
Abstract
Introduction
Trust is a fundamental aspect of the patient–health care provider (HCP) relationship associated with adherence to medical treatment and continuity of follow-up. Despite its importance there is a paucity of information in Ethiopia.
Objectives
This study aimed to assess patient trust in HCPs at the Jimma medical center (JMC), Ethiopia.
Methods
An institution based cross-sectional study was conducted among 404 participants from April 16 to June 29, 2020. Study participants were selected using a systematic sampling technique. Data were collected on socio-demographic characteristics, health related and clinical characteristics, and patient trust in the patient–HCP. The collected data were entered into Epi-Data version 3.1 then exported to SPSS version 23.0 for analysis. Variables with a p-value <.25 on bivariate analysis were considered as candidates for multivariate analyses. Statistical significance on multivariable analysis was declared with p-value < .05 and 95% confidence intervals (CI).
Results
In our study, 38% of patients had low trust. Among the 397 study participants, 46.6% were female. One-third (33.2%) of respondents had no formal education. Patients who live alone [(AOR) 4.30(1.98–9.33), p = .00], and self-reported as a poor current health status [(AOR) 2.32(1.39–3.88), p = .002] were positively associated to patient trust in patient–HCP. On the other hand, duration of disease more than one year after diagnosis [(AOR) 0.48 (0.25–0.92), p = .028], comorbid disease [(AOR) 0.39(0.22−0.67), p = .001], and impaired physical mobility [(AOR) 0.27(0.16−0.45), p = .001] were negatively associated with patient trust in HCP.
Conclusion
This study pinpoints that 38 out of 100 patients had low trust. Living alone and having poor self-reported current health status increased low trust. This calls for HCPs to rebuild trust and give due attention to patients living alone and with poor health status.
Introduction
Patients’ trust in their health care provider (HCP) has been defined as “the belief that a care provider is working in the patient's’ best interests” as well as the optimistic acceptance of the vulnerable situation in which patients believe that the HCPs care for their interests. People's trust with their physician and, generally, with a provider is vital to the care process. It can modify patient attitude and behavior which can result in better levels of treatment, increase acceptance of medical suggestions and compliance with treatment recommendations and improve motivation to seek help and use preventive care (Brown, 2018).
Hospitalized patients are often required to place all of their trust in their care providers, a person with whom no close relationship exists, because of their inability to care for themselves (Brown, 2018). Trust is essential for cooperation, coordination, and performance at all levels of human interaction: at the individual (person to person), group or community level, and organizational levels (Adam & Donelson, 2022).
The nature of trust its definition and measurement, as well as the question of how it influences and changes human interactions is addressed across multiple academic disciplines, including psychology, economics, anthropology, sociobiology, history, and management (Adam & Donelson, 2022). Trust focuses more on the future, the expectations concerning accuracy of diagnosis and the result of treatment and motivation of the HCP and significantly affects the strength of the relationship between the patient and the HCP. Moreover, trust enhances communication between health care and patients as well as the perception of efficacy, self-reported health status well-being, and quality of life (Lewandowski, 2011).
Review of Literature
When patients have a high level of trust in health-care professionals, it will be associated with increased willingness to seek medical treatment, increased use of preventive health services, greater compliance with treatment recommendations, satisfaction with recommendations, satisfaction with medical care, symptom improvement (Brennan et al., 2013; Yucel & Ay, 2013), less development of depression, and improvement in the detection of depression in patients with chronic medical conditions (Bova et al., 2012). In contrast, low patient–provider trust can lead to poor treatment adherence and patients are more likely to leave a hospital against medical advice and negative health outcomes (Bova et al., 2012).
Trust in a provider may reduce the number of conflicts between patients and medical staff, diminish the probability of complaining about medical malpractice, lower transaction costs (e.g., expenditures that can decrease patient anxiety by using additional diagnostic testing and physician consultation), and increase motivation to recommend the HCP to others. Trust is influenced by different factors such as age, educational level, income, gender, and length of time with HCPs (Hall et al., 2002). To date, there is widespread concern that patient trust in HCPs is declining worldwide. As a result, low institutional trust may cause inefficiency and undermine the legitimacy of health insurance and eventually decrease solidarity as well as overall success of health policy (Zhao et al., 2016).
Thus, an emphasis on the importance of research factors that may affect the level of trust in healthcare become seeming fundamental. Although patient trust in the HCP is unquestionable, there is a paucity of information in Ethiopia. Thus, the current study aimed to assess patient trust in HCP which may have more clinical significance.
Methods
Study Design and Setting
This cross-sectional study was conducted from 16 April to 29 June 2020 at the Jimma Medical Center (JMC), Ethiopia. JMC is located 352 km Southwest of Addis Ababa, which is one of the oldest hospitals in Ethiopia and was established in 1930. The hospital provides inpatient, outpatient, emergency, delivery, and pharmaceutical services. On average, 1565 patients were admitted to the JMC for two months.
Research Questions
What is magnitude of patient trust in health care provider?
What are factors associated to patient trust in health care provider?
Sample Size Determination
The sample size was determined by using single population proportion formula by considering the following assumptions. The formula for the single population proportion is:

Where: -
n = sample size
Zα/2 = confidence level at 95% which is 1.96
p = estimated prevalence level 50% since there is no previous study in Ethiopia.
d = margin of error of 5%
After adding a non-response rate of 5%, the final sample size was 404.
Eligibility Criteria
This study included patients aged ≥15 years who were hospitalized for at least two weeks during the study period. Patients who cannot give full information like patients in the intensive care unit, with psychiatric disorders, speaking and hearing problems were excluded.
Sampling Technique and Procedure
A systematic random sampling technique was employed after proportional allocation according to the number of patients in each ward. Prior to the actual data collection, patients who came for two months were obtained from the patient registration logbook and the average was taken from each ward. In two months, there were 671 inpatients in surgical ward, 595 admitted patients in medical unit, 142 hospitalized patients in gynecology and maternity ward, while 157 patients were admitted to maxillofacial unit which gave 1,565 total number of patients admitted to JMC and the interval was calculated by using k-value = 1,565/404 = 4.
The patients’ medical registration number was used as the sampling frame to select individual study participants. The first patient card number was given a unique code to ease the procedure; then the first participant was selected using the lottery method and the second patient was selected after four intervals from the first patient from the list of the unique code. Therefore, the first random card was used to obtain the first patient for whom data was collected in each ward until the required sample sizes were obtained. Of 404 participants, 397 were interviewed which made response rate 98.3%.
Operational Definition
Results
Sample Characteristics
Among the 397 study participants, 36.5% of them were found between 31 and 45 years and 46.6% of them were female. One-third (33.2%) of respondents had no formal education. Over half (57.2%) of the respondents were married. Half of (49.6%) participants lived with three or more persons (Table 1).
Socio-Demographic Characteristics of Patients’ Trust in Health Care Providers Among Hospitalized Patients, Jimma, South West Ethiopia.

Health-Related and Clinical Characteristics
From total study participants, more than one-third (37.8%) had comorbid diseases. More than half (62.7%) of the respondents had lived with the disease less than 179 days. One-fourth (26.4%) of the respondents had stayed in the hospital greater than 30 days after admission. Approximately175 (44.1%) of the patients had poor self-rated status of health and 37.8% of the participants had impaired mobility. Approximately 42.9% of the study participants had emergency care visits before the current admission and 181 (45.6%) of respondents had been hospitalized in the last year before the current hospitalization (Table 2).
Health-Related and Clinical Characteristics of Patients’ Trust in Health Care Providers Among Hospitalized Patients, Jimma, South West Ethiopia.

Patient Trust in HCP
Figure 1 presents patient trust in HCPs. About 62% had high trust toward their HCPs and more than one-third of (38%) patients had poor trust toward their HCPs (Figure 1).
Patient trust in health care provider among hospitalized patients, Jimma, South West Ethiopia.
Factors Associated With Patient Trust in HCP
All study variables were tested by binary logistic regression analysis and nine variables had p-values less than .25 and those variables were candidates for the multivariate logistic regression to control for confounding variables and to determine potential predictors of patient HCP trust (Table 3).
Binary Logistic Regression Analysis of Factors Associated to Patients’ Trust in Health Care Providers Among Hospitalized Patients, Jimma, South West Ethiopia.

HCP
Multivariable Logistic Regression Analysis of Factors
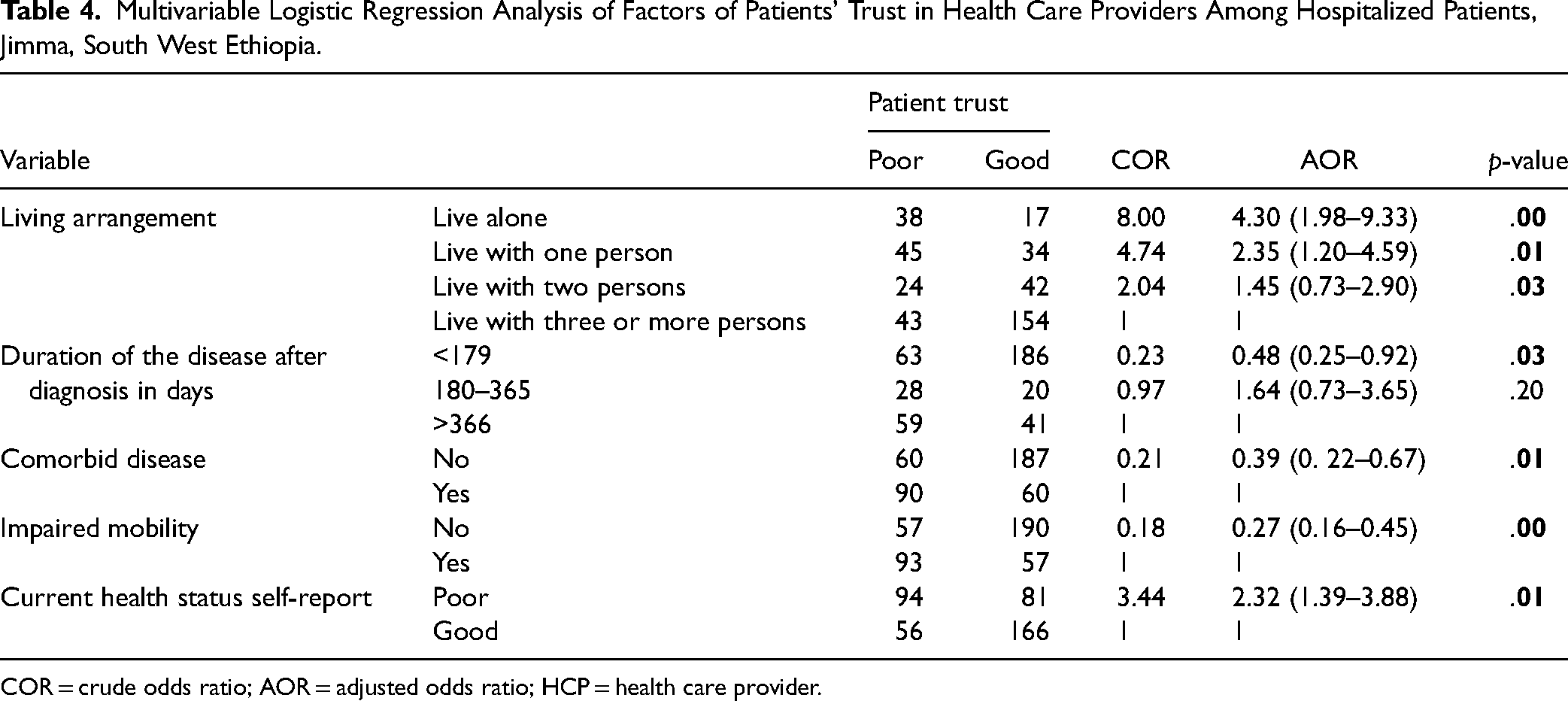
On multivariate logistic regression, five variables were found to be significantly associated with patient HCP trust. This finding showed that patients who lived alone [(AOR) 4.30(1.98–9.33), p = .00], patients who had a duration of greater than one year after diagnosis [(AOR) 0.48 (0.25–0.92), p = .028], patients who had comorbid disease [(AOR) 0.39(0.22–0.67), p = .001], patients who had impaired mobility [(AOR) 0.27(0.16–0.45), p = .001], patients who self-reported as poor current health status [(AOR) 2.32(1.39–3.88), p = .002] were significantly associated with patient HCP trust (Table 4).
Multivariable Logistic Regression Analysis of Factors of Patients’ Trust in Health Care Providers Among Hospitalized Patients, Jimma, South West Ethiopia.
COR
Discussion
Despite the current evidence on the positive impact of patient trust on health outcomes (Chandra & Mohammadnezhad, 2020), there are no studies that have been conducted in Ethiopia. Thus, we are the first to conduct patient trust in HCPs among hospitalized patients at the Jimma medical center, Ethiopia. We found that more than one-third of the patients had low trust in their HCP. This implies that patients’ low trust in healthcare is associated with an increase of medical negligence, complaints, display of lack of concern and knowledge of trust, and refusal to disclose their alternative treatments (Tam, 2012). Low patient trust in HCPs can lead to patients withholding medical information, refusing medical recommendations, engaging less in advance care planning or discussing end-of-life matters, and lowered medication adherence (Gregory et al., 2022).
In contrast, patients with high trust in HCP exhibit improved health-related behaviors, outcomes, treatment adherence, satisfaction, and quality of life (Gregory et al., 2022). In addition, patients’ high trust in HCPs facilitates and speeds relief, healing, and cure, contributes to reducing pain and stress, increases faith in medication, positivity towards HCP, likelihood of looking for the same doctor in subsequent visits, likelihood of promoting the provider's reputation, referral tendency within one's social networks, and reduces the possibility of side effects through disclosure (Isangula et al., 2018). Moreover, patients who trust their HCP accept therapeutic recommendations, adhere to HCP recommendations, and are satisfied with HCP recommendations, medical care, and symptom improvement (Brennan et al., 2013).
The results of this study indicated that living arrangements were significantly associated with patient trust in HCPs. As the number of patients’ family members were decreased, there was an increased odds of patients having poor trust in HCP. Therefore, the interaction between individuals within various living contexts at the micro or individual level (family and friends) may be as important as community or society level social capital. Patients living without family, friends, or neighbors are linked to loneliness consequently increasing the odds of trust (Nyqvist et al., 2013). Moreover, a family's living arrangement is an important influencing factor of medical service usage which has a direct impact on health status, quality of life, and mental health (Lin, 2018); thus social support through civic engagement and social participation are key sources of cooperation that advance the collective welfare of society.
The duration of the disease after diagnosis is important. In this study, patients who had <179 days duration of disease after diagnosis were 52% less likely to have poor trust than >366 days duration of disease after diagnosis. This may be explained as an increased length of stay in hospital may contribute to patients’ direct experience of the care process through clinical encounters or as an observer can provide valuable insights into everyday care. Examples include attention to pain control, assistance with bathing, feeding, the environment (cleanliness, noise, and physical safety), and coordination of care between professions or organizations. Furthermore, long hospital stay may not give good comfort for patients and patients may feel that the HCP has not provided good care for them (Doyle et al., 2013). Patients who have been sick for a relatively long period may blame their physicians for failing to solve their problems. Thus, these patients may have less trust in their physicians (Tam, 2012).
This result indicates that presence of comorbid diseases decreased trust of the patient's HCP. Patients who had comorbid diseases may visit hospital frequently and stay for long time inpatient which brings loss of hope that finally leads to no meaningful interactions between patients and patient's HCP in managing the burden of multimorbidity, leading to decreased trust of patient's HCP (Garg et al., 2016).
This study found that impaired physical mobility diminished patient trust in patient's HCPs. This revealed that impaired physical mobility may contribute to low socioeconomic status, comorbidity, lack of motivation (i.e., dependent personality, decreased self-efficacy), weak social networks, and limited social activities (Unsworth et al., 2021). These factors may contribute to the decreased trust in patient's HCP. The current health status self-reporting of patients was statistically significantly associated with decreasing trust. This shows that patients with poor health status had low trust in their HCP.
Strengths and Limitations of the Study
The findings of this study should be viewed in light of some strengths and limitations. In terms of strength, this study is a baseline for further studies to assess patient trust in HCPs. This study is not without limitations. This study was cross-sectional, used a one-time interview which shares all the limitations of cross-sectional studies. Another limitation of this study is that it was a single-center study done on acutely hospitalized patients.
Implications for Practice
Trust is a foundational part of the patient's HCP relationship with important implications for patient consultation and health-related behaviors. Trust is known to improve clinical outcomes. Patients must trust the HCP while sharing their private information and examining their bodies, as this is essential for proper management. Patients might expect their HCP to be compassionate, empathic, competent, honest, dependable, and interested in their good will and look forward to a good outcome of their visit.
Conclusion
In conclusion, patients trust should be repaired by their HCPs. Living arrangement, duration of the disease after diagnosis, comorbid diseases, impaired physical mobility, and current self-reported health status were important factors affecting patient trust in HCP that HCP should give due attention.
Footnotes
Abbreviations
Acknowledgment
We are thankful to Jimma University, Nursing School, and the data collectors. We would also like to thank the study participants for their wholesome efforts for providing information.
Availability of Data and Materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis, and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.