
Abstract
Introduction
During the pandemic, the nursing workforce is experiencing overwhelming workloads that carry a heavy psychological burden. A wide variety of psychological responses to the COVID-19 pandemic have been studied in nurses globally, but many are not studied or understudied in US nurses. Theoretical underpinnings of the current study are based on the disaster component of the Middle-Range Theory of Nurses' Psychological Trauma.
Objective
To explore the associations of psychological responses (life satisfaction, perceived stress, posttraumatic stress disorder [PTSD] symptomatology, attitude toward life, and compassion satisfaction), years of experience, and general health in US nurses during the COVID-19 pandemic using network analysis.
Methods
A cross-sectional study was conducted using an online survey from October to November 2020 in US nurses. Network analysis was used to model the data and analyze the centrality indices of betweenness, closeness, and strength. Data were reported according to the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) checklist.
Results
In 128 nurses, 19.35% of nurses had probable PTSD. Network analysis showed strong significant correlations between life satisfaction and perceived stress (negative), between perceived stress and PTSD symptomatology (positive), and between attitude toward life and compassion satisfaction (positive).
Conclusion
Low life satisfaction, high perceived stress, and low attitude toward life are key inflection points that signal the need for psychological intervention in the US nursing workforce during the continued pandemic. Based on 2021 Tri-Council of Nursing COVID-19 Report and the 2022 International Council of Nurses guideline, healthcare should implement scalable, system-level interventions to reduce psychological burden during the pandemic. The current study suggests targets for such intervention, which may promote a healthier, more effective US nursing workforce.
Introduction/Background
As of April 2022, more than 79 million cases of COVID-19 have been detected and over 970,000 deaths have occurred in the US alone (Centers for Diseases Control and Prevention [CDC], 2022). Hospitals face unprecedented challenges including overcapacity, staff shortages, and infection among healthcare providers (CDC, 2020; Ripp et al., 2020). Because of these major challenges, the nursing workforce is experiencing overwhelming workloads that carry a heavy psychological burden. A meta-analysis reported lack of sufficient resources and being a nurse as risk factors for developing mental health problems during the COVID-19 pandemic (Luo et al., 2020). Preventing maladaptive responses to COVID-19 and reducing psychological sequelae in nurses remain a system-level challenge, given the chronic nature of the pandemic.
The US, the United Kingdom, and China are calling for large-scale, intensive, and long-term interventions to mitigate the psychological burden of COVID-19 in health care providers (National Health Commission of the People's Republic of China, 2020; Türközer & Öngür, 2020; Vostanis & Bell, 2020). Before disseminating psychological interventions to the nursing workforce, however, understanding the research base and theoretical underpinnings of psychological factors related to COVID-19 in nurses is essential. A wide variety of psychological responses to the COVID-19 pandemic have been studied in nurses globally, but many are not studied or are understudied in US nurses.
Review of Literature
In the US, no previous research examined life satisfaction of nurses during the pandemic, but studies found inconsistent levels of life satisfaction (moderate or low) in Turkish nurses (Karabağ Aydın & Fidan, 2022; Teke et al., 2021). In the US, both a national survey and a survey across 30 states showed that one third of nurses had high perceived stress during the pandemic (Prasad et al., 2021; Sinsky et al., 2021). According to the Middle-Range Theory of Nurses' Psychological Trauma, perceptions of stressful experiences are unique to each individual, and nurses cannot avoid such experiences given the nature of their work (Foli, 2021). COVID-19-related experiences of nurses are traumatic, including overwhelming grief and loss when facing patients’ deaths, being torn between personal and family safety and professional duties, and job dissatisfaction and intention to leave the profession (Foli et al., 2021). With these traumatic COVID-19 experiences persisting, allostatic overload can occur leading to increased risk for mental and physical health issues, poor patient care, and burnout (Foli, 2021).
In the US, the severity of PTSD symptomatology varies widely in health care providers including nurses during COVID-19. A study found high severity of PTSD symptomatology in nurses and nursing assistants (Sagherian et al., 2020). However, a national survey reported low severity of PTSD symptomatology in health care providers including nurses (Warren et al., 2021).
Attitude toward life, which reflects the meaning of life, encompasses the elements of ordinary life and connectedness, individual efforts, and the futility of life, and it already has established importance in a previous disaster situation (Uchida et al., 2014). Attitude toward life was introduced and measured in a survey after the Great East Japan Earthquake, which was accompanied by a tsunami and the leaking of radioactive material from the Fukushima nuclear power plant. Reflecting on the disaster, 60% of young Japanese showed changes in attitude toward life including valuing ordinary life and social connectedness (Uchida et al., 2014). Attitude toward life is different from life satisfaction, which focuses on how much a person likes his/her life (Veenhoven, 1996), and attitude toward life is also different from compassion satisfaction, which focuses on the pleasure derived from work (Professional Quality of Life [ProQOL], 2021a). No research examined attitude toward life during the pandemic.
Compassion satisfaction of nurses during the pandemic was not studied in the US. In Spain and Portugal, the majority of nurses had moderate compassion satisfaction (Ruiz–Fernández et al., 2020; Serrão et al., 2022). Finally in US nurses during COVID-19, no studies about general health were found.
The purpose of this study was to explore the associations of psychological responses (life satisfaction, perceived stress, PTSD symptomatology, attitude toward life, and compassion satisfaction), years of experience, and general health in US nurses during the COVID-19 pandemic using network analysis. Compared to correlation and regression analysis, network analysis shows interactions among variables through a network and centrality indices (Epskamp et al., 2018). Network analysis is used in the current study to facilitate the identification of potential psychological inflection points through which to target interventions, which in the future with further study, ultimately, may help to reduce COVID-19-related psychological sequelae in the nursing workforce.
Methods
Design
This study used a cross-sectional survey design following the STROBE checklist (Equator Network, 2021). This design enables researchers to examine relationships among multiple variables at one point in time, which is useful in establishing preliminary evidence for future advanced studies. A Middle-Range Theory of Psychological Trauma (Foli, 2021), the Tri-Council of Nursing COVID-19 Report (2021), and the International Council of Nurses guideline (2022) were used to interpret the findings.
Research Question
The research question is: Using network analysis, what are associations of psychological responses (life satisfaction, perceived stress, PTSD symptomatology, attitude toward life, and compassion satisfaction), years of experience, and general health in US nurses during the pandemic?
Sample
The study used convenience nonprobability sampling. Participants were recruited from an alumni database of 6,000 nursing alumni from a large midwestern university.
Inclusion/Exclusion Criteria
Inclusion criteria were nurses at least 18 years old. An exclusion criterion was lack of Internet access.
Ethical Considerations
The current study complied with the Declaration of Helsinki. Prior approval for using and revising research instruments was obtained from the creators of the research instruments. Individuals participated in the study anonymously and voluntarily. The study was approved by the Institutional Review Board at a large midwestern university (ethics approval number: 275305), and digital consent was obtained from each participant.
Study Instruments
Life satisfaction was measured using the Satisfaction with Life Scale, a five-item scale designed to assess global cognitive judgments of satisfaction with one's life (Diener et al., 1985). It uses a seven-point Likert-type scale (strongly disagree to strongly agree). Higher total scores indicate greater life satisfaction (Measurement Instrument Database for Social Sciences, 2021). Reliability was previously established (Cronbach's α = 0.87; Diener et al., 1985). In the current study, Cronbach's α was 0.79.
Perceived stress was measured using the Perceived Stress Scale, a four-item scale designed to examine the degree to which individuals experience stress in their various life situations (Carnegie Mellon University, 2015). It uses a five-point Likert-type scale (never to very often). Higher total scores indicate greater perceived stress. Reliability was previously established (Cronbach's α = 0.60; Cohen & Williamson, 1988). In the current study, Cronbach's α was 0.84.
PTSD symptomatology was measured using the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders (DSM-5; PCL-5), a 20-item scale designed to assess symptomatology of PTSD (US Department of Veterans Affairs, 2021). It uses a five-point Likert-type scale (not at all to extremely). Higher total scores indicate more severe PTSD symptomatology. The cutoff score for probable PTSD is between 31 and 33 (National Center for PTSD, 2021). In the current study, a cutoff score ≥31 was used. Reliability was previously established (Blevins et al., 2015). In the current study, Cronbach's α was 0.94.
Attitude toward life was measured using the Attitude Toward Life Scale, a 10-item scale designed to assess how individuals’ attitudes toward life are changed after a disaster (Uchida et al., 2011). Attitude toward life scale encompasses three factors: (a) ordinary life and connectedness (example items: I began to feel that normal everyday living is important and makes me happy. I started wanting to place a higher value on the connection with my local community); (b) individual efforts (example item: I started wanting to place a higher value on the sense of fulfillment I get from work or academics); and (c) the futility of life (example item: I began to feel that no matter how hard I try, it's all in vain). Nine items of the original scale were used; one item was conceptually nontranslatable to US culture. The first item measures the degree of change in attitude toward life after the experience of COVID-19 using a five-point Likert-type scale (not changed at all to changed a lot). Only in the case where the response is changed somewhat or changed a lot, is the second part of the instrument completed. It uses a seven-point Likert-type scale (strongly disagree to strongly agree). Higher total scores indicate better attitude toward life. Cronbach's α was previously established and ranged from 0.89 to 0.98 (Uchida et al., 2014). In the current study, Cronbach's α was 0.60.
Compassion satisfaction was measured using the compassion satisfaction subscale of the Professional Quality of Life Scale Version 5. This is a 10-item subscale designed to measure the pleasure individuals derive from being able to do their work well (ProQOL, 2021a). It uses a five-point Likert-type scale (never to very often). Higher total scores indicate greater compassion satisfaction. Total scores that are ≤22 indicate low compassion satisfaction. Total scores that are between 23 and 41 indicate moderate compassion satisfaction. Total scores that are ≥42 indicate high compassion satisfaction (ProQOL, 2021b). Reliability was previously established (Cronbach's α = 0.88; ProQOL, 2021b). In the current study, Cronbach's α was 0.95.
Years of experience was measured by a single question: How long have you been a nurse? General health was measured using the General Health Item from the standard four-item set of Healthy Days core questions (CDC, 2018). A single item used to measure individuals’ general health condition is: Would you say that in general your health is poor, fair, good, very good, or excellent? A higher score indicates better general health (CDC, 2018).
Data Collection Procedure
Pilot testing was conducted to ensure the usability and technical functionality of the online survey before the start of the study. The survey was conducted from October to November, 2020 using Qualtrics. In a recruitment email, the researchers invited participation through a phone or a computer survey link. The survey included 63 questions: 13 about demographic and clinical information and 50 about psychological responses, years of experience, and general health. Volunteers were asked to provide digital informed consent. Participants completed the survey anonymously to reduce response bias. To increase response rate, researchers sent four email reminders.
Statistical Analysis
A partial correlation network was computed using graphical LASSO to investigate the structure and magnitude of associations among life satisfaction, perceived stress, PTSD symptomatology, attitude toward life, compassion satisfaction, years of experience, and general health. Networks are typically displayed (a) using gradations of color and thickness of lines in a graphic and (b) a plot of z-scored centrality indices. In the network graphic, darker and thicker lines show stronger correlations. Additionally, z-scores >0 show a higher centrality in the network.
The graphical LASSO technique is an extension of regression analysis and has the advantage of handling study data with relatively small samples (Finch & Finch, 2016). To run the graphical LASSO algorithm, R packages glasso (Friedman et al., 2008) and qgraph (Epskamp et al., 2012) were used. Undirected edges represent the relationships among the variables in the network, not cause and effect.
To evaluate the centrality indices (betweenness, closeness, strength) of the variables (Epskamp et al., 2018), a bootnet R package was used. The index of betweenness shows the “importance” of each variable in the network (the number of connections each variable has). The index of closeness shows each variable's location in the network. A variable with a higher betweenness and closeness is considered to possess a higher connection in the network. Finally, strength in a network of variables represents the magnitude of the connections between the variables (McNally et al., 2017).
Results
Sample Characteristics
A total of 212 surveys were received. After eliminating participants who answered <90% of the questions, 128 participants were included in data analysis. Participants were predominantly female (90.55%) and White (83.33%), and had a Bachelor's degree (46.03%). Some nurses had contracted COVID-19 themselves (17.32%). Seventy nurses (55.12%) had direct contact, caring for COVID-19 patients. For these nurses, the average days of care were 53.44 with a range of 1 to 245 days. Overall, about one in five nurses had probable PTSD (Table 1). The degree of change in attitude toward life after the experience of COVID-19 is presented in Figure 1 and the level of compassion satisfaction is presented in Figure 2.

The degree of change in attitude toward life after the experience of COVID-19.

The level of compassion satisfaction after the experience of COVID-19.
Demographic and Clinical Variables.a

a Note. Some values may not total 100% due to rounding. PhD = Doctor of Philosophy; COVID-19 = coronavirus disease 2019; PTSD = posttraumatic stress disorder.
Research Question Results
A partial correlation network is presented in Figure 3. The LASSO graphic illustrates significant partial correlations among variables. Analyses indicate strong correlations between life satisfaction and perceived stress (negative), between perceived stress and PTSD symptomatology (positive), and between attitude toward life and compassion satisfaction (positive). In addition, moderate correlations were identified between attitude toward life and life satisfaction (positive) as well as between compassion satisfaction and perceived stress (negative). Other moderate correlations were between general health and life satisfaction (positive) and between general health and perceived stress (negative). Smaller correlations were found between years of experience and perceived stress (negative), between years of experience and PTSD symptomatology (negative), between years of experience and compassion satisfaction (positive), and between general health and PTSD symptomatology (negative). Overall, findings with strong correlations stood out as clinically relevant.
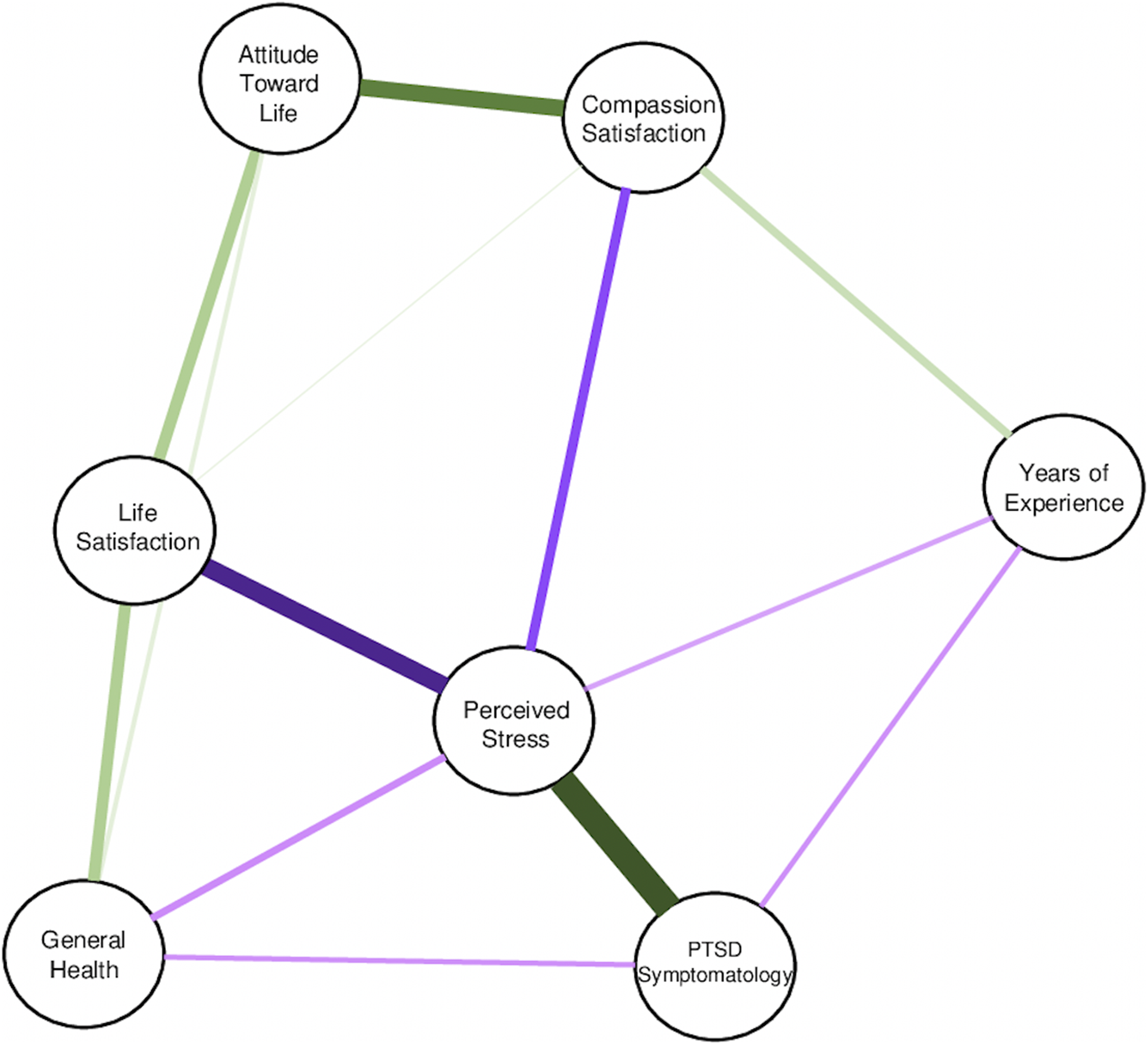
The LASSO graphic for regularized partial correlations among life satisfaction, perceived stress, PTSD symptomatology, attitude toward life, compassion satisfaction, years of experience, and general health. Green lines illustrate positive correlations. Purple lines illustrate negative correlations. Darker and thicker lines show stronger correlations.
Z-scored centrality indices (betweenness, closeness, strength) are presented in Figure 4. Life satisfaction, perceived stress, and PTSD symptomatology had a z-score >0 for each index, demonstrating higher centrality than other variables. Specifically, life satisfaction had the highest betweenness connection with other variables; perceived stress had the closest and strongest connection with other variables in the network. PTSD symptomatology had considerable betweenness (importance; z-score = 0.4) and closeness (z-score = 0.3), and a strength >0 (z-score = 0.2). In contrast, years of experience and general health, with a z-score <0, showed the lowest centrality. Overall, based on betweenness, life satisfaction, perceived stress, and PTSD symptomatology stood out as “important” variables. The betweenness of attitude toward life was only slightly below the zero.

The Z-scored centrality indices in the network. The centrality indices are betweenness, closeness, and strength. The variables of interest are listed on the left. Z-scores >0 show a higher centrality in the network.
Discussion
In the current study, 19.35% nurses had probable PTSD. Whether this percentage is consistent with previous COVID-19-related research in the US is difficult to tell. In one study across 15 states, 23% of nurses showed a high risk for developing PTSD during the pandemic (Rodriguez et al., 2021). In another study, 55.38% of nurses and nursing assistants had probable PTSD during the pandemic (Sagherian et al., 2020). Furthermore, in a national survey, 4.6% of health care providers including nurses showed pandemic-associated probable PTSD (Warren et al., 2021). The difference in percentages might be explained by the use of various PTSD scales, cut-off scores, and scoring algorithms as well as combined groups of health care workers.
Under the influence of COVID-19, more than half of US nurses studied experienced somewhat or a lot of change in attitude toward life, signaling a major life shift. Given this is the first time that attitude toward life has been examined in COVID-19 research, the degree of attitude toward life change needs to be confirmed in future studies. One important aspect of attitude toward life is futility of life. High futility of life is reflected by participants indicating that their efforts are useless and their efforts do not bring any meaning or value to their lives (Uchida et al., 2014). It seems therefore that nursing managers and counselors would want to be aware of and interested in monitoring increasing feelings of futility of life.
Three key inflection points for maladaptive responses in US nurses during the pandemic were identified primarily based on the presence of strong relationships and also on the indices of centrality using network analysis. Regarding the first inflection point, a strong negative relationship between life satisfaction and perceived stress in nurses during COVID-19 was found in the current study. This relationship was not directly examined in previous research. However, a study reported strong family functioning and high resilience (indicators of life satisfaction) as protective factors for perceived stress in US nurses during COVID-19 (Kim et al., 2021). Furthermore in the current study, life satisfaction also served as an “important” variable based on z-scored centrality indices. Therefore, life satisfaction is a potential inflection point for intervention to reduce perceived stress in nurses during the pandemic.
Regarding the second inflection point, the strongest positive association was found between perceived stress and PTSD symptomatology. The relationship was also found in frontline ICU nurses in China during the pandemic (Leng et al., 2021), a meta-analysis, and a literature review before the pandemic (Ozer et al., 2003; Rajkumar, 2020). Additionally, according to z-scored centrality indices, perceived stress was an “important” variable in the network. Therefore, perceived stress is a potential inflection point for intervention to mitigate PTSD symptomatology in nurses during the pandemic. Furthermore, in the network analysis, three psychological responses predominated. Strong correlations between life satisfaction and perceived stress, and between perceived stress and PTSD symptomatology highlighted that life satisfaction also serves as a potential inflection point for intervention to mitigate PTSD symptomatology in nurses during COVID-19.
Regarding the third inflection point, a strong positive relationship was found between attitude toward life and compassion satisfaction. Because of the strong relationship, attitude toward life is a potential inflection point for intervention to improve compassion satisfaction.
Few studies in US nurses were found in the literature on the significant low and moderate relationships reported in the current study. Findings from Kim et al. (2021) were in agreement with the finding in the current study that years of experience was negatively related to perceived stress. In contrast to the finding of a negative relationship between years of experience and PTSD symptomatology in the current study, Schierberl Scherr et al. (2021) found no significant relationship. This might be due to the use of different PTSD instruments (Schierberl Scherr et al., 2021).
Strengths and Limitations
The major strength of this study was the use of network analysis, which has the advantage of providing a model of the data as well as centrality indices, illustrating the structure and magnitude of associations. The current study has some limitations. First, the study utilized a relatively small sample of nurses; larger, more diverse studies are warranted. Second, this cross-sectional design could not capture changes in psychological responses over time. Future research, using a multiwave or longitudinal approach would allow for the examination of how COVID-19 chronicity influences these relationships. Third, because health care systems vary widely across countries, generalizing findings to countries outside of the US should be done with caution. Finally, all psychological outcomes were self-reported, which could result in overestimation or underestimation of psychological burden.
Implications for Practice
The latest national and international nursing guidelines suggest nurses’ transition to recovering from the burdens of working during the COVID-19 crisis (International Council of Nurses, 2022; Tri-Council for Nursing, 2021). Nursing guidelines are focused on sustaining the psychological well-being of nurses and retaining them in practice (International Council of Nurses, 2022; Tri-Council for Nursing, 2021). Given that the pandemic has persisted for over two years, countries have released their own policy guidelines, emphasizing the need to move to system-level, long-term COVID-19-related counseling interventions (National Health Commission of the People's Republic of China, 2020; Tri-Council for Nursing, 2021). Although the type, cost, and feasibility of these future therapies have not been determined, the findings of the current study support a move to long-term therapy. We found that the majority of participants had experienced a major shift in their lives, a profound change in attitude toward life, and over 19% had probable PTSD. Long-term therapies must focus beyond coping with COVID-19-related events in the work setting and include, more generally, COVID-19-related challenges in life and struggles with everyday living as well.
We found that life satisfaction was prominent in our network analysis and was strongly related to perceived stress, suggesting that low life satisfaction should be targeted in counseling interventions. Our network model supports that if long-term counseling could break the chain between low life satisfaction and high perceived stress and then high PTSD symptomatology, then it would mitigate maladaptive responses in practicing nurses.
The Tri-Council of Nursing COVID-19 Report (2021) stresses the need to monitor psychological outcomes and determine benchmarks to show when psychological interventions are successful in the nursing workforce. This report emphasizes that, from a policy perspective, psychological health should be taken more seriously; it should be taken at least as seriously as physical health during the pandemic. In our network model, psychological variables were more important than general health.
In the qualitative study, nurses reported the intention to leave their job or profession due to the psychological trauma related to COVID-19 (Foli et al., 2021).
The key goal of the International Council of Nurses guideline (2022) is to sustain and retain nursing workforce during the prolonged pandemic. To achieve this goal, nursing leadership should provide intervention programs that improve psychological well-being of nurses, such as that enhancing compassion satisfaction through improving nurses’ attitude toward life.
Conclusions
We successfully used network analysis to identify psychological variables that nurse administrators and nurse practitioners might target for long-term therapy, given that COVID-19 is persisting in the US. In other words, awareness of low life satisfaction, high perceived stress, and low attitude toward life may serve as primary prevention targets to reduce the mental health burden of nurses. Specifically, improving life satisfaction through therapy might reduce perceived stress and in turn reduce PTSD symptomatology. In addition, enhancing attitude toward life is associated with augmenting compassion satisfaction, a significant factor in quality patient care. According to the recommendations from recent guidelines about recovering from COVID-19 (International Council of Nurses, 2022; Tri-Council for Nursing, 2021), implementing interventions for psychological health must be a high priority. Psychological well-being must be enhanced to the extent necessary to sustain and retain nurses during the pandemic.
Footnotes
Acknowledgments
The authors thank Keri Jupka who assisted to conduct the study and all nurses who spent their time and effort to participate in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The current study complied with the Helsinki Declaration. Prior approval of using and revising research instruments was obtained from creators of research instruments. Individuals participated in the study anonymously and voluntarily. The study was approved by the Institutional Review Board at University of Missouri – St. Louis (ethics approval number: 275305) and digital consent was obtained from each participant.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Anne F. Fish received a grant from UMSL Global at the University of Missouri – St. Louis for publication costs.