
Abstract
Introduction
Paying attention to stigma among caregivers to provide proper care for patients is necessary, and promoting awareness (about mental illness and mental health) to taking care of the caregivers’ health, is crucial.
Objective
This study aimed to investigate the effect of psycho-education on the affiliate stigma in family caregivers of people with bipolar disorder.
Method
This study is a quasi-experimental research with an experimental and control groups. 64 family caregivers of people with bipolar disorder participated in this study (32 in each group). Data was collected using the demographic questionnaire and Affiliate Stigma Scale before and after intervention (with 4 weeks gap). The experimental group received a psycho-education program for four weeks. The control group carried on their normal routine lifestyle.
Results
The mean scores of the affiliate stigma of both control and experimental groups before the intervention did not show a statistically significant difference (P = .36), however after the intervention the results were statistically significant and increased in the experimental group (P < .001).
Conclusion
According to the findings of this study psycho-education is an effective intervention that can reduce the affiliate stigma among family caregivers of people with bipolar disorder and it can be considered as one of the de-stigmatization strategies for them.
Introduction
Bipolar disorder (BMD) is one of the most common psychiatric disorders (Gania et al., 2019; Michalak et al., 2011). The prevalence of BMD in the general population is three percent and it is the sixth leading cause of disability worldwide (Gania et al., 2019). Family members as the close relatives of the patient, play an important role in support of them. These families often experience negative emotions such as depression and other health problems due to an increased caregiving burden (Fitriani & Suryadi, 2019). As well as, psychosocial stressors, especially during the relapse-recovery period of this disorder, can affect the burden they experience (Miklowitz, 2007).
Generally, families’ awareness/knowledge of mental illness is insufficient. For these families, many of the support resources are not available in time of need, which may be due to the stigma relating to mental illness (Shamsaei et al., 2015). Caring for patients puts a lot of burden on families, mainly in terms of psychosocial and stigma. These burdens are one of the most challenging situations that families may experience (Girma et al., 2014).
Review of Literature
Based on Goffman's conceptualization, stigma is an attribute that leads to distress and psychological discomfort in a person who is affected by it. From a social point of view, stigma may affect the attitude of others toward these people (Stuart, 2016). The existence of stigma in the society context, either directly or indirectly, can affect individuals (especially those who live with mentally ill people) (Ahmedani, 2011). Affiliate stigma occurs when a person cognitively and emotionally accepts the common negative assumptions and stereotypes in society about mental illness, and believes in them. By accepting and believing in the stigma, the person's behavior will also be affected (Drapalski et al., 2013). Affiliate stigma in caregivers of people with mental illness develops when they perceive and internalize public stigma toward themselves. Caregivers are affected with affiliate stigma in terms of cognitive component (accept public stigma toward themselves); affective component (feel negative emotions stemming from affiliated stigma); and behavioral component (withdraw from social relations or alienate themselves from stigmatized family members; Chang et al., 2020).
Studies show that there is a direct relationship between the affiliate stigma and increased caregiving burden (Mak & Cheung, 2011), signs and symptoms of depression, feeling of
According to the World Health Organization, there are at least 450 million people with mental disorders, and it is estimated that 30% of these patients can be appropriately treated with effective interventions, including de-stigmatization of their caregivers and return to society (Tawiah et al., 2015). Therefore, one of the ways of improving the well-being of people with bipolar disorder in line with standard treatment is to increase the awareness and knowledge of their caregivers about the disease (Sajedianfard et al., 2019). With the advancement of nursing science, attentions have shifted to the families as a goal for caregiving, because they are an essential part in the caregiving process (Oliveira Pda et al., 2011). Therefore, appropriate interventions for caregivers will play an important role for people with mental disorders (Chang et al., 2017). In this regard, psycho-education can be useful in increasing the level of knowledge as well as in improving process of de-stigmatization within the family environment (Girma et al., 2014).
Psycho-education provides appropriate knowledge to family caregivers and enables them to deal with mental disorders effectively by learning appropriate skills. Therefore, psycho-education can reduce the caring burden by improving/increasing the level of knowledge (Fitriani & Suryadi, 2019) and necessary skills (communication and problem-solving) of family caregivers (Girma et al., 2014).
Since maintaining the well-being of family caregivers is necessary to provide proper care to patients, thus promoting their knowledge and awareness (about mental illness, coping skills, how to maintain their health and how to provide proper care) is crucial to keeping their mental health in a reasonable level. It is possible that psycho-education as an effective intervention can help the families to manage the crisis that may be caused by a family member's illness. Thus, this study was aimed to investigate the effect of psycho-education on the affiliate stigma in family caregivers of people with bipolar disorder, in Sanandaj, Iran.
Methods
Design
The present study is a quasi-experimental research with control and experimental groups. This study was conducted in the Ghods Psychiatric Hospital, in 2019–2020 in Sanandaj, Iran. In coordination with the officials of Ghods Psychiatric Hospital, the sampling procedure was performed on all wards of the hospital and the outpatient clinic. Those caregivers who were eligible and willing to enter the study were selected. After the explanation of the study objective, ensuring the confidentiality of personal information and receiving their informed consent, the questionnaires were provided to them. Sampling was performed first for the control group and then for the experimental group (in order to prevent from any possible bias). The sampling method in the experimental group was the same as that of the control group. It should be mentioned that the pre-test and post-test were conducted for the control group with a time interval of four weeks.
After recruitment of subjects of the control group as well as the experimental group, psycho-education was provided to the experimental group (during the hospitalization of their patients). It should be noted that during the psycho-education, the control and experimental groups did not have any contact. The psycho-education for the experimental group was performed by psychiatric/mental health nurse practitioner during four weeks, one session per week for 60 to 90 min, in the class that was prepared in advance for providing training (in the educational unit of the hospital) through group discussion. The headings of the psycho-education were provided to the caregivers at the beginning of each session, and before any explanation they were asked to share their attitudes and experiences about it. This intervention, in terms of expressing the concept of stigma, (other provided educational concepts have been in line with this concept) was different from other psycho-educations, which most of them only express the concept of illness, treatment and patient care. Table 1 provides the titles of educational content. Post-test immediately after finishing the psycho-education was performed.
Psycho-education Program Provided for Four Weeks.

Research Question
Does psycho-education reduce the level of affiliated stigma among family caregivers of people with bipolar disorder?”
Sample
The simple random sampling method was performed and the sample size was measured according to the study of Shamsaei et al. (2018), with the reliability level of 95% and statistical power of 80% and taking into account the 10% drop-out in the samples size, by using the following equation, and 32 people (the caregivers of people with bipolar disorder) was considered in each group (total sample size was 64).
Inclusion/Exclusion Criteria
The inclusion criteria included, 18 to 65 years of age, spending the most caregiving time for the person with bipolar disorder, and lack of physical disability. It should be noted that for each hospitalized patient, only one family member was allowed to enter the study. If the caregivers did not participate in one of the training sessions, or unexpected events occur, such as the death of a relative or hospitalization of a caregiver, they were excluded from the study.
Instruments
The demographic questionnaire
This questionnaire
Affiliate stigma scale
This scale, designed and developed by Shamsaei et al. in 2016, consists of 30 items on 5-point Likert scale (always (4), most of the time (3), sometimes (2), rarely (1), and never (0)). The score ranges from 0 to 120. A score between 0 and 30 indicates no stigma, (30–60) indicates mild stigma, (60–90) indicates moderate stigma, and (90–120) indicates high stigma. Shamsaei et al. obtained the validity of the Affiliate Stigma Scale through content validity and Cronbach's alpha coefficient of 0.94 (Shamsaei et al., 2018).
In this study the value of the Cronbach's alpha coefficient used to test the reliability of the Affiliate Stigma Scale was .85 that indicates the favorable reliability for this scale.
Ethical Considerations
The control group carried on their normal routine lifestyle, but in order to observe the ethical standards, after completing the training of the experimental group, the educational content was presented in the form of a small booklet and pamphlet for the control group.
Statistical Analysis
Data were analyzed using SPSS-22. The descriptive analysis included frequency distribution, mean, and standard deviation. Independent and paired t and analysis of variance were also used. The significance level was set at α = .05.
Results
Sample Characteristics
According to Table 2, most of the caregivers were women (54.7%), and married (73.4%). The mean age of the caregivers was 41.48 ± 10.16 years, most of them were spouses of the clients (29.7%), self-employed (28.1%), and had moderate economic status (64.1%). In terms of education most of the caregivers had diploma degree (31.3%), and the majority of them did not have a family history of the disease (62.5%). Mean duration of the disease was 4.61± 2.97 years with the mean of 4.67± 3.23 previous hospitalizations.
Demographic Characteristics of the Samples.
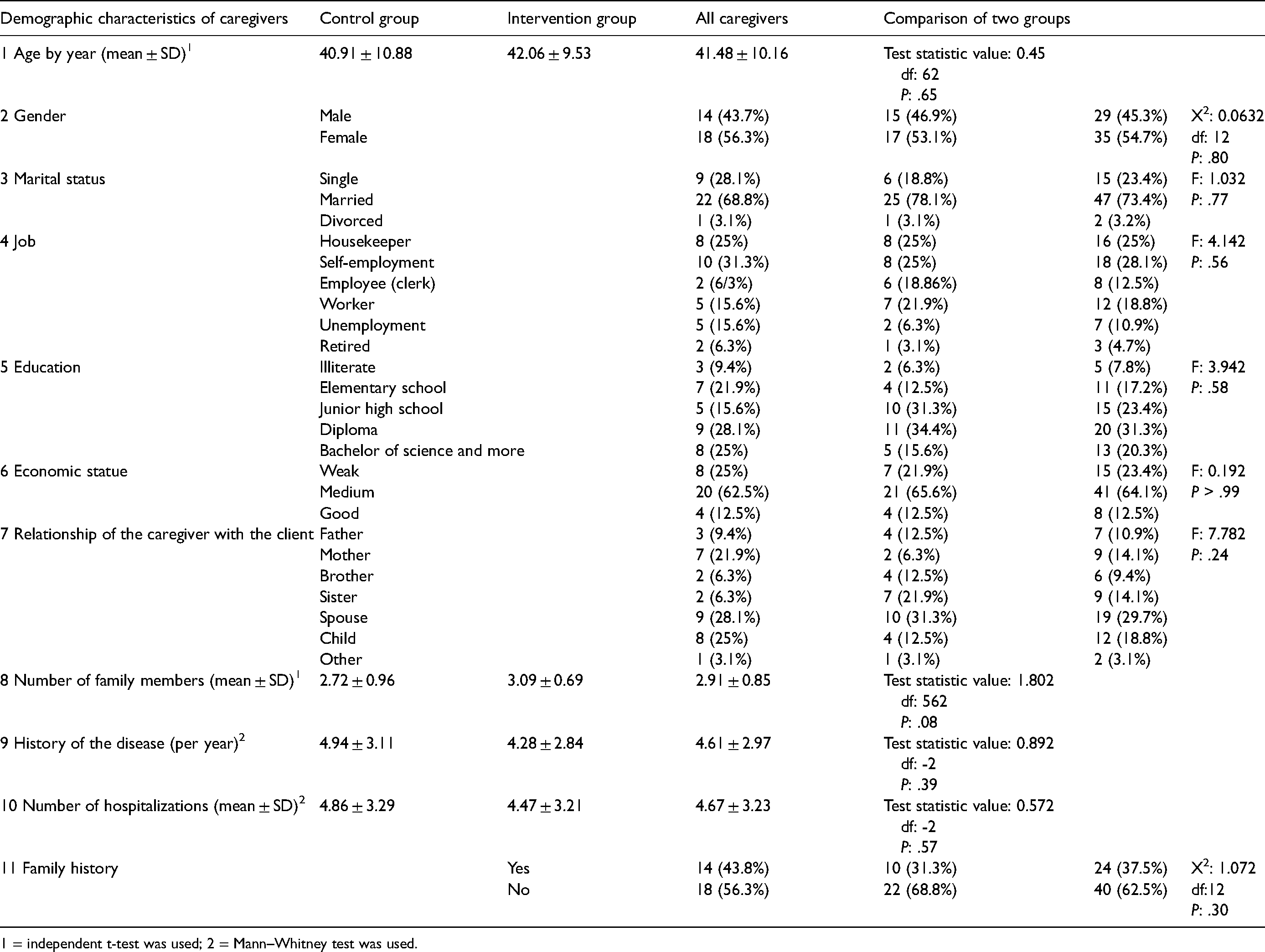
1 = independent t-test was used; 2 = Mann–Whitney test was used.
Research Question Results
Table 3 showed the mean scores of affiliate stigma in control and experimental groups. These scores were 73 ± 14.72 and 69.63± 14.66 for control and experimental groups respectively. Therefore no significant difference was found between the two groups at baseline (P = .36), and all of them had moderate level of affiliate stigma. Although in the control group the mean score of the post-test of the affiliate stigma was 74± 14.21, which was not significantly different from pre-test (P = .17), but after the intervention the post-test results in the experimental group (after the implementation of the psycho-education) changed, and the mean score of the affiliate stigma reached 35.06 ± 8.31, which showed a statistically significant difference (P < .001), and the level of affiliate stigma was decreased (Table 4).
Comparison of Affiliate Stigma Before and After the Intervention in the Both Control and Experimental Groups.

Comparison of the Mean Affiliate Stigma Scores of the Pre-test and Post-test in the Both Control and Experimental Groups.

Discussion
Lack of knowledge about mental illness is one of the main components of the stigma and is also associated with stigmatizing attitudes (Koschorke et al., 2014). This study provides a brief opportunity to examine how psycho-education can affect the level of knowledge and awareness of family caregivers of people with bipolar disorder. The results of the present study showed a moderate level of affiliate stigma at the baseline and psycho-education can decrease stigma's level in experimental group which indicates the positive effect of psycho-education by providing knowledge to the caregivers.
Families often face many stressors due to lack of knowledge and skills in their caregiving role, which the most important of them is stigma (Vaghee et al., 2015). As the literature indicates, stigma is one of the most important issues and challenges that family caregivers of people with mental disorders face (Ae-Ngibise et al., 2015; Pittman et al., 2010; Steel et al., 2014; Yin et al., 2014), and also is one of the main reasons of avoiding asking for help by patients and their caregivers (Farzand & Baysen, 2018).
Some researchers stated that the lack of knowledge and awareness about mental illness as well as the stigma imposed by the society on caregivers leads to a negative attitude toward mental illness and eventually ignoring the ill member (Elkhalek Ahmed & Hady Ghaith, 2018; Ostman & Kjellin, 2002; Shah-Veysi et al., 2007; Yin et al., 2014). Psycho-education can reduce the negative attitude of family caregivers by providing useful and practical information about mental illness and its treatment. In fact, psycho-education leads to the acceptance of the ill member in the family environment and improves the inner feeling of the families toward the patient and themselves (Rahmani et al., 2016; Vaghee et al., 2015).
The findings of previous studies showed that the mean stigma score, after the psycho-education for caregivers of people with psychiatric disorders had a significant reduction (Cuhadar & Cam, 2014; Shamsaei et al., 2018; Uchino et al., 2012; Vaghee et al., 2015), and the other studies indicated that patient inattention rate that imposed by the caregivers was significantly reduced after the intervention (Cook et al., 2014; Cuhadar & Cam, 2014), and the amount of social interactions among the caregivers was increased (Cook et al., 2014; Cuhadar & Cam, 2014; Uchino et al., 2012). Shamsaei et al. in their study showed that, after the psycho-education and increasing the level of awareness and knowledge, the parents did not blame themselves for their child's mental illness (Shamsaei et al., 2018), and the study of Rahmani et al. showed that after the intervention (psycho-education), the positive attitude of family caregivers toward the people with bipolar disorder were significantly increased (Rahmani et al., 2016), which indicates the positive effect of providing knowledge. Bernhard et al. (2006) and Yang et al. (2014) also noted that the psycho-education, which improved the level of knowledge and attitudes of caregivers about mental illness led to a positive attitude in caregivers toward the ill person and their disorders and has a significant impact on the recovery of people with psychiatric disorders (Bernhard et al., 2006; Yang et al., 2014). In the present study the effectiveness of psycho-education on reduction of the affiliate stigma has been confirmed, and it is aligning with the results of the above studies.
Strengths and Limitation
One of the strong points of this study is the inclusion of the concept of stigma in the educational content, which other concepts (life skills and coping strategies) were explained in line with it. However, there were some limitations in the implementation of this study that should be noted. First of all, the present study was a short duration of psycho-education and it seems that the long-term and continues training is more effective in improving the quality of the intervention; therefore the inclusion of psycho-education in community-based care, can be useful. The sample size of this study was small and since this study was conducted in a limited area, the results of this study may not be generalizable to a larger population; so, it is suggested that similar interventions in future studies be performed on larger populations. Another limitation was the lack of follow-up investigation about the effectiveness of psycho-education after performing it for families. Considering that only the families of hospitalized patients participated in this study, as a suggestion it is better to include the families of inpatients and outpatients in the future studies and then compare the results. Despite the above limitations, the findings of the present study provided significant empirical evidence on the effectiveness of psycho-education on the reduction of the affiliate stigma in the family caregivers of clients with bipolar disorder.
Implications for Practice
We demonstrated that the caregivers of people with bipolar disorder had a high level of affiliate stigma that put their health at risk. Therefore, psycho-education as a reliable way can be a useful educational program to promote their awareness. Future studies should have more emphasis on promoting and maintenance of mental health of the caregivers and patients with the use of complementary methods alongside with psycho-education.
Conclusion
The present study showed that stigma is one of the issues of the family caregivers of clients with bipolar disorder. Due to the key role of the caregivers in the caregiving process, the follow-up, and the constant treatment of patients, it should be noted that the lack of adequate knowledge and awareness about the concept of stigma may reduce the quality of care provided by the caregivers and endanger their physical and mental health. Therefore, continuous efforts to reduce stigma among the family caregivers seems to be vital and necessary.
Based on the findings of the present study, it can be said that one of the de-stigmatization strategies among the caregivers of people with bipolar disorder is the implementation of the psycho-education; therefore, based on the results obtained, the main hypothesis of this research which suggests that psycho-education can decrease the affiliate stigma of family caregivers of people with bipolar disorder, is confirmed. It seems that more attention to this educational intervention can be useful in the process of treating patients and supporting their families.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
This study was approved by the research ethics committee of Kurdistan University of Medical Science (approval no.: IR.MUK.REC.1398.15).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Kurdistan University Of Medical Sciences (grant number IR.MUK.REC 1398.151).