size measurement in this study was:
Inclusion/Exclusion Criteria
The inclusion criteria were: female patients with a positive diagnosis of breast cancer, have the best level of consciousness, complained of pain for at least the last 24 h, have moderate pain intensity (pain scale 4 to 6), performance status with a minimum Karnofsky scale value of 50%–60%, have minimum secondary school education or equivalent, and willing to be a respondent.
While the exclusion criteria were: patients with Pain Controlled Analgesia installed, patients who became very weak/decreased consciousness, and breast cancer patients with bone metastases.
Research Ethics, Patient Consent, and Data Collection
This study follows the rule in the WMA Declaration of Helsinki-Ethical principles for medical research involving human subjects.
The researchers obtained ethical approval from the Health Research Ethics Committee of Health Polytechnic Semarang (No. 0306/EA/KEPK/2022) and the Health and Research Ethics of Tugurejo Public Hospital Semarang (No. 076/KEPK.EC/IX/2022). The researcher took data from September to November 2022.
Upon ethical approval, formal permission to collect the data was requested from the head of the nursing colleges Health Polytechnic Semarang to the Research Office and Health Office of Pekalongan Regency. Following this process, the researcher requested formal permission from the hospital, selecting three nurses from Kraton Hospital Pekalongan to become data collectors and giving them related training to ensure that nurses deeply understand the research and massage procedure. The nurses approached each potential participant and asked about their availability to become a participant. For data collection in Tugurejo Hospital, Semarang also followed a similar procedure.
Before performing massage using DRM Pain Relief, the data collectors gave brief explanations about the research purpose and the steps of intervention to the potential participant. They also received information about the research's benefits and risks. If participants agreed to participate, the researcher gave an informed consent form to be signed by the participant. Participation in this study was voluntary. There was no pressure to be a participant, which means potential participants could freely refuse and withdraw their participation at any time. The researcher ensured patient privacy during the treatment by not permitting other people to enter the room during the intervention. After signing informed consent, participants followed a pre-test about the current pain level, comfort level, and quality of life. For intervention group received massage using DRM Pain Relief twice in the first day and twice on the second day. Twice means each day, patients received the first massage for about 15 min, then took rest for 15 min, and continued with the double massage for 15 min. The total duration of massage was 30 min each day, meaning during two days the participants received a total of 60 min.
The procedure of massaging using DRM Pain Relief followed these steps: (1) Wash your hands; (2) Put on gloves; (3) Help the client to a comfortable position to focus on the area of pressure, which is the area around the pain; (4) Check the completeness and readiness of the DRM Pain Relief equipment (pads, remote, flash disk, android/notebook), make sure the potentiometer is in position 0 (turn to the left until it stops); (5) Insert the jack cable pad into the connector on the front twice (must be four pads, cannot be just one pair); (6) Turn on the device by pressing the On button (red) on the front left, the LCD will light up and load the file. Select the main menu (select USB if using memory file or select line if using android/notebook); (7) Attach two pairs of pads to the area around the pain; (8) Turn the potentiometer to the right to the position that the client considers the massage strength to be sufficient, massage can be done for approximately 30 min twice (digital massage rubbing for 15 min—rest for 15 min—digital massage rubbing for 15 min); (9) After the 15 min of each digital massage rubbing, turn the potentiometer back to position 0, remove both pairs of pads, attach the pads to the pad place so that the gel pad layer remains sticky and the pad can be reused; (10) The DRM Pain Relief device can be turned off by pressing the off button; (11) After two installations of the device, position the potentiometer to position 0, remove all attached pads, then press the off button; (12) Position the client comfortably again; (13) Remove the gloves and wash your hands; and (14) The DRM Pain Relief device can be charged with its battery (charge with the charger) during the rest period or if the battery power is low. Charging the battery can also be done simultaneously with the device in the “On” condition (in use).
The data of post-first intervention was taken after intervention on the first day. In the next day (within 24 jam), the patient received such intervention, and the second post-intervention data was taken on the second day. The interventions were held in the morning.
If there were any discomfort during treatment, the researchers stopped the process, did an evaluation and gave patients time to rest. If those patients were available to continue the treatment, the treatment would be continued. Otherwise, the treatment would be stopped and then moved to other patients.
The researchers also kept the data confidential; no name was mentioned in the data collection. All collected data were kept safely in the researcher's private laptop and will only be used for academic purposes.
Research Instrument
To perform massage, DRM Pain Relief tool was used. In a previous study, researchers designed DRM Pain Relief tool in collaboration with an electro-medical expert to develop this tool for research and development design (R&D). The DRMPain Relief tool has passed a qualitative study and has been tested for the instrument's feasibility. It was tested on 20 Normal people in Semarang, Indonesia. The feasibility test results for the DRM Pain Relief tool show that the frequency of the device was 100 Hz, and the current generated and used on the device was 1–3.5 mA, while the maximum allowed current was 50 mA (Figure 1 and Table 1).

The design and prototype of DRMPain Relief.
Description of DRM Pain Relief Components.

Inside components:
- Two pairs of electrode pads - Dimensions: 20 × 16.5 × 7 - Materials - Input voltage: 9 V DC / 2 A - Output current: Max 4.19 mA.
Wairing
The results of the DRM Pain Relief tool trial in normal people are shown in Table 2.
The Result of Testing of DRM
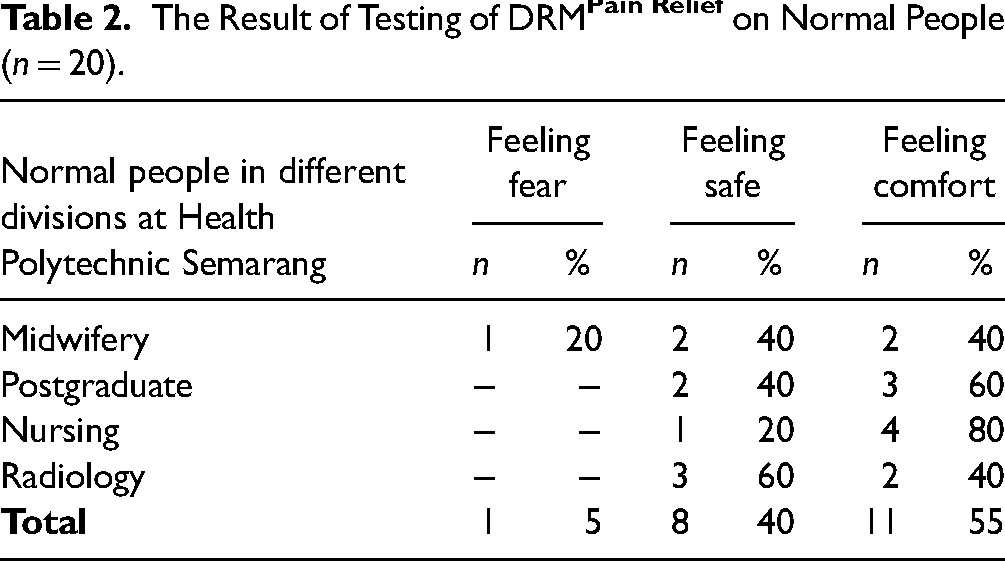
These results indicate that the DRMPain Relief tool is felt to be 95% safe and comfortable by the respondents (Figure 2).

Inside components and structure of DRM Pain Relief.
To collect the targeted data, the researchers used these instruments: Brief Pain Inventory (BPI) (Cleeland, 1991), Comfort Scale (Lee, et.al 2014), and the European Organization for Research & Treatment of Cancer Core Quality of Life Questionnaire (EORTC QLQ – C30) (Aaronson et al., 1993), and the Supplementary Breast Cancer Module (QLQ – BR23) (Radisic & Schafer, 1996).
Cleeland created a BPI to measure patients’ pain scale. It consists of nine questions using a Likert scale of 0–10. While the Comfort Scale created by Lee was used to measure patients’ comfort levels. It is used as a picture to describe the level of comfort, 0 means very uncomfortable, and 10 means very comfortable (Lee et al., 2014).
The European Organization for Research & Treatment of Cancer Core Quality of Life Questionnaire (EORTC QLQ – C30) was created by Aaronson to measure patients’ quality of life. The QLQ-C30 consists of nine multi-item scales: five functional scales (physical, role, cognitive, emotional, and social); three symptom scales (fatigue, pain, and nausea and vomiting); and a global health and quality-of-life scale. Several single-item symptom measures are also included. Several single-item symptom measurements are also included (Aaronson et al., 1993).
In 1996, the BR-23 questionnaire was created to assess breast cancer patients’ quality of life. Many treatments and diagnosis changes have occurred during the past few years. Twenty-two new questions were added to the QLQ BR-23, which was updated.
Statistical Analysis
The data were analyzed using simple and multiple linear regression. The authors used the SPSS version of 23, 2015, and controlled other variables such as age, emotion, family support, type of medication, finance, pain experience, and cancer stage.
Results
Sample Characteristics
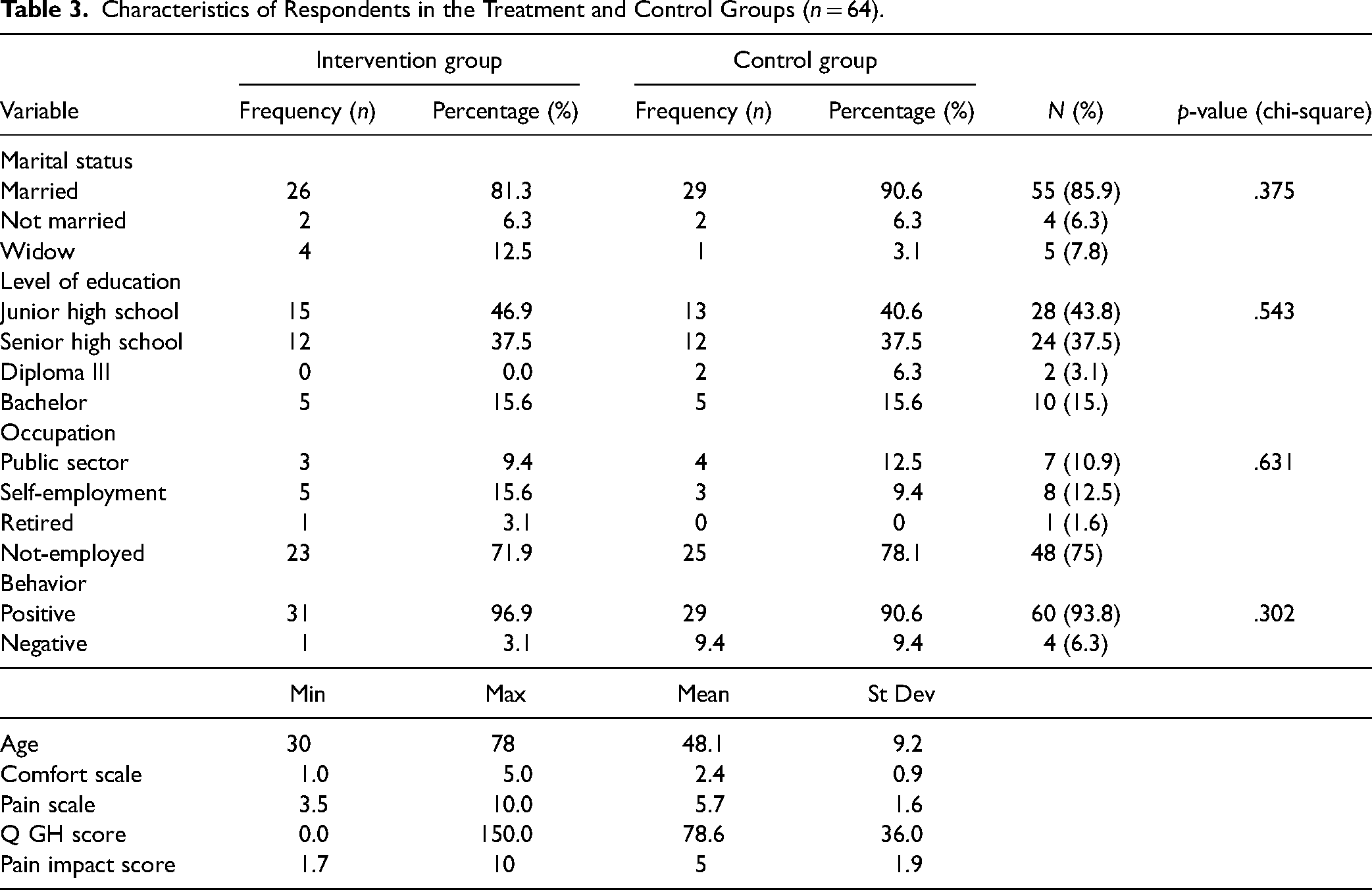
The characteristics of the respondents between the intervention and the control group can be seen in Table 3. The characteristics data of marital status, level of education, occupation, and behavior were homogeneous.
Characteristics of Respondents in the Treatment and Control Groups (n = 64).
Effectiveness of Using DRM-Pain Relief on Pain, Pain Effect, Comfort Score, and Quality of Life
The effectiveness of DRMPain Relief on pain, pain effect, comfort score, and quality of life after controlling for pre-pain scores, age, emotions, family support, drug, finances, pain experience, and cancer stage can be seen in Table 4 and Figure 3.

Effectiveness of Using DRM-Pain Relief on Pain, Pain Impact, Comfort Score, and Quality of Life.
Effectiveness of Using DRM-Pain Relief on Pain, Pain Effect, Comfort Score, and Quality of Life.

Effectiveness of DRMPain Relief on the Degree of Pain in Breast Cancer Patients
A brief pain questionnaire (BPI) measured the degree of pain. The measurement results were expressed by a pain score of 0 (no pain) to 10 (severe pain). After the first DRM Pain Relief intervention, the pain score decreased significantly by 2.62 (p < .001). The use of DRMPain Relief affected reducing 75.6% pain scores. Moreover, after the second intervention, the pain score decreased by 2.09 (p < .001); which means the use of DRMPain Relief had an effect of 40.0% in reducing pain scores.
Effectiveness of DRM-Pain Relief on Pain Impact Score
In the first intervention, the use of DRMPain Relief decreased the pain impact score by 2.43 (p < .001), and had an effect of 47.8% in reducing the pain impact score. After the second intervention, the pain impact score was lower (1.79, p < .001), which means that the use of DRMPain Relief had an effect of 25.8% in reducing the pain impact score.
Effectiveness of DRMPain Relief for the Comfort of Breast Cancer Patients
Regarding the comfort score, using DRMPain Relief post-first intervention increased the comfort score by 3.48 (p < .001); 83.3% in increasing the comfort score. After the second intervention, the comfort score increased by 5.61 (p < .001). The use of DRMPain Relief had an effect of 88.1% in increasing the comfort score.
Effectiveness of DRM−Pain Relief to Global Quality Life Score (GH Q Score)
DRM-Pain Relief could increase the Q GH score by 17.91 (p = .001). The use of DRM-Pain Relief had an effect of 18.1% in increasing the Q GH score. After the second treatment, DRM-Pain Relief increased the Q GH score by 37.39 significantly (p < .001); 46.5% increased the Q GH score.
Discussion
DRM Pain Relief Tool
The PDA (Pain Digital Acupressure) tool is the base of the development of the DRM Pain Relief tool. The difference between this tool and a PDA device is that the DRM Pain Relief tool uses sine waves and binual beats to produce a rubbing sensation and is combined with the Android/Note Book application (Figure 4). In contrast, the PDA tool uses square waves and does not use the Android/NoteBook application. The development of a DRM Pain Relief tool is necessary because doing massage and rubbing simultaneously using your fingers is very inefficient and tiring because the appearance of pain can occur at anytime and anywhere. With the development of the DRM Pain Relief tool, it is hoped that breast cancer patients can deal with pain independently.
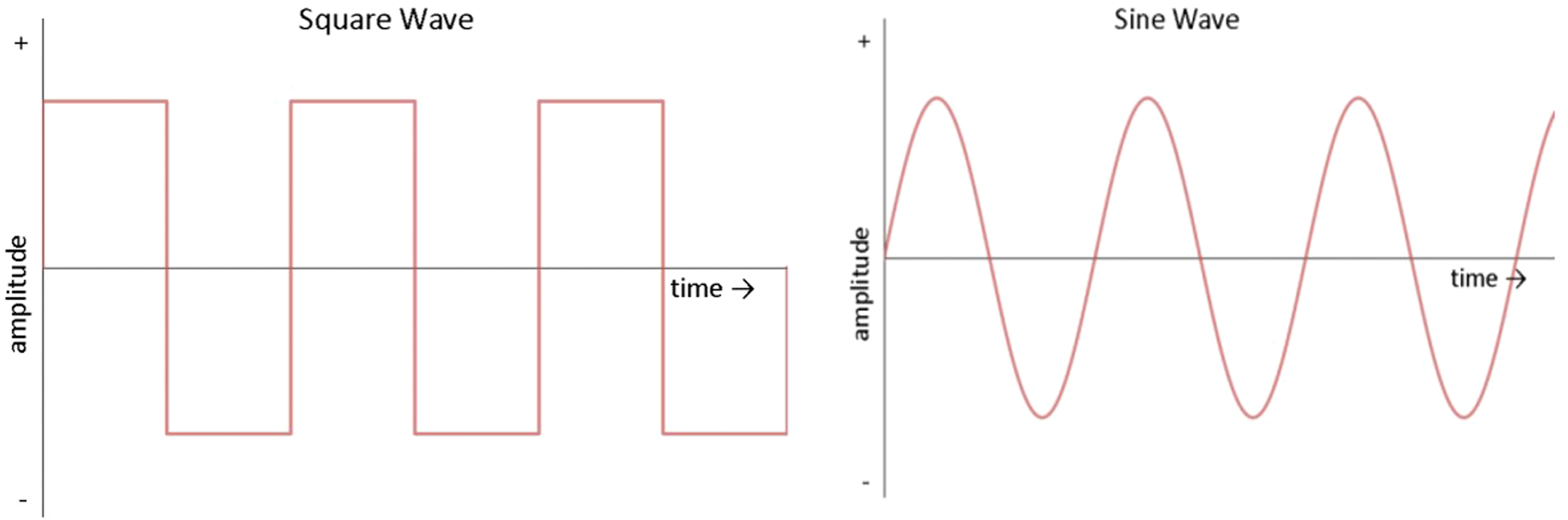
Types of sine and square waves.
Sine waves were used because, based on the identification of wave characteristics, the most comfortable response was a sine wave (65%). These results followed Petrofsky's study (2009), which states that square waves give more pain sensation than sine waves. The breast area is sensitive and requires a gentle/delicate touch. The following forms a sine wave type compared to a square wave.
Sine waves were characterized by gradually increasing and then decreasing in amplitude. In contrast, square waves were characterized by increasing rapidly, then experiencing plateaus within a certain period, and falling suddenly. The principle of this wave is the faster it increases in amplitude (rate rise), the greater the ability of the wave to generate a neural network (Prentice, 2002).
The main difference between DRM Pain Relief tools and the other tools available is that DRM Pain Relief tools use sine waves and binual beats. It provides a rubbing massage sensation different from PDA tools, Modified Pain Digital Acupressure, and Digital Massager Oxytocin, the average TENS uses square waves and has no rubbing massage (stroking/gentle touch/massage).
Effectiveness of Using DRM Pain Relief on the Degree of Pain Among Breast Cancer Patients
The result of this study indicates that DRM Pain Relief effectively reduced pain among breast cancer patients. The initial mean degree of pain among the intervention group was 5.7, which decreased to a scale of 3.3 after the first intervention and 1.6 after the second intervention. Using DRM Pain Relief reduced pain scores, namely 75.6% at post-first intervention and 40% at post-second intervention. Those also decreased the impact pain score after the first and second interventions to 47.8% and 25.8%, respectively. These results prove that DRM Pain Relief could significantly reduce the degree of moderate pain to mild pain. In contrast, the pain in the control group remained high, namely 5.7 in the initial measurement and 3.6 in the last measurement on the second day.
Pain is influenced by the activity of large and small nerve fibers in the dorsal root ganglion. The use of DRM Pain Relief will provide a stimulus to the large nerve fibers. It will increase the activity of the substantia gelatinosa, which results in the closing of the mechanism door so that T cell activity is inhibited and causes the conduction of pain impulse stimulation also to be inhibited. Gelatinosa substance located at the dorsal end of the spinal cord nerve fibers acts as a pain control gate that can modify and change the pain sensation before it reaches the cerebral cortex (brain). DRM Pain Relief tool might close the defense/control gate door based on the pain gate control theory proposed by Melzack and Wall in 1965. However, the real measurement of endorphin levels has not been carried out in this study. Brain-produced endorphins serve as the body's natural pain relievers. Endogenous morphine, or endorphins, are opioid neuropeptides naturally generated in the body. Their primary function is to inhibit pain perception, but they are also present in instances of pleasure (Chaudhry & Gossman, 2022).
Finding that massage using DRM Pain Relief tool could reduce pain among cancer patients supported a previous study that oncology massage therapy has the potential to provide substantial health benefits to both cancer patients and survivors (Galamaga & Cristian, 2021).
Desen and Japaries (2011) state that the obstacles associated with patients and their families in managing cancer pain are misunderstandings about pain. The patient does not want to recognize pain as it is, worried that it will be judged as a bad patient, so they are more silent. According to Naveh et al. (2011), 18% of patients did not ask for pain medication even though they felt pain. Moreover, 66% of patients did not ask about the form of pain management; even patients did not ask when pain medication did not show results in reducing the degree of pain. When diagnosed with breast cancer, there is a high probability of recurring pain attacks because the nature of cancer pain can be minimized but cannot be completely lost, it can even become persistent pain as cancer cells become more active in the body (Desen & Japaries,2011; Harmer, 2011). Pain management remains crucial for patients with breast cancer.
This study showed that the degree of pain was far lower after the second treatment using DRM Pain Relief tools than the degree after the first treatment. This result supported a previous study on the effect of foot massage on upper extremity pain level and quality of life in breast cancer patients who underwent mastectomy indicated that foot massage was effective in reducing pain but less effective in improving quality of life (Demirci et al., 2022). In addition, Liu et al. (2022) reported that massage therapy is effective for reducing postoperative pain; a similarly significant effect was discovered for both brief (immediate assessment) and long-term (assessment performed 4–6 weeks after the massage therapy).
The use of DRM Pain Relief tools has been proven to provide effective results for managing cancer pain, especially for more than once time treatment. Thus, healthcare providers, especially those working with breast cancer patients, are strongly encouraged to practice repeated massage using DRM Pain Relief tools to improve positive outcomes and reduce pain of breast cancer patients.
The Effectiveness of Using DRM Pain Relief for the Comfort of Breast Cancer Patients
The research has proven that DRM Pain Relief effectively increases the comfort of breast cancer patients. The initial comfort score between the treatment and control groups was the same (2.4). After using DRM Pain Relief on the first day, the comfort score increased by 3.48 (83.3% of increasing). After the second intervention, the comfort score increased by 5.61, which means it had an effect of 88.1% in increasing the comfort score. On the other hand, the comfort score of the control group was only 0.6 post-first intervention and 0.3 post-second intervention. It indicates that the increasing comfort score of the intervention group was higher than the control group. This condition is clinically beneficial for breast cancer patients in overcoming the problem of discomfort, as comfort is a basic need that everyone, whether healthy or sick, needs. The study showed that breast cancer patients’ psychological and coping conditions affect comfort (Cipila et al., 2020). Feeling comfort is important as a positive aspect representing a positive outcome as the ultimate goal of nursing. Pain in breast cancer patients affects physical comfort, sleep rest, psychological comfort, and social comfort, resulting in a decrease in the quality of life of cancer patients (Putri et al., 2022). Thus, managing pain and comfort is essential.
The results of this study are also relevant to Lara-Palomo et al’s study (2012), that interferential current electro-massage overcomes disability and pain and improves the quality of life in patients with low back pain. Rubbing massage will stimulate or relax the body muscles from the tension that arises. Physical relaxation is parallel to mental relaxation, meaning that a relaxed mental state will accompany a relaxed physical state (Soewondo, 2012).
Increasing comfort score also correlates with the decrease of pain score. In this study, while the pain score decreased, the comfort score increased. It follows the results of Schuiling's study (2010), which states that there is a correlation with the direction of a negative relationship between comfort and pain in breast cancer patients; the assessment of pain scores increases, and conversely, the comfort score decreases.
This study also showed that the comfort score was higher after the second treatment (increased by 5.61) compared to the first treatment (only increased by 3.48). This result supported a previous study that used repeated treatment as the treatment procedure in research to improve the outcomes. Guney & Ucar (2021) reported that the comfort level of the experimental group participants who had received deep tissue massage (DTM) was higher than that of the control group participants. Participants in the experimental group received DTM twice (10 and 22 h) after cesarean delivery.
Since this study showed that The DRM Pain Relief effectively helped breast cancer patients deal with pain and increase comfort, healthcare providers are encouraged to use The DRM Pain Relief as an alternative solution to manage pain and discomfort among breast cancer patients. They should apply this treatment not only once but several times to gain better results.
The Effectiveness of Using DRM Pain Relief on the Quality of Life of Breast Cancer Patients
The results of this study indicate that the use of DRM Pain Relief increased the global quality of life score by 17.91 and had an effect of 18.1% in improving the global quality of life score after the first intervention. This increase was significant when compared to the control group. Most cancer patients could achieve a reduction in pain and improve their quality of life within one to two weeks. This study supported a previous study conducted by Damodar et al. (2013) which showed that physical dimension, role functioning, and future perspectives significantly influence the quality of life. Massage using DRM Pain Relief can be categorized as a physical dimension. Similarly, Qomar Wani et al. (2012) conducted a health-related quality of life assessment on breast cancer survivors with follow-up at the first visit, six months, 12 months, and 24 months. They found that physical functioning, role functioning, cognitive functioning, emotional functioning, social functioning, global health status, and symptomatology showed a significant development statistically (p < .001). The increase in functional status caused the patients to have a more positive perception of their global health status, thus driving the achievement of an optimal global quality of life.
Global health status determines healthy behavior affecting the overall quality of life. Suppose the quality of life of breast cancer patients is not optimal. In that case, it will worsen functional and symptom status, making it difficult for patients to actively participate in everyday activities to the best of their ability. Damodar et al. (2013) stated that the global health status of breast cancer patients is influenced by physical function, social function, body image, future perspective, insomnia symptoms, and breast and arms symptoms. In this study, DRM Pain Relief helped patients to get better quality of life. Based on the current symptom status of breast cancer patients, DRM Pain Relief has been proven to help change the existing symptom status. This study showed that the symptom status in the treatment group experienced a significant decrease in scores from pre-test to post-test 2 (p < .001). In the control group, symptom status remained stable from post 1 to post 2. This study reinforces the research conducted by Janz et al. (2017), which sought to investigate the relationship between symptoms and quality of life of post-treatment breast cancer patients (surgery, chemotherapy, or radiation). The average reported symptom was 6.18 (range 1–13), with the six most common symptoms being systemic therapy side effects (87.7%), fatigue (81.7%), breast symptoms (72.1%), sleep difficulty (57.1%), arm/hand swelling (55.6%), and pain (51.7%). The research findings concluded that improving symptom status could enhance the quality of life among women with breast cancer.
A further study by Winnie et al. (2010) indicated that the symptom cluster of fatigue, pain, anxiety, and depression affected the quality of life in female breast cancer patients receiving chemotherapy or radiotherapy treatment. Most respondents reported pain and fatigue at a mild to moderate level, anxiety (21%), and depression (36%). Respondents undergoing chemotherapy with inadequate social support experienced worse symptom status and had lower quality of life. Thus, improving the global quality of life is essential. Healthcare providers, particularly those who work with breast cancer patients, are encouraged to repeatedly perform messages using DRM Pain Relief to help patients gain a better quality of life. Hopefully, by giving therapy using DRM Pain Relief, breast cancer patients could have higher score in quality of life, as this study showed that the global quality of life score increased even higher after the second treatment (37.39, 46.5% increasing).
Strengths and Limitations
This study only measured the degree of pain through a pain scale and did not measure biomarkers (endorphins) indicating the presence of endogenous analgesics. However, this study remains beneficial and innovative as DRMPain Relief is a novel treatment for breast cancer patients. The use of an instrument such as pain scale, comfort scale, and quality of life scale is also already standardized.
Implications for Practice
DRMPain Relief is a digital rubbing massage tool to reduce the pain that can be integrated into the nursing care of breast cancer patients. DRMPain Relief provides a more concrete form of pain management in nursing care as a real treatment that can be carried out independently by the patient at any time of pain attack. Treated pain will increase patient comfort. So, patient satisfaction with nursing services is expected to increase. In addition, integrating this tool into nursing care in hospitals and health centers might provide independent learning in managing pain and change patient perceptions of dependence on pain medication.
The authors recommend to the Department of Non-Communicable Disease Control, the Ministry of Health of the Republic of Indonesia to use DRM Pain Relief as pain management in hospitals, pain management centers, pain clinics or palliative care units to support the achievement of a Cancer pain-free Indonesia.
Conclusions
DRM Pain Relief uses electromedical principles with a 100 Hz sine wave, binual beat for a massage-rubbing sensation combined with an android/notebook application, an amplitude of 3.5 mA, and an installation time of 30 min. The DRM Pain Relief application effectively reduced the degree of pain, increased comfort and improved the quality of life of breast cancer patients.
Breast cancer patients are expected to be able to independently use the DRM Pain Relief tool to manage pain and discomfort and optimize quality of life. Further research can be conducted to examine endorphin hormone levels using human beta-endorphin ELISA and satisfaction studies using DRM Pain Relief.
Footnotes
Acknowledgments
Thank you to the Directorate General of Health Workers of the Republic of Indonesia and the Semarang Ministry of Health Polytechnic for funding the implementation of this research; Head of the Semarang Nursing Study Program; Director of Kraton Hospital, Pekalongan Regency & Director of Tugurejo Hospital, Semarang.
Author Contributions
All authors conceptualized the study, analyzed, and interpreted the data. All authors reviewed and contributed to the intellectual content of the paper. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
This study follows the rule in the WMA Declaration of Helsinki-Ethical principles for medical research involving human subjects (WMA General Assembly, 2013). We obtained ethical approval from the Health Research Ethics Committee of Health Plythechnic Semarang (No. 0306/EA/KEPK/2022), and from Health and Research Ethics of Tugurejo Public Hospital Semarang (No. 076/KEPK.EC/IX/2022). The researcher took data from September to November 2022.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by The Ministry of Health Republic Indonesia.