
Abstract
Introduction
As simulated patients in simulation-based learning, nursing students can contribute to a better understanding of the patient perspective in clinical practice.
Objective
The aim was to explore final-year nursing students’ experiences in roleplaying as patients in a student-led simulation of difficult conversations as a form of preparing for practice in mental healthcare and homecare nursing.
Methods
The study was conducted using a qualitative research design. After the student-led simulation, four of the students participated in multistage focus group interviews over a period of six months: the first interview was immediately after simulation and the second was after clinical practice.
Findings
One main theme was identified before clinical practice: “simulating the patient contributes to preparation for difficult conversations in practice.” Two main themes were identified after the students’ clinical practice: “simulation of both the nurse and patient lays the foundation for communicating with patients” and “the value of silence.”
Conclusion
The findings indicate that simulation training and role exchange when students roleplay both as the patient and nurse contribute to a greater understanding of the patient perspective, and students benefit from this when communicating with patients in clinical practice.
Keywords
Introduction
Nursing students must learn to provide caring and professionally sound nursing based on updated knowledge, and respect for the patient’s autonomy and participation. During their education, students must acquire competencies in a relationship, communication skills, and guidance skills to be able to understand and interact with patients and their relatives. By learning therapeutic communication, understood as “a face-to-face interaction that focuses on improving the emotional and physical welfare of the patient,” the students become more confident in communication (Blake & Blake, 2019). To obtain these skills, nursing students’ role as patients in simulation-based learning (SBL) can contribute to forming a better understanding of the patient perspective when students do their clinical practice.
Review of Literature
SBL is a student-active standardized method in which students simulate the role of nurses to achieve the given learning objectives, which are led by facilitators (INACSL, 2016; Jeffries, 2021). The patient can be either a simulator or can be played by a simulated patient (SP), a term often used interchangeably with the term standardized patient (Hall, 2017; MacLean et al., 2017). An SP is preferred over a simulator for topics such as communication, and can be played by actors, drama students, former patients, teachers, or fellow students (Coleman & McLaughlin, 2019; Mackey et al., 2014; Söderberg et al., 2017). The facilitators can be either teachers or professional instructors. SBL can also be student-led, which here is understood as peer-to-peer learning where students guide and facilitate each other (Schunk, 2012; Svellingen et al., 2021). The three phases of simulation are as follows: (1) briefing; (2) simulation; and (3) debriefing (INACSL, 2016; Jeffries, 2021).
Moreover, previous studies have shown that nursing students are anxious about entering therapeutic communication with patients, especially when it comes to challenging and difficult conversations with mental patients (Blake & Blake, 2019; Hall, 2017; Vandyk et al., 2018). When carried out before such practice, SBL provides students with a valuable learning experience which can reduce students’ anxiety (Coleman & McLaughlin, 2019; Hall, 2017; Svellingen et al., 2021; Vandyk et al., 2018).
An SP in simulation training provides valuable feedback on the patient's perspective and contributes to the achievement of learning goals (Johnson et al., 2020; MacLean et al., 2017; Söderberg et al., 2017; Vandyk et al., 2018). Dalwood et al. (2020) found no significant differences between students who simulated with peers as patients and students who simulated with trained persons as patients. Playing the role of a patient in simulation positively impacted learning communication and helped develop empathy.
Furthermore, in a study where junior students simulated basic skills with senior students as patients, Mackey et al. (2014) found that students playing the role of patient obtained new perspectives being patient and became aware of their observation skills. Senior students reported increased reflection and that their experiences as an SP had personal and professional impacts. However, they called for research on the impact of experiences the patient role has on nursing students’ clinical practice.
Position Exchange Theory presented by Gillespie and Martin (2014) deals with how in interaction, people develop and change by moving within physical, social, and institutional spaces. This theory is explained in more detail by the concepts of “play,” “game,” and “education,” where the latter two are central to the present research. The participants change positions, thereby gaining an increased understanding of each other's positions. Understanding strengthens the ability to anticipate the other's actions. Here, it is possible to cultivate the other's perspective, gradually gaining a bodily understanding of other social positions. Eventually, one will play the game about being a generalized other. The same happens in education when using different forms of peer student learning such as student-led simulation. Students learn by taking other people's perspectives.
Consequently, the aim of the current study is to explore nursing students’ experiences when roleplaying patients in a student-led simulation of difficult communication with suicidal patients, patients with dementia, depression, or lack of motivation. Additionally, to explore whether students’ experiences as SPs could support understanding the patient's perspective during clinical practice in mental health/homecare nursing.
Methods
Design
The current qualitative research study used a hermeneutics approach in interpreting the findings (Creswell & Creswell, 2018). Data were collected through multistage focus group interviews (Hummelvoll, 2008, 2010) unlike focus groups that are normally interviewed once (Krueger & Casey, 2015; Malterud, 2012, 2017) after a student-led simulation. The purpose of choosing multistage focus group interviews was to explore together with the same group of nursing students their experiences over time. Therefore, the focus group met twice at six-month intervals. According to Hummelvoll (2008), additional meetings contribute both to exploring experiences and counter-experiences and to saturation.
Context
A Bachelor of Nursing program at a Norwegian university college uses SBL throughout the students’ education following the Simulation in Nursing Education (Jeffries, 2021) and INACSL Standards of Best Practice (2016) as a framework. Thus, simulation was a well-known pedagogical method for the class of 70 final-year students. A student-led simulation was carried out at school in advance of clinical practice in homecare nursing and mental healthcare.
The class was first divided into two, and each part was divided into eight groups of four to five students. Second, all groups attended a workshop in which they prepared content for shared resources concerning motivational interviews, active listening, nonverbal communication, paraphrasing, validation, open-ended questions, mirroring, and cognitive impairment (all subjects related to therapeutic communication). At the end of the workshop, the groups presented their work to each other. Third, the student-led simulation was planned under the guidance of experienced teachers. One day was set aside to plan and prepare the patient scenario based on a given template and the chosen learning objectives for the simulation training (Jeffries, 2021). The groups were given various relevant issues for the simulation, such as smoking habits with chronic obstructive pulmonary disease, depression in adolescents, suicide risk, a spiritual conversation with a patient afraid of dying and a patient suffering from dementia. To ensure professional quality, the patient scenarios were reviewed and approved by the supervisor. Furthermore, the groups prepared a role card for the patient and rehearsed in advance.
Example of a Patient Scenario From the Simulation
Has knowledge of how illness and health affect the population. Knows how to facilitate actions that strengthen the individual and environment’s resources. Applies different communication techniques. Shows empathy and understanding for people in different life situations.
It was set aside for two simulation days (Table 1). The 16 groups alternated between facilitating simulation one day and simulating the nurse's role in different scenarios the opposite day.
Organizing Student-led Simulation (Switching Groups the Other day).
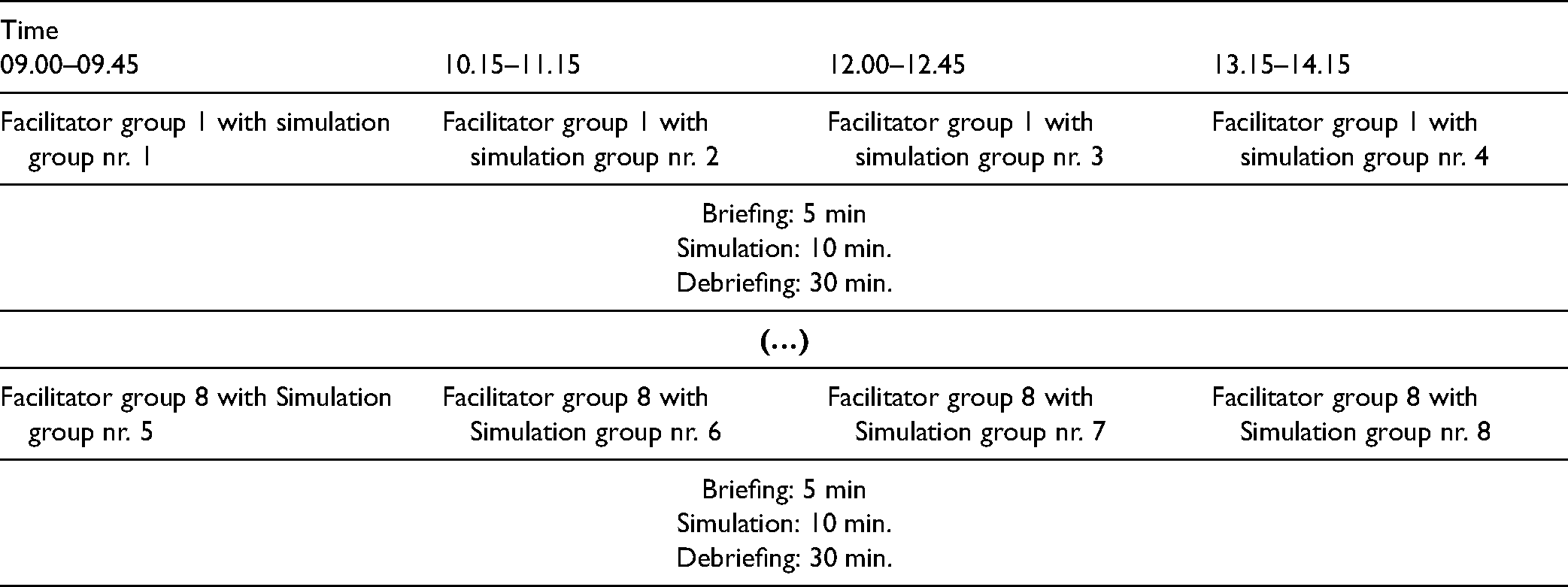
Furthermore, the students in the facilitator group switched roles, hence either being the facilitator once and the patient the next time or vice versa. The students in the opposite group took similar turns playing the nurse. When simulating, the student acting as the nurse had the opportunity to take a timeout and discuss what happened with their group. The same patient scenario was played four times.
The debriefing was facilitated by a student from the group who led the simulation following a debriefing template. The SP actively participated in the reflection, while the other group members were observers. All members of the opposite group (the nurse group) participated in the reflection.
To ensure the students felt secure when simulating the roles, the supervisors followed the groups when planning, simulating, and debriefing and could intervene if necessary. All the supervisors were skilled and had extensive experience both as nurses and teachers. The students knew they were not performing as individuals but as representatives of their group. The possibility of taking a timeout for discussion with one's group was one action for making the students roleplaying the nurse feel more comfortable. Both the rehearsal before simulation and active participation during the debriefing were actions to make the students in the role of patient more comfortable in case they felt uncomfortable. They were all encouraged to contact their supervisor afterward if something was perceived as emotionally difficult.
Participants and Data Collection
After the simulation, all 70 students received oral and written information about the study with a request to participate in a multistage focus group that would have two interview sessions: the first interview the week after a simulation, which occurred shortly before starting a clinical practice, and the second interview, which occurred after clinical practice.
The invitation to participate was given to the whole class by the responsible teacher after the students’ simulation training. Five students from different simulation groups, all women aged 21–25, gave written consent to participate. One focus group was established. One participant was ill for the first interview and, hence, was excluded.
Because of time constraints (only a one-week opening after simulation and before they started their clinical practice), no further attempt was made to include more participants in several focus groups.
One female researcher (AS), external to the students, led both interviews at the students’ university, conducting an in-depth exploration focusing on student involvement in the simulation. In the first interview, the focus group was asked to reflect on their experiences concerning planning the simulation, simulating the patient scenario, the debriefing session, learning outcomes, the significance of a present teacher, and the simulation's expected significance for clinical practice. In the last interview, the focus group was asked to reflect on the same in retrospect, now with the added knowledge of their clinical experience. Another female researcher (KR) was the moderator. Both interviews lasted approximately 60 min. The interviews were taped and transcribed verbatim. The results of the first interview served as a background for the second interview.
Data Analysis
Qualitative content analysis was performed (Graneheim & Lundman, 2004). All three researchers contributed to the analysis process. The interviews were read thoroughly several times. Meaning units were identified, condensed, abstracted, and then labeled with a code. The codes were compared to find similarities and differences and sorted into categories, described as the manifest content. Finally, after a thorough process of reflection and discussion, the researchers agreed upon the themes and the latent content. Examples of qualitative content analysis are given in Table 2.
Example of Qualitative Content Analysis (Graneheim & Lundman, 2004).

Ethical Considerations
Ethical approval was obtained from the Norwegian Centre for Research Data. Informed written consent was obtained. Anonymity was maintained throughout the research process. The audio recordings were kept confidential until deleted after transcription. The participants were unknown to the researcher leading the interviews. Because of her SBL competency, the moderator had been a supervisor for some groups when simulating, but she did not previously have a central lecturer role in the class.
Results
The data analysis of the multistage focus group interviews produced three key themes: (1) Simulating the patient contributes to preparing for difficult conversations in practice. (2) Simulation of both the nurse and patient lays the foundation for communicating with real patients. (3) The value of silence. Themes and categories are given in Table 3.
Themes and Categories from Content Analysis of Multistage Focus Group Interviews About Nursing Students Experiences from Roleplaying Patients in (SBL).
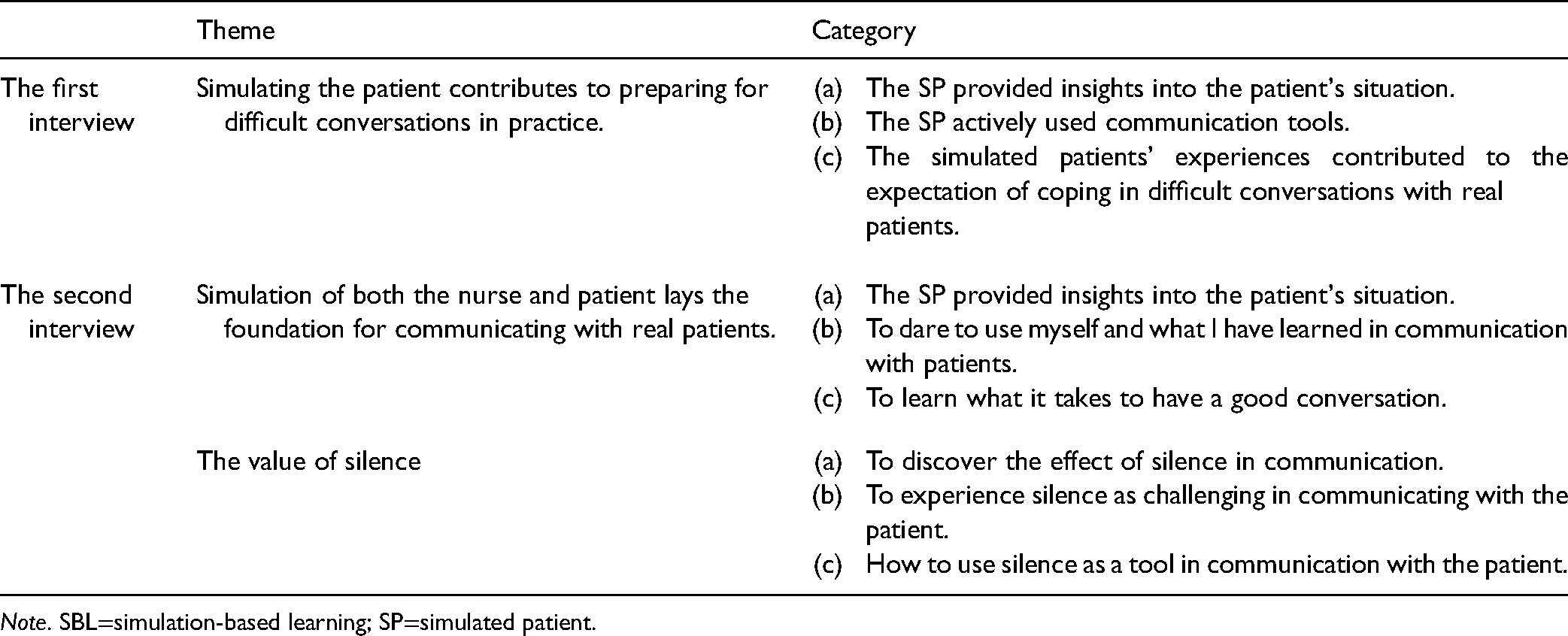
Note. SBL=simulation-based learning; SP=simulated patient.
Simulating the Patient Contributes to Preparing for Difficult Conversations in Practice
The students expressed that their previous experience with simulation and clinical practice and planning the patient scenarios was necessary for a good simulation experience. They experienced that being an SP provided them with insights into the patient's situation and they considered this valuable before they met real patients in clinical practice. In a way. I can understand the patient's situation, even if I can’t fully understand it.
In addition, the students found it instructive to observe how peers acted as SPs in the same patient scenario because “no patients are alike.”
Being the SP of the opposite sex and age was unproblematic, even though the students also described a vulnerability in doing this. Some patient roles were found to be extra challenging, for example, being a 70-year-old suicidal man. The student playing this patient was strongly affected by thinking about his situation. The emotions influenced the “nurse,” who became strongly influenced and felt sorry for the SP. This simulation was described as an “intense experience.”
In general, the SP actively used relevant communication tools focusing on learning objectives. Thus, the informants were aware of the response they should give and how to communicate to get the “nurse” on the right track. Being an SP required constantly thinking through what communication was about and being aware of the “nurse's” communication to adequately respond. The following is an example from a patient scenario where a motivational interview was the focus: the SP should answer yes or no if the “nurse” asked closed questions and answer in a complementary manner when the “nurse” asked open questions. Another example was a suicidal SP who should only respond when the “nurse” sat close to her and touched her, highlighting the importance of nonverbal communication. Eventually, the SP would respond positively to the fact that the “nurse” spoke to her.
The informants described that both simulating difficult conversations and playing a patient contributed to experiences that they would bring into practice, along with an expectation of easier mastery of challenging communication. One informant expressed that she had previously dreaded meeting patients suffering from dementia alone in homecare nursing practice, but simulating patient scenarios had contributed to insights into both the nurse and patient perspective, increasing her self-confidence: It's as if pieces fall in place. You experience it in a scenario and practice it out in the clinic.
Simulation of Both the Nurse and Patient Lays the Foundation for Communicating with Patients
After clinical practice, the informants confirmed that simulation had been appropriate in preparing for practice and had contributed to insights into what awaited them. Both roles were perceived as useful forms of preparation. However, it was being an SP that had given them insights into the patient's situation. In retrospect, simulation with different SPs was considered useful and instructive, preparing them for similar situations in practice: Being a patient in simulation gave me an increased understanding of what it can feel like to be a mentally ill patient.
Simulating difficult meetings with suicidal patients and patients suffering from dementia was highlighted as the most important preparation for practice. They thought they could more easily understand the dementia patient's feeling of not being understood after they themselves felt this through simulation. Furthermore, this experience contributed to reflections in and on practice regarding the patient's autonomy and user participation.
SBL contributed to an awareness of one's own communication with patients. This was illustrated in encounters with aggressive patients where nonverbal communication, the use of posture, and eye contact were recognizable from the simulation: Just how to stand and where to look … Does she get angry now when I look her in the eye? No, I’m looking down … No, that's not right. Then she asks, “Aren’t you looking at me?” Where should I look?
The informants highlighted communication competence as highly valuable in nursing practice. They were now more aware of how they could use themselves as tools; this was particularly important for their practice in mental healthcare and at homecare nursing, in which there are different requirements for communication skills than in a somatic ward. Simulating difficult conversations was considered “invaluable for my own security and self-esteem.” They began to use what they had learned in meetings with real patients to a greater extent.
The Value of Silence
Both in simulation and practice, the informants had become aware of the value of silence in communication. The topic was not emphasized in teaching; they had discovered the effect by chance during simulation, especially because the facilitator was silent during the debriefing. This allowed for reflection. In clinical practice, the use of silence could be challenging, demanding, and difficult to relate to: The challenge has been the silence in conversations. Then, I tense my toes, bite my lips and want someone to say something.
The students struggled with “the terrible silence”; it could be almost “unbearable.” Several expressed that in practice, they had to work with themselves to learn to “endure the silence” and were trained to use silence as a tool in conversation. Similarly, they developed an awareness of not expecting the patient to talk because of illness. Being quiet with the patient could be sufficient. Silence was perceived as both an effective communication tool and a natural response in conversations with patients.
To sum up, the informants described a learning process that included discovering the importance of silence in conversations with patients, learning to tolerate silence, learning to use silence as a tool, and learning how silence could be broken in a constructive way by using appropriate question formulations.
Discussion
Our findings suggest that simulation as a form of practice preparation gives the student an increased understanding of both the patient's perspective and the student's own role in meeting the patient.
We discuss the findings from two perspectives. First, the nursing student as the SP is oriented toward peers’ learning and the real patient in future practice. Second, the nursing student in clinical practice is oriented toward the real patient's experience, hence using their previous experience from SBL.
A complex learning situation emerged from the first focus group interview, in which the nursing student as an SP had to relate to several perspectives and roles at the same time: (A) must use prior knowledge from theory and practice; (B) must be focused on the purpose of SBL and peer student's learning; and (C) must imagine the “patient” as a real patient.
Previous simulation experience, relevant theory, overall goals, and clinical experiences are important ingredients when students plan a simulation with a relevant patient scenario. Planning involves various action options in response to what the “nurse” says or does. The planning provides insights into the scenario and active ownership of the SP. When students themselves plan a simulation, it provides a more thorough preparation than teacher-led SBL (Svellingen et al., 2021).
When simulating, the student as an SP must have two thoughts in mind at the same time: achieving the learning objectives and the well-being of their peer. An important issue is to promote learning for the peer “nurse.” The SP must find a balance between the fact that one must practice communication skills while taking care of the other's well-being. Thus, students as SPs themselves practice relevant communication strategies and learn to respond in different ways. The students also learn from observing peers’ play and developing their repertoire of actions. Like Dalwood et al. (2020) and Mackey et al. (2014), we found that SBL contributes to an increased understanding of the importance of nurses’ communication skills and a deeper understanding of the patient. In contrast to our study, both Dalwood et al. (2020) and Mackey et al. (2014) studied teacher-led simulation with senior students instructed by the teacher when simulating patients for junior students.
When simulating the patient in a difficult conversation, the student does not have full control over the situation. Role cards can be a good, but not complete, tool. The SP must be flexible and able to improvise. The fact that students with ownership of patient scenarios simulate patients rather than use external standardized patients can be an advantage for peer students’ learning. As SPs, students are oriented toward the learning process in another way than an external person is. The patient's role can be safer and more engaging because they familiarize themselves with the patient (Dalwood et al., 2020).
In some scenarios, the interaction between the “nurse” and SP resulted in strong emotions; they dove down so deep into the role of the patient that it affected both their bodies and emotions. The students were not prepared for this. However, they perceived it as positive because emotional expression increased insights into the patient's perspective. Because emotions may be expressed in simulation, it is important to take care of the well-being of the SPs throughout the simulation, even after debriefing (Dalwood et al., 2020; Nestel et al., 2017). Bearman et al. (2015) concluded that the emotional aspect of both roles in simulation can be key to developing empathy with the patient and that switching roles can increase students’ reflection, contributing to them seeing the patient's perspective. However, one should consider the possibility of students having strong emotional reactions. This is particularly important in student-led simulation; the teacher must supervise during the planning and be available and attentive during the simulation, including the debriefing session.
Simulating a difficult conversation provides useful experiences with relevant communication tools and empowers nursing students to master such in practice. The fact that they are SPs and can experience the “other perspective” in interaction with the “nurse,” besides acting as a “nurse,” greatly contributes to this perception. Students learn by reflecting on being met in an appropriate or unfavorable way and by looking at how they can adjust to the conscious use of communication tools. SPs play an important role in giving feedback to the “nurse” during the debriefing. The role pair can share their experiences and reflect together, contributing to an increased understanding of the “other” in both roles. Our findings indicate that peer simulation, regardless of acting as an SP or “nurse,” contributes to a pronounced belief in mastery in clinical practice. This is consistent with the findings of Mackey et al. (2014), Mandrusiak et al. (2014), and Springfield et al. (2018). The last two of these studies explored physiotherapy students.
Experience as an SP gave the students insights into the patient perspective, creating a positive effect on clinical practice. Previous research (Dalwood et al., 2020; Mackey et al., 2014) has concluded that peer simulation is useful for learning communication skills and developing empathy because students gain insights into the patient, but these studies have not explored the learning effect on practice as we did. Our findings indicate that student-led simulation with students as SPs can be beneficial for learning communication skills and strengthening students’ security and self-esteem when they enter into clinical practice. The dynamics between patient and nurse roles contribute to students’ awareness of communication with real patients. With positive learning outcomes in simulation, students become more confident and have positive learning experiences in practice. Students bring experiences from both roles into practice. Hence, SBL should include learning objectives for SPs.
We found that the students learned of taking the other's perspective by alternating between playing the patient and nurse. This is an important finding that strengthens both student-led simulations as a pedagogical method for learning communication and the use of students as SPs. Other studies have shown similar results (Dalwood et al., 2020; Mackey et al., 2014), but they have not explored the consequences of the practice.
Our findings can be interpreted in light of Position exchange Theory (Gillespie & Martin, 2014). In a student-led simulation of communication, the interaction between the “nurse” and the SP is the focus, and the students take turns playing the two roles (position exchange). Being oriented toward the other adds a new dimension in terms of understanding the patient perspective in future clinical practice. The SP's experiences can be understood as “if I were the other” and “if this happened to me.” Here, the perspective of the other is cultivated, entailing “the other-within-self” (Gillespie & Martin, 2014). It can also be related to taking the perspective of the peer student as a “nurse” and the notion of oneself as the future nurse in practice. In practice, the nursing student remembers “the other-within-self” from SBL.
The use of silence in communication is such an example. Silence is a powerful and valuable communication tool (Bassett et al., 2018; Hill et al., 2003). The SPs used silence as a tool in the meeting with the “nurse,” but also experienced the impact of silence when the “nurse” was silent. Although the communication literature in the nursing study consists of silence as one important communication tool, it appears to be new knowledge for the students. It seems that the students gradually gained an understanding of the value of silence when simulating difficult conversations. This can be interpreted with position exchange theory: one gains a bodily understanding of other social positions when one steps out of one's own social position and play another social position (Gillespie & Martin, 2014). In clinical practice, students bring their embodied understanding of being the patient and train on being silent with real patients. The topic of silence should be emphasized to a greater extent in communication training.
Strengths and Limitations
The current study includes a relatively small sample size, a convenience sample, and was conducted within one institution. However, the purpose of the study was to explore students’ experience over time. Therefore, it is a strength that the same group was interviewed twice over a period of six months. According to the literature on multistage focus group interviews, one group can be sufficient when the same group is followed over time (Hummelvoll, 2008, 2010). Moreover, no similar comparable longitudinal studies were found, so we recommend that future studies explore what impact playing the patient role has on nursing students’ clinical practice.
Implications for Practice
The findings indicate that it is essential for SBL and for clinical practice in mental healthcare and homecare nursing that students take on the role of the patient when simulating. Therefore, students should be prepared for and perform as SPs more often. By taking on both roles, learning is enhanced. The learning objectives in SBL should be related to both roles and the interactions between them, not only the nurse's role.
The following are success criteria when students take on the role of SPs: the students become familiar with SBL; they have ownership of “their patient”; a well-functioning group dynamic exists; and the students are confident with each other. To practice therapeutic communication during education can be challenging for nursing students. Therefore, teachers should be close to student-led simulation and aware of students’ reactions.
Conclusion
SBL of difficult communication ensures increased attention in clinical practice on how to use oneself to contribute to good communication and learn from others, and it can be a positive learning experience that influences nursing practice and confidence.
The findings indicate that role exchange when students roleplay both as the patient and nurse gives students a greater understanding of the patient perspective, and they benefit from this when communicating with patients in clinical practice.
Footnotes
Acknowledgments
The authors want to thank the students who participated in the focus group interviews and other members of our research group who have given valuable feedback on the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.