
Abstract
Objective
To investigate evidence-based nursing practice among nurses in Ghana.
Methods
This is a descriptive cross-sectional survey and data was collected among clinical nurses and nurse educators from both private and public institutions across Ghana. Nurses were included if they have full-time or part-time appointment; were in active service and have a valid Personal Identification Number (PIN) from the Nursing and Midwifery Council of Ghana.
Results
About half of the nurses disagreed or were neutral regarding formulation of answerable research questions and 40% do not critically track relevant scientific evidence. Also, more than 30% of the nurses disagreed or were neutral regarding the integration of scientific evidence into practice. Clinical nurses were about 2.1 times more likely to have difficulty determining the applicability of research findings in service delivery compared to nurse educators.
Conclusion
The findings suggest EBP uptake and integration is suboptimal in Ghana.
Introduction
There is no doubt that nurses are in the frontline of service delivery in the healthcare industry more than any other health professionals. Therefore, the application of scientific knowledge in nursing service delivery is critical for the healthcare industry. The application of scientific knowledge is one of the cost-effective ways of reducing errors and improving patient outcomes. However, many nurses do not possess adequate knowledge and skills required for evidence-based nursing practice (Pravikoff et al., 2005). The reliance on knowledge passed on from generation to generation as new nurses are recruited into the profession and drawing from past educational instructions to make decision about individual nursing practice are common to the nursing profession. These however may not be sustainable for the high demand of technology in the healthcare industry. The nursing profession in the 21st century requires service delivery in a highly specialized nursing environment, with a high degree of professionalism and optimum patient outcome.
Considering that nurses require a cognitive process of applying knowledge and experience in clinical decision-making process, Evidence-based Nursing Practice (EBP) may provide a great opportunity for moving nursing care to a level that may involve clinical reasoning. By this, nurses will be able to meet the demand in the 21st century and beyond thus, improve patient outcome and cost containment.
Review of Literature
EBP is a process by which evidence in nursing practice is critically evaluated and considered in relation with patient for informed practices, optimum nursing care and patient outcomes (Scott & McSherry, 2009). It involves an attempt to bridge the gap between research and practice where nurses are able to evaluate research, clinical guidelines or procedure manuals and other relevant information based on scientific findings and apply the outcomes to practice. Unlike traditional decision-making processes in clinical practice which relies largely on expert opinion through experience acquired on the job over years of practice, EBP involves integration of best research evidence (Mohsen et al., 2016). In addition, traditional decision-making process is likely to lead to poor patient outcomes whereas EBP is a critical step in improving healthcare quality as well as the ability to enhance personal and professional performance of nurses (Chien et al., 2013; Mohsen et al., 2016).
Even though nurses are taught courses such as research methods, therapeutic communication, nursing theories, these courses are taught largely through classroom teaching with little clinical exposure. The classroom model of training in which nursing education is largely focused on information literacy is not sufficient for EBP, instead identifying research problems in clinical settings and relating research evidence to practice is an important pre-requisite for EBP. Professional regulatory bodies recognize EBP in the healthcare community as the acceptable standard for service delivery. For instance, the International Council of Nurses (ICN) has encouraged nurses to be actively involved in research and apply research scholarship to develop EBP (Mohsen et al., 2016). However, it is not clear what nurses in Ghana base their clinical decisions on. This study therefore documents evidence-based nursing practice and barriers among nurses in Ghana.
Methods
Design
This study presents results from a nation-wide descriptive cross-sectional survey conducted between November 2019 and July 2020 among 480 clinical nurses and nurse educators. These nurses were identified from private and public institutions in Ghana.
Research Questions
The study addressed the following research questions:
What is the level of evidence-based nursing practice in Ghana? What are barriers to EBP among nurses in Ghana? What factors are associated with EBP among nurses in Ghana?
Sample
We employed a multi-stage sampling technique to identify the training institutions and selection of the study participants. In the first stage, teaching hospital and training institutions were purposively sampled based on the number and geographical distribution across the country. A population frame of all nurse educators at the training institutions in this study were considered. This is because there are not many nurse educators at the nursing training institutions in Ghana compared to clinical nurses. With regards to the teaching hospitals, professional nurses were conveniently sampled. The recruitment strategy involved the research team to be present at the study sites and approach professional nurses from the different departments across the hospitals. Information about the study and the participant information and consent form was provided to potential participants. Participants were included if they submit signed consent form.
The Raosoft sample calculator (Raosoft, 2004) was used to estimate the required sample size for this study. With an estimated population size of 1,500 professional nurses at the three selected teaching hospitals, a margin of error at 5%, confidence interval of 95% and a default distribution of 50%, the estimated sample size was 306 nurses. Considering non-response and withdrawal from the study, 20% (n = 61) was added to the originally estimated sample size. Thus, a total of 367 clinical nurses were estimated for this study. About 123 nurses were sampled from each of the three teaching hospitals identified from the Northern, Middle and Southern parts of Ghana.
Inclusion and Exclusion Criteria
The study included both clinical nurses and nurse educators. The clinical nurses were recruited from three teaching hospitals in Ghana. There are five teaching hospitals in Ghana and in the Ghanaian context teaching hospitals are tertiary health care facilities. The teaching hospitals serve as referral facilities for Regional Hospitals and clinical attachment sites for universities training health professionals, including nurses. Nursing education in Ghana is done at two main levels: the diploma and bachelor's degree. The Universities have the mandate to train degree holders in nursing whereas the nursing training colleges churn out diploma holders. The nurse educators were identified from five universities in Ghana (three public and two private) and eight nursing training colleges in Ghana. Nurses were included in this study if they were working on full-time or part-time basis; were in active service and have a valid Personal Identification Number (PIN) from the Nursing and Midwifery Council of Ghana. A full-time job appointment requires teaching the minimum required credit load at the training institution or working 40 h per week at a healthcare facility. A part-time job appointment requires the nurse educator to teach fewer credit load or a clinical nurse to work fewer hours per week. Auxiliary nurses, health assistants and nurses on retirement/contract were excluded from this study.
Data Collection Instrument and Outcome Measure
Paper-based and closed-ended questionnaires were self-administered by the participants. Depending on the preference of the respondent, the completed questionnaire was collected instantly or on a later date convenient to the participants. Data were collected on participants’ socio-demographic characteristics, teaching curriculum, hospital procedure manuals, the use of EBP in teaching and clinical practices and barriers to EBP. The survey instrument was adopted from previous EBP studies (Majid et al., 2011; Mohsen et al., 2016; Upton & Upton, 2006) that reported reliability coefficient (Cronbach's alpha) for each subscale exceeding 0.70 and good construct validity. Additional variables were included to identify barriers to teaching EBP. There were six items measuring the use of EBP and these items were scored on a 7-point Likert scale (from 1 to 7 response options). Point 1 on the scale indicates poorer and 7 indicate higher scores for EBP. The subscale measuring barriers to EBP has six items and the participants were required to respond “yes” or “no” to each item.
Data Quality Control
The questionnaire was pre-tested among 20 nurses at the Ho Municipal Hospital for accuracy in measurement soon after the training of the research assistants. This is to assess the acceptability, appropriateness of wording and suitability of the instrument and to ensure that the instrument measures what it was intended to measure and suitable for the intended purposes. The pre-testing further gave the researchers the needed experience and opportunity to correctly administer the instruments during the main study. The principal researcher was directly involved in the field work to ensure that the questionnaires were properly administered and blank questions were filled appropriately. The data was double entered into SPSS software; a check for consistency was done and all the inputted data were agreed upon. The data were finally coded appropriately for analysis.
Statistical Analysis
The data were analyzed using SPSS software package. Basic descriptive statistics were used to summarize the data and presented as medians and interquartile range (IQR) for the ordinal level data. The Mann-Whitney U-test was used to compare mean rank scores of barriers to EBP between clinicians and nurse educators and p-values less than 5% were considered significant. Kruskal Wallis H-test was used to compare mean ranks of three groups (Nurses educated above BSc, BSc level and below BSc) and Spearman correlation test was also used to test for significant relationship between participants’ socio-demographic characteristics and the Use of EBP; nursing competencies and barriers to the use of EBP. The results are reported in tables and figures.
Ethical Considerations
Formal ethical approval was obtained from the University of Health and Allied Sciences, Research Ethics Committee (REC) (Approval No. UHAS-REC A.1 UI 18–19). The study was also performed in accordance with the ethical standards as set forth by the UHAS -REC. The data for analysis did not include any identifying information on the nurses. Administrative approval was obtained from all the institutions involved in this study. Potential participants were verbally invited to participate in the study and written informed consent was be obtained from the study participants before there were enrolled in the study. The Participants Information and Consent Form (PICF) explain the purpose of the study and indicate that there will be no immediate benefit for participants. It also emphasized that participating in the study was voluntary and that deciding for or against participation or withdrawing from the study at any time will not influence any relationship with the participants. With regards to risk, there wasn’t any risk associated with participation. To ensure confidentiality, the participants and the institutions involved were given unique identification numbers assigned at the beginning of the interview by the Principal Investigator. This unique identification number was known to only the Principal Investigator.
Results
Sample Characteristics
A total of 480 valid responses from clinical nurses and nurse educators in Ghana were analyzed by this study. The Socio-demographic data include sex, marital status, religion, educational qualifications, work arrangement and age (Table 1).
Socio-Demographic Characteristics.

The overall mean age was 32.62 ± 7.44 and clinical nurses were younger (30.30 ± 4.66) compared to the nurse educators (41.91 ± 9.07). A majority (80.0%) of the nurses were clinicians, 60.2% were females, more than half (56.5%) of the nurses were married at the time of the data collection. A majority of the nurse educators (81.2%) were educated at or above Bachelor's degree whereas a majority of the clinicians (95.9%) had a bachelor's degree or lower, largely working full-time (96.4%) with less than or equal to 10 years working experience.
Information on Teaching Curriculum and Hospital Procedure Manuals
Data was collected on the teaching curricula at all the training institutions and on procedure manuals used for nursing procedures at the teaching hospitals. A summary of the responses is presented in Table 2 and Table 3 respectively.
Information on Teaching Curriculum.

Information on Protocols/Procedure Manuals.

All the training institutions had National Accreditation Board (NAB) accredited teaching curricula (100%), about 95% indicated that the teaching curricula has ever been reviewed and 67.0% indicated the review is done every 5 years. With regards to what instigated the curricula review, a majority (71.4%) indicated Research/Needs Assessment, followed by national accreditation requirements (47.3%).
Of the clinical nurses who indicated they have protocol/procedure manual at their facilities, more than half (50.3%) indicated that their procedure manuals were not regularly review and only 37.9% expressed that the review is done yearly. Regarding the reasons for the review a majority (58.0%) expressed that it was due to Research/Needs Assessment.
The use of EBP in Teaching and Clinical Practice
A total of six items were employed to assess the use of EBP among the nurses. These items included the ability and frequency to formulate answerable research questions, integrate available evidence into practice and evaluate outcome practice outcome. The nurses (both clinical and nurse educators) were asked to indicate their level of agreement to the statements measuring EBP and the responses of the nurses are summarized in Figure 1.
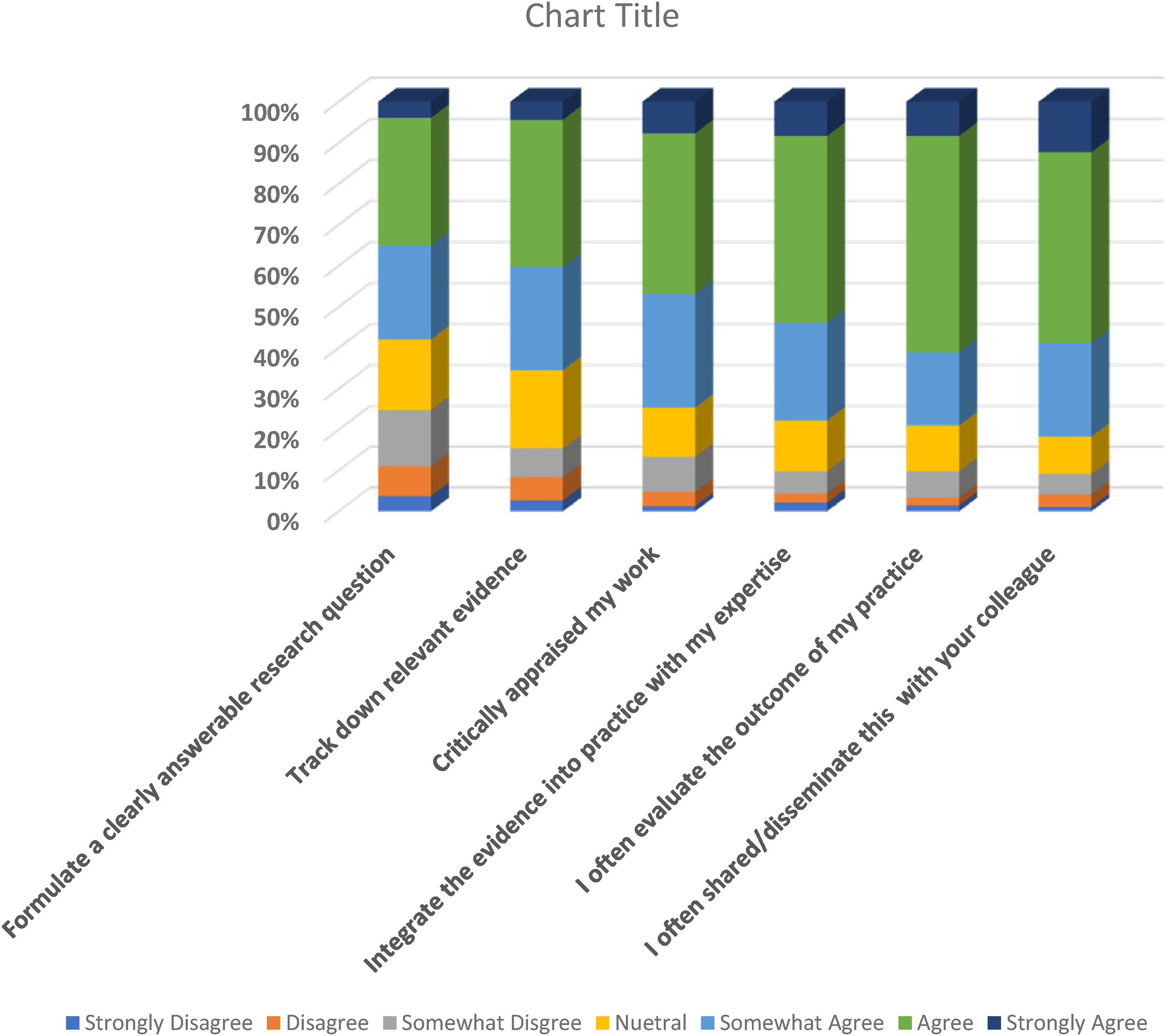
Use of EBP.
More than half of the nurses at least, agreed with all the items measuring the use of EBP and about 20% somewhat disagreed with the formulation of a clearly answerable research questions at work. About 20% disagreed or were neutral to integrating evidence into practice with their expertise.
Barriers to EBP by Nurse Category
To determine whether there is any significant difference with regards to barriers to EBP between nurse clinicians and educators, a chi-square analysis was performed. The results are presented in Table 4.
Barriers to EBP by Nurse Category.

*COR: crude odds ratio.
There were significant differences between clinicians and educators regarding judging the quality of research articles and reports (p = 0.031) and determining the applicability of research findings (p = 0.008). Clinical nurses were 2.074 times more likely to have difficulty determining the applicability of research findings in service delivery compared to nurse educators. Also, clinical nurses were 1.741 times more likely to have difficulty in judging the quality of research articles and reports compared to the nurse educators.
The use of EBP was significantly higher among married participants (5.50), Christians (5.33), nurse educators (5.67) and nurses who have worked for more than 10years (5.83). There were no significant differences between the sex of the nurses and their work arrangement as presented in Table 5.
Socio-Demographic Characteristics and Use of EBP.

Variable Association to EBP
The Kruskal-Wallis test (one-way ANOVA on ranks) was used to assess association between nurses’ level of education and the use of EBP as well as barriers to EBP. The level of education was recoded into three leve1s (1 = above Bachelor's Science (BSc); 2-a Bachelor's Science and 3-below a Bachelor's Science). The level of significance was set at p-values ≤0.05 and the results of the analysis are presented in Table 6.
Association Between Level of Education and the use of EBP and Barriers to EBP.

** – Statistically Significant.
EBP – Evidence-Based Practice.
KG – Knowledge.
BSc – Bachelor of Science.
IQR – Inter Quartile Range.
The Kruskal Wallis test showed that the use of EBP (H = 30.344, P < .001, df = 2) and barriers to EBP (H = 7.797, P = .020, df = 2) differ for all the educational level of the nurses. A post hoc test comparing i) nurses educated above BSc degree and those educated at only BSc level showed statistically significant differences across all the variables and ii) nurses educated above BSc level and below BSc level also showed statistically significant differences across all the variables. However, the comparison between nurses educated at BSc level and those educated below BSc level did not show any statistically significant differences across all the variables (Table 6).
Discussion
Evidence-based practice is gaining grounds since the introduction in 1992 and nurses must be proficient in evaluating and using research evidence in teaching and in clinical practice. This study therefore investigates evidence-based nursing practice among nurses in Ghana. The findings suggest that the uptake of EBP among nurses is suboptimal and nurses experience varying difficulties and barriers to evidence-based practices. Between 20% to 40% were neutral regarding statements such as tracking relevant evidence, integrating scientific evidence into their practice and evaluating their practice outcomes. About 20% somewhat disagreed with the formulation of a clearly answerable research questions at work. These findings are similar to previous reports among nurses working at a University hospital in Bergen, Norway and at Kenyatta National Hospital in Kenya. The nurses in Norway and Kenya mostly used knowledge acquired from work experiences rather than evidence-based knowledge (Dalheim et al., 2012; Kyalo et al., 2015) for clinical decision making. Determining the value and applicability of research findings contribute to the willingness and uptake of EBP and the lack of research skills could hamper the appreciation of the quality of research findings and its applicability to practice.
All the training institutions had accredited teaching curricula by the National Accreditation Board. The curricula are reviewed regularly based on research needs or for re-accreditation purposes. A majority of 88.0% of the clinical nurses also indicated they have procedure manuals and these manuals are reviewed regularly. The regular review helps to incorporate core competencies required to practice as professional nurses so as to meet the expanding demands of the healthcare industry.
Barriers to EBP identified by this study include difficulty in finding time to search for and read research articles; insufficient time to conduct research and inadequate facility for healthcare service. Also, about 30% of the nurses agreed that they had difficulty judging research quality and understanding statistical terms. These findings agreed with Dalheim et al. (2012), who also observed that insufficient time to conduct and apply research information and the lack of expertise as barriers confronting newly qualified nurses in Norway. This suggests the need to provide additional training and support to improve nurses’ skills with regards to the use of research evidence and knowledge translation. This may help to bridge the existing gap between clinical practice and theoretical knowledge.
Although nurses have difficulties regarding evidence-based practice, clinical nurses experience more difficulties. This current study found statistically significant relationships between clinicians and nurse educators in terms of difficulty in judging quality of research findings (0.031) and difficulty in determining the applicability of research findings (0.008). Clinician were more likely to have difficulty ascertaining the applicability of research findings, incorporating the information into practice and judging the quality of research articles and reports compared to their nurse educator counterparts. These findings confirm the inadequacy of relevant information and the lack of expertise among nurses (Baatiema et al. (2017). In addition, Hankemeier and Van Lunen (2013) also found lack of time as a barrier to EBP among approved clinical instructors in a teaching programe. Mulenga and Naidoo (2017) also noted the lack of appropriate skills in searching for relevant information as well as challenges with evaluating the efficacy of research findings as obstacles to the uptake of EBP among nurses working in a teaching hospital in Malawi. Effective pedagogical interventions to improve the teaching of EBP in nursing schools and in-service education can be developed based on the needs of nurses in addressing these challenges.
Considering that about half of the nurses in this study are mostly overwhelmed by workload it is understandable that time constraints are barriers to EBP among Ghanaian nurses. Additionally, internet challenges which is prevalent in most Ghanaian institutions could also add to the time required to search and retrieve relevant information. However, nurse managers must be encouraged to promote research among nurses at their facilities. There are reports that nurses do not engage in research after completing school. For instance only 26.0% of nurses were involved in research at the Kenyatta National Hospital (Kyalo et al., 2015). Models to enhance the research ability of nurses are urgently and translation of research evidence are needed to advance nursing science and ultimately improve nursing care and patient outcomes.
Strengths and Limitations
The study has shed light and provided insight into EBP among nurses in Ghana and further highlighted the differences regarding EBP between clinical and nurse educators in Ghana. Also, the response rate for this study was high among practitioners and educators and the findings support existing literature on barriers to EBP. The findings further added to science on teaching curriculum and hospital procedure manuals.
The study also has a number of limitations which should be considered when interpreting the results. First, the clinical nurses were not randomly sampled. Second, the study included only nurses working at teaching hospitals and did not include nurses working at private hospitals in Ghana. This may have some implications on the study findings. For instance, the views from the sample in this study may not be the representative of all nurses in Ghana.The study also acknowledges that data in this study were self-reported, which may have produced desirable responses leading to participants under-reporting or over-reporting information.
Implications for Practice
There is solid evidence that the level of education contributes positively to nurses’ use of EBP therefore as the health care industry continues to grow in sophistication, clients’ demand for quality care is also growing and the nursing profession must evolve and advance in education to accommodate these demands. It is important for nurses to enhance their knowledge and skills and embrace research evidence in decision-making in obtaining nursing education and practice.
Conclusion
The findings suggest that many nurses have difficulties in the uptake of EBP and integration of research findings into practice among nurses is suboptimal. Also, nurses have varying difficulties and barriers to evidence-based practices. Because the nursing profession is a critical component of the healthcare industry the science of nursing practice and education must develop through rigorous research and evidence-based practice.
Footnotes
Acknowledgments
We are grateful to the management of the research grant at the University of health and Allied Sciences, all the nurses who participated in this study and the ethics review board of the University of health and Allied Sciences for their guidance.
Compliance with Ethical Standards
Ethical approval was granted by the University of Health and Allied Sciences (UHAS), Research Ethics Committee (REC) (Approval No. UHAS-REC A.1 UI 18–19). The study was also performed in accordance with the ethical standards as set forth by the UHAS-REC. Informed consent was obtained from all students for being included in the study. The data for analysis did not include any identifying information on the participants.
Conflict of Interest
The authors declare that they have no conflict of interest.
Funding
The study was funded by the University of Health and Allied Sciences (UHAS) research grant.