
Abstract
Introduction Women had for years endured impediments at the workplace in many aspects such as gender inequity and low pace of career advancement. The status quo is persistent despite the enactment of legal frameworks institutionalized to redress gender disparities in the workforce. Aim This study strives to explore gender equity, assess the magnitude of women in decision-making and to ascertain impediments that humper career progression in nursing. Method This study utilized secondary data collected from a thesis titled ‘Gender equity and career progression in the Ministry of Health and Social Services in Khomas region of Namibia.The main study employed a mixed method approach to collect information through interviews. Tools Two separate semi-structured interview guides that comprised of both set of close-ended and open-ended questions were employed to gather information from selected respondents and the key informant. Results The conception that women in nursing are less successful in their careers in comparison to their male colleagues is contrary to the study findings as managerial positions at the studied institutions are held by women. Cultural factors are found to hold less significance in impeding career progression at Ministry of Health and Social Services as opposed to organizational hierarchical structure. Conclusion The feminization of the nursing career that led to the predominance of female in profession is still unopposed as the profession is not showing a sign of equilibrium of the two genders.
Introduction
For a very long time, women have been viewed as child-bearers and keepers of the home. Their roles have been homebound and have been limited to be active actors in the economic and social spheres unlike their male counterparts (Mwetulundila, 2019). However, with the rise of feminist movements and activists advocating for women participation in activities outside the home particularly in the labor force, the global arena has witnessed a promising flow of women entering the job market. According to Acker (2012) theorizing gender and organizations began in the late 1960s and early 1970s as feminist scholars criticized conventional organizational research as inadequate because it ignores the importance of gender in working life.
As posited by McIntosh (2010) in Mwetulundila (2019) stressed that generally women in nursing are less successful in their careers in comparison to their male colleagues. Reference is made to Scotland whereby the national statistics reveal that although there are high levels (89.9 percent) of female representation in nursing workforce, 27.6 percent of senior nurse manager positions are held by men. Men represent 10.1 percent of the nursing workforce. Many men who work in women's professions such as nursing experience a glass escalator effect that facilitates their advancement and upward mobility within these fields (Wingfield, 2009). Research findings indicate that subtle aspects of the interactions, norms, and expectations in women's professions push men upward and outward into the higher status, higher paying and more masculine positions within these fields. This phenomenon of barriers that prevent the ascension of women is complemented by the concept of ‘sticky floor’. This concept describes the forces that tend to maintain women at the lowest levels in the organizational pyramid (Still, 1997). Horizontal segregation is also widespread within the nursing profession that specialties chosen by men for their compatibility with male character traits include: psychiatry, because of its association with physical strength; anaesthesiology, because of its association with technical prowess and autonomy; and, intensive and emergency care, because of their association with technical competency and cool-headedness (Evans, 1997, p.228).
In Namibian the government has made advances in ensuring the elimination of many forms of discrimination in formal employment following the adoption of the Affirmative Action (AA) Act 29 of 2008 (Employment Equity Commission (EEC), 2015). However, this did not completely resolve gender inequality that had in the past been persistent. Echoing similar sentiments, Mufune (2013) points out that results from the Namibia Household Income and Expenditure Survey (NHIES) 2009/10 indicated that more Namibia women were increasingly entering into the labor force because of the post-independence policies. However, women still lag behind in many areas of labor force participation. The most common inequalities are the wage gaps between men and women and the sex segregation of jobs, occupations, and skewed hierarchal positions.
Literature Review
Nursing Force in Namibia
In Namibia nurses are classified as: pupil enrolled nurses, student nurses, enrolled nurses, registered midwives, professional also called registered nurses, senior professional nurses, chief professional nurses and chief control professional nurses (Washeya, 2018). All are governed by the Health Professional Council of Namibia (HPCNA) formerly known as the Nursing Council under the Nursing Act, Act No 8 of 2004. It is this Act that outlines the scope of practice for each category of nurse in Namibia. However, the scope of practice for the nursing profession may differ from country to country. The majority of these categories of nurses started their career in public healthcare facilities and later moved to the private healthcare sector. The private hospitals provide services to patients or clients with medical insurance and means of cash. During Namibia's 2009–2010 financial year it was reported that only 53 percent professional nurses were employed in Namibian public healthcare facilities, and 47 percent in the private sector (Washeya, 2018). The private sector also contributes to the training of nurses and currently Namibia has three nursing training institutions that provide professional nurse human resources after the government closed its training institution formerly known as National Health Training Centre. The three current institutions are; UNAM, International University of Management and Welwitchia University (Washeya, 2018).
Namibia's Interventions to Address Gender Inequalities
The Namibian government like many other governments across the globe institutionalized various laws and policies designed to redress inequalities in terms of gender. The Namibian Constitution explicitly forbids discrimination on the grounds of sex. Namibia also ratified the United Nations Convention on the Elimination of all Forms of Discrimination Against Women (CEDAW) in 1992 that advocates for member states to act swiftly against the discriminatory practices based on gender (Ruppel, 2008).
In 1997 the government adopted the National Gender Policy which marked an important step toward the attainment of gender equality in the country (Ministry of Gender Equality & Child Welfare, 2010). Amongst other government interventions, was the introduction of the EEC and formulations of policies and guidelines to guide the country in gender-related matters. The EEC became the custodian of the AA Act of 1998 under the Ministry of Labour and Social Welfare (EEC, 2002). This legislation fostered fair employment practices with regard to recruitment, selection, appointment, promotion, and equitable remuneration of previously disadvantaged persons. More specifically, previously disadvantaged persons such as women and persons with disabilities were referred to as the designated group.
Like the National Gender Policy, the AA Act's agenda is to close the gaps that were created by past socio-economic, political, and cultural inequalities that existed in pre and post-colonial Namibia. According to Holzer and Neumark (1996) AA policies have always been controversial, largely because of the allegation that they cause employers to prefer less-qualified minorities or females over more qualified males. The Employers’ Guidelines to the AA Act no. 29 of 1998 states that, “for the purpose of the Act, a suitably qualified person is defined as a person who has the abilities, formal qualifications or relevant experience for a position of employment” (EEC, 2002, p. 9). The government also introduced the Labour Act of 2007 which aims at regulating the conditions of employment of all employees in Namibia without discrimination on grounds of sex, race, color, ethnic origin, religion, creed, or social or economic status, thus, ensuring equality of opportunity and terms of employment, maternity leave and job security for women (Republic of Namibia, 2007, p.8).
Aim of the Study
This study strives to explore the magnitude of women in decision-making and to ascertain impediments that humper their ascension towards career progression.
Problem Statement
The problem of gender equity in many institutions is a universal concern. Various literatures on career progression indicate that women progress slow compared to men. Namibia is of no exception to this global phenomenon. With reference to the escalating statistics on gender disparities, as it has been indicated by the 2013/14 AA report, there is an urgent need to accelerate the implementation of the National Gender policy of 2010–2020 whose one of its priority area is women equal partaking in governance and decision making (Ministry of Gender Equality & Child Welfare, 2010). In this context, Acker (2009), stressed that the pattern holds even for women predominate fields, such as nursing or elementary school teaching, in which men move faster more quickly than women into administrative and leadership positions.
Theoretical Framework
There are a number of theoretical explanations for the general dearth of women in management positions. Such theoretical perspectives focused on the emphasis on the women's life context perspective, and one of the theory relevant to this study is the social role theory. It emerged in the 1980s and originated as an effort to understand the causes of sex differences and similarities in social behavior. Its underlying assumption is that men and women are assigned to different roles based on their gender. It uses more of a structural approach in understanding gender behavior. The structures that are most important to take cognisant of when examining the effect on gender based behavior are family, organizations, institutions and communities. It is assumed that these structures have caused men and women to act or behave in a certain way (Eagly, Wood and Diekman as cited in Eckes & Trautner, 2000).
From the social theory standpoint, socialization influences the society and there will be careers and roles that will be concentrated of more women and others will be concentrated of more men. Mills (2000) posits that although we are first socialized from a very young age by our parents, into different gender roles, the socialization process also takes place in society concerning occupations we pursue as men and women. For instance, “if perceivers consistently observe women caring for children, they are likely to believe that characteristics thought to be necessary for child care, such as nurturance and warmth, are typical of women,” (Eagly & Steffen, 1984, p. 735). Thus, in a profession like nursing which is attached to caring and nurturing, women tend to be more predominant, whilst blue collar jobs are dominated by more men. Again, if one digs in the profession such as nursing, it is evident that certain roles that require hard labor for instance at the intensive care units, more men are assigned in those roles. This brings in the concept of horizontal segregation which is understood as under (over) representation of a certain group in occupations or sectors not ordered by any criterion. Horizontal segregation refers to the concentration of women and men in professions or sectors of economic activity (Meulders et al., 2010). Also the concept of vertical segregation surfaced in some countries which exists when men and women both work in the same job categories, but men commonly do the more skilled, responsible or better paid work (Blackburn & Jarman, 1997). In this regard, Juliff et al. (2016) argued that gender based roles and matters around intimate touch nursing care have been suggested as a reason why men in nursing migrate more towards the technical, rapid assessment areas of emergency and intensive care. According to the social role theory, it is widely believed that men and women possess certain qualities and traits that predispose them to the type and nature of roles they typically occupy (Eagly, Wood & Diekman as cited in Eckes & Trautner, 2000). Behavior is then modeled after such stereotypes, due to demands placed on them by society.
Significance of the Study
It is hoped that the findings would yield vital information on the MoHSS status quo in terms of gender equity and impedes of career progression. The study would also create an understanding on factors that inhibit women partaking decision making designations and career progression at MoHSS. The data presented in this report could also serve as a tool to raise awareness on the importance of gender mainstreaming at all levels at the MoHSS which might be relevant to any other work setting particularly the government establishments.
Methodology
This study relies on secondary data collected from a thesis titled ‘Gender equity and career progression in the Ministry of Health and Social Services in Khomas region of Namibia (Mwetulundila, 2019). This analysis focuses on equity in terms of gender and specific impedes that hinder career progression in nursing.
Design
The study employed a mixed method approach by following a convergent design. Under this design, the researcher converged and merged the qualitative and quantitative data by gathering the data simultaneously, then integrate the data, thereafter, perform a complete analysis of the data before giving a general and complete interpretation of the results (Creswell, 2014; Leavy, 2017). Hence the analysis of the findings are based on secondary data collected from a purposive sample of twenty two nurses from different nursing classifications and a human resources deputy director in Khomas region.
Population and Sample
The population for this study consisted of all professional nurses in Khomas region at all public clinics, public health centers and public hospitals. According to statistics as provided by the deputy director of the human resources directorate of the ministry, there are about 590 registered nurses and 587 enrolled nurses in Khomas region, 30 percent of the given population are said to be males. These statistics are provided by MoHSS human resources department. A purposive sample of 22 respondents from the following nursing designations treated as strata; enrolled, registered, senior registered and chief registered nurse represented by four respondents respectively. For control registered nurse both incumbents were automatically chosen because they are only two in Khomas. Additionally, one in-depth interview was administered with the human resources director as key informant from the MoHSS. Due to busyness as experienced by nurses, their daily work practice is often characterized by a hectic pace in the execution of tasks. As noted by Govasli and Solvoll (2020) previous research shows that busyness can potentially lead to a reduction in the quality of nursing. As this study was conducted during working hours, it was a challenge to get more nurse to partake in interview discussions hence the sample was reduced to 22 nurses. Attempts were also done to conduct interviews during free time such as lunch, off days and after work which was not so ideal to most nurses.
Setting
The study was conducted in Khomas region which is one of the fourteen regions of Namibia. Khomas is cantered on the capital city Windhoek where data collection was specifically confined due to its high population than of the few settlements on its outskirt hence the study was conducted at two main public hospitals, one public health center and nine public clinics in Khomas region. This implies that all public hospitals, health center and clinics within Windhoek's jurisdiction formed part of the study.
Tools for Data Collection
Two different semi-structured interview guides were designed in line with the objectives and literature review, consisting of open and closed-ended questions and were employed to collect information from respondents and key informant.
Data Analysis
Quantitative data that was captured, it was processed using the Statistical Package for Social Sciences (SPSS). SPSS generated basic and descriptive statistics that include frequencies and percentages were used for analysis of data. Results were then presented in table format for easy interpretation. For the qualitative data collected, the researcher adopted the five-step approach, which enabled the researcher to analyse the text and all other documents. The five-step approach allowed the researcher to compile the data (Step 1), disassembled the data for removal of irrelevant themes (Step 2), reassembled the data by coding and clustering into meaningful themes (Step 3), interpreted the meaning of the data by identifying recurring patterns (Step 4), and finally, concluded by summarizing the established findings of the study (Step 5) (Yin, 2011). For document analysis which will help strengthen the findings of the study, the researchers read through existing literature on gender equity and obstructs of career progression in nursing, whilst writing down bullets the emerging relevant points in a notebook, which were later arranged into themes and categories. Through this approach of analysis, the researcher was able to detect persistent themes and patterns whilst conducting the interviews and the data, and was able to create categories and themes before presenting the data through descriptions and tables (Creswell, 2013). A total of two themes and four subthemes were generated as depicted in Table 1.
Themes and Subthemes.

Source: Interview Data, 2019.
Ethical Considerations
Ethical clearance for the main study was obtained from UNAM's Post Graduate Committee and thereafter at MoHSS’ directorate of research. After the approval of MoHSS, nurses in charge at the identified sites were informed. Written informed consents were obtained from the respondents before the execution of interviews. Respondents were informed about the objective of the study, their voluntary participation and their right to withdraw from the study at any time without any recrimination and anonymity and confidentiality were maintained throughout. The informant consent stipulated that the findings will be made public and the researcher may perform further analysis as long as confidentiality is maintained. Lastly the study declare that an ethical statement is not applicable as it does not involve human or animal research.
Results
Socio-Demographic Characteristics of Respondents
The study recruited 22 nurses from all different nursing classification and one deputy director of human resources of MoHSS in Windhoek of Khomas region in Namibia. Table 2 depicts the socio-demographic characteristics of the studied sample (n = 22). As presented in Table 1, the highest percentage of the nurse are female (68.2 percent) and majority of the interviewed respondent ranged from 20 to 30 years old accounting 31.8 percent. Those in the age group of 31–40 years old were 27.3 percent followed by the group of 41 to 50 years old who were 22.7 percent and 18. 2 percent from the age category of those aged 51 to 60 years of age.
Characteristics of Sampled Participants (N = 22) (%).

Source: Author's own.
Concerning marital status the majority of studied nurses (68. 2 percent) were never married, 27.3 percent of the respondents were married and 4.5 percent of the respondents were widows. In terms of qualifications, the highest percentage of the studied nurses (45.4 percent) had a diploma in nursing followed by certificate holders accounting for 27. 3 percent. Of the respondents, 18, 2 percent had a bachelor's degree whilst 9.1 percent of the respondents had a master's degree and none holds a PhD/Doctoral degree.
The three nursing classification namely; enrolled, registered and senior nurses all accounted for an equal participation of 27.3 percent respectively whereas chief registered nurse and control registered nurse portfolios accounted for 9.1 percent respectively. Table 2 further shows that 41 percent of the respondents worked for more than 19 years whereas, 3.1 8 percent of respondents worked for less than 3 years. A total of 13.6 percent indicated that they have been working for 7 to 10 years, while 9.1 percent of the respondents were reported to have been at MoHSS for 3–6 years and the remaining 4.5 percent worked at MoHSS for a period of 11–14 years. Lastly Table 1 illustrates the number of years nurses remained at the current designations. A total of 41 percent nurses are reported to have remained at their current designations in a range of three to six years followed by 31. 8 percent for those reported to remain at the current positions in less than three years. Respondents that remained at their current positions in the group range of 7–10 years were reported to be 18.2 percent and the range of 15–18 years as well as 19 years and more reported 4.5 percent respectively.
Promotion by Sex
Table 3 illustrates the percentage of the respondents by sex that have been promoted and those that were not promoted. Out of all the females interviewed, 46.7 percent had been promoted, whilst out of all males interviewed, 42.9 percent had been promoted.
Promotion status by sex (%).
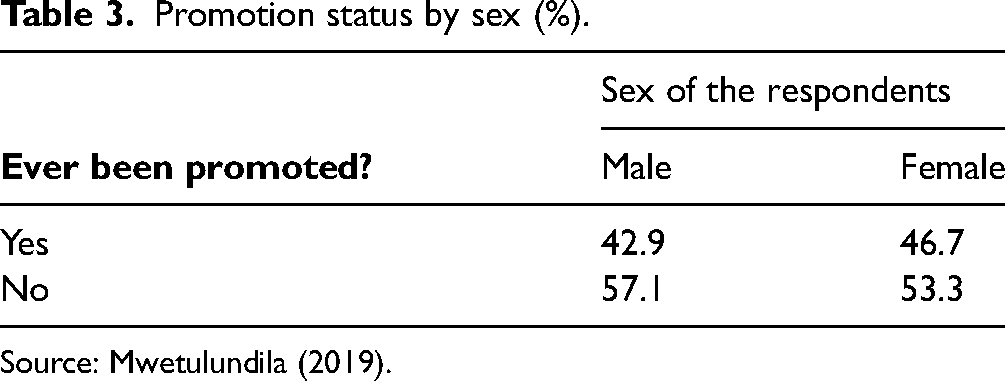
Source: Mwetulundila (2019).
Disaggregation of Female and Male Across Education, Years of Service and Top Positions
A disaggregation of male and female nurses across qualification, length of stay in service as well as in managerial positions was performed as illustrated in Table 4. Among respondents, there were two masters holders from both genders and five female nurses hold bachelor degrees as opposed to one male nurse. There were also six female diploma holders and three male diploma holders. For certificate holders, female nurses were four and male nurses were two. Table 4 further shows that more female nurses (7) have stayed in service for 19 years and more compared to one male nurse that stayed for a similar period. The similar pattern is observed for nurses that have been in service for less than three years whereby female nurses are more (5) as opposed to two male nurses. Lastly the depiction is on the incumbents of the three top positions of which all two control registered nurses in whole hierarchy of MoHSS in Khomas region are occupied by female nurses. Of the interviewed respondents, five female nurses were chief registered and one chief registered male nurse.
Disaggregation of Female and Male Across Education, Years of Service and top Positions (Headcounts).
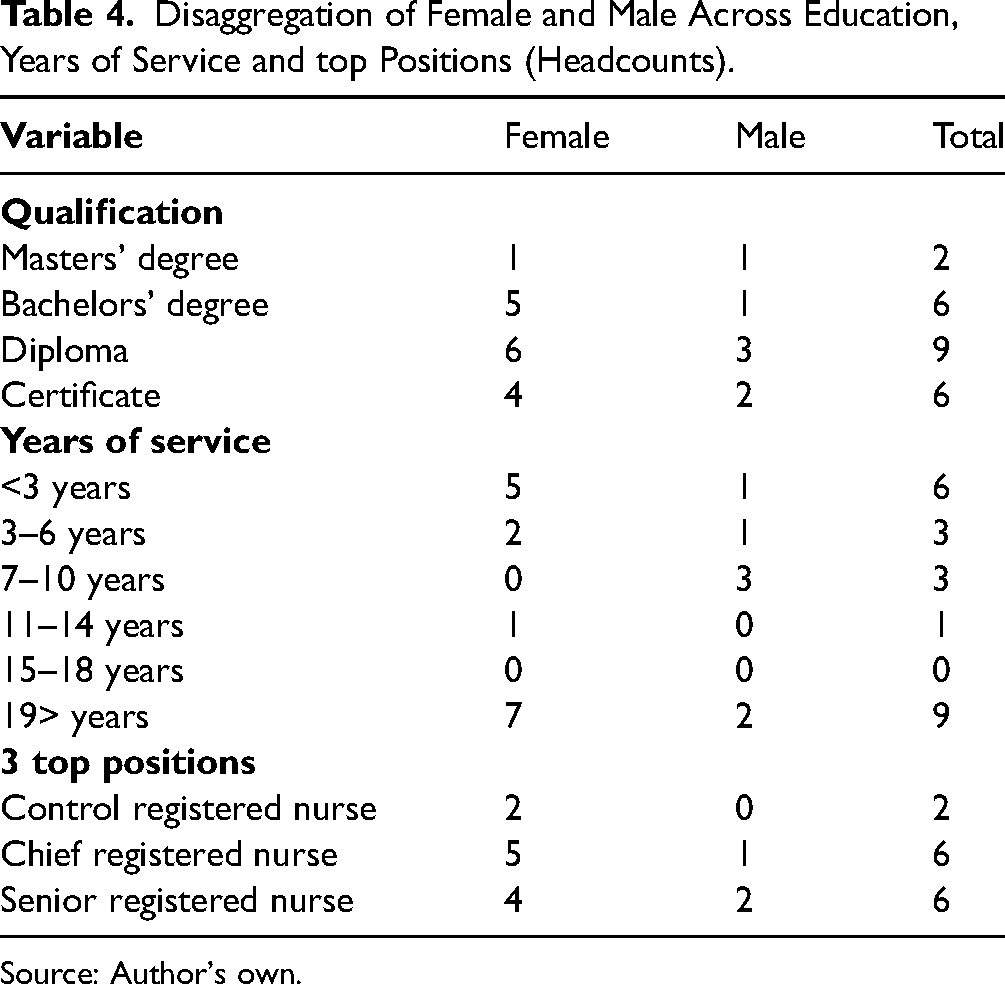
Source: Author's own.
Nurses Perception on Career Progression
Table 5 presents responses from the respondents with different nursing qualifications as assessed. Most of the respondents hold diplomas and viewed career progression at the institution as weak (80 percent) while 20 percent viewed it as moderate and none of the respondents in this category perceived it as good. Second in describing career progression as weak were nurses with Bachelor's degrees (75 percent) and 25 percent who perceive promotion at MoHSS as moderate.
Perceptions on Career Progression by Level of Education (%).

Source: Mwetulundila (2019).
Promotion by Years of Service
The results in Table 6 shows that there were no enrolled nurses worked for less than three years and got promoted, however 4.5 percent of those who worked for 4–6 years were promoted. For registered nurse that worked for less than three years and for more than 19 years, 4.5 percent were promoted respectively. Senior registered nurse who worked for a period of 7 to 10 years and 11–14 years, 4.5 percent were promoted respectively and also those that worked for more than 19 years, 18.3 percent also received promotions. Chief registered nurse and control registered nurse who have been in service for more than 19 years, 19.1 percent were also promoted respectively.
Promotion status by Years of Experience (%).

Source: Mwetulundila (2019).
Promotion by Level of Education
Table 7 presents percentage distribution of respondents by promotion and level of qualifications. Fifty percent of diplomas holders were promoted and all respondents with bachelor's degrees and master's degrees were all promoted.
Promotion status by of Level of Education (%).

Source: Mwetulundila (2019).
Factors Contributing to Career Progression at MoHSS
Respondents that have been promoted indicated that they were asked to state what they think have qualifications appear to be the most significant contributing variable followed by work experience, skills, hard work, commitment and employees’ dedication to work. “Educational qualification and work experience is very important” as emphasised by a registered nurse.” Respondents also noted that the nursing workforce has witnessed a number of nurses pursuing studies and other trainings to advance their educational backgrounds which is argued to be instrumental toward career advancement. An enrolled nurse narrated that “MoHSS has bridging course encouraging enrolled nurses to study further to become registered nurses.” Other training programs include specializing into cardiac, therapy and midwife among others.
Proportion of Women to Men in Management at MoHSS
On the structural hierarchy of the two hospitals, nine clinics and one health center in Khomas, the study discovered that both at KIH and WCH which are two biggest hospitals, the top management positions of the control registered nurses are both commanded by females. Second in the hierarchy is the chief registered nurse which at KIH, the incumbent is a female whilst at the WCH is held by a male. The gender composition of the managers at eight clinics and at the health center are held by females. A senior registered nurse argued that “women are leading the leadership roles at MoHSS in nursing only but not at other departments such as human resource, finance etc.”
Socio-Cultural and Structural Factors Impeding Career Progression at MoHSS
Respondents indicated that there are few factors affecting women career's progression. However, it was discovered that organizational structure appears to affect career progression of both male and female nurses. Thirty-eight percent of the respondents indicated that human resources policies do not affect women career progression in any way. Moreover, 27 percent of the respondents stressed that there are several social and cultural factors that are present in the institution's structures that affect women career advancement. “Lack of confidence within women themselves who culturally believe that they must know their place in society asserted one of the respondents; women are socialised to believe they should not grab opportunities, opportunities are for men and a lot of women cannot even speak in a meetings to date” asserted by a senior registered. The study further revealed that not all nurses are aspiring to advance in their careers particularly registered nurses due to economic reasons. For example registered nurses are entitled to work overtime and “if you get promoted this benefit is no more applicable to you” as argued by a registered nurse, hence some nurses do not want to leave this position. Lastly, a handful number of female nurses were quick to indicated that family responsibilities such as child bearing, caring of the sick and other reproductive roles are time consuming for women that sometimes necessitate the delay in their career progression compared to their male counterparts when opportunities arises.
Sixty-three percent of respondents indicated that organizational structure plays a significant role impeding employees’ career advancement. In 2013, the MoHSS restructured its organogram to Job Evaluation Grading which resulted in the dissolution and merge of various positions. Through this new structure, nurses stated that career progression at the MoHSS becomes very narrow.
Another structural barrier impeding career progression is; registered nurses at clinics find it difficult to progress to a position of senior registered nurse because such designation is only available at two big hospitals. The primary focus of the two settings vary as the hospitals deals with curative whereas, clinics deals with primary health care which are preventive in nature. Registered nurses with aspirations to advance to senior registered nurses find it difficult because when high positions occur at the hospitals, the interview questions usually focus on curative measures, a component which is non-existent at the clinics.
Family Oriented and Gender Sensitive Human Resource Policies
A total of 95 percent of the respondents have indicated that human resource policies at MoHSS are family oriented. “Women are offered three months maternity leave and there is also a provision for breastfeeding mothers to have an extended lunch for an hour. In the past, there was also what was called ‘mother-baby friendly corner’, however, due to limited spaces at workplace, it was stopped” stated by a senior registered nurse. Other friendly policies include; sick leave, an annual vacation leave for 25 days, compassionate leave for 10 days, study leave, medical aid and pension that employees are entitled to as per Public Service Commission (PSC) regulations. Like any other government institution, MoHSS human resources made provisions for housing subsidies for staff members to acquire houses and the ministry also considers matters such as cross transfer. However, five percent of the nurses described the human resources policy as not family friendly because it does not make provision for paternity leave when one's partner gives birth, the father is not given sufficient time to support the mother and the baby.
Findings further revealed that 81 percent of the nurses indicate that human resources policies are gender sensitive because there are provisions that encourage women to apply for high positions. For example the when a vacant position is advertised there are emphasis made for women to apply when they meet the requirements as provided by the AA Act of 2008. The human resources also provides a trustworthy environment to employees to report all sorts of issue affecting them in the workplace and their social life in general. Thus, many respondents maintained that the policies are non-discriminatory in nature, hence both men and women are equally free to report grievances through the institutionalized modus operandi.
Discussion
Interpretation of the Findings
This study concurred with the conventional belief that nursing profession is a female realm. According to the statistics provided by MoHSS human resources department indicate that Khomas region has about 1177 nurses in total of which 70 percent are females. This is in relation to what other scholars have found. For instance Landau and Henle (n.d) argued that men continue to be a minority in the nursing profession although a small increases in their representation have occurred in the last years. In the same vein, O’Connor (2015) posit that nursing profession across the Western world women outnumber men by a ratio of 10 to 1. The profession is often seen as being synonymous with being female and with femininity. However, the study disputed the conservative conception by various scholars who posit that despite women being dominant in the nursing profession, they often experience suppression from metaphors such as the sticky floor and the glass ceiling in work places. McIntosh (2010) stressed that generally women in nursing are less successful in their careers in comparison to their male colleagues. Also augmenting the same conception Lapierre and Zimmerman (2012) argued that that even in a female-dominated profession, women continue to struggle to receive equitable representation in senior management positions. However in contrary, the study findings contested the status quo whereby it is revealed that women at MoHSS are ones on top of the hierarchal ladder. On the hierarchical structures of the two hospitals, nine clinics and one health center, it was discovered that both at KIH and WCH, the highest management positions of the control registered nurses are commanded by females respectively. Second in the hierarchy is the chief registered nurse which at KIH, the incumbent is a female whilst at the WCH the position is held by a male. Furthermore, the study discovered that the gender composition of the managers at eight clinics and one health center are held by female registered nurses.
In the contemporary world, women are breaking the glass ceiling and achieving targets, where many believed that these targets could only be achieved by men (Sachinthana & Hapurugala, 2019, p.23). In Namibia this could attributed to post independence policies that were effected as impetus for redressing past imbalances and amongst others, focused on subject of gender equity. One of the policies formulated to reverse the phenomena through legal realm was the adoption of the AA Act. In the Namibian context, this legislation intends to foster fair employment practices to the previously racially disadvantaged people, women and persons with disabilities, referred to as the designated group in the Act (EEC, 2002). Other laws and legislation include; the Constitution of Namibia, ratification of CEDAW and the National Gender Policy. The enactment of such legislations and the designing of such policies can be attributed to liberal feminism within the political structures.
Karamat (2016) stressed that marriage remains an important institution which lays the foundation of a family which is the bedrock of a society. The study findings reported that marital status of majority of the interviewed nurses were reported to be never married (68.2 percent). As to Karamat (2016), analysts and policymakers increasingly acknowledge the negative impacts of early marriage in developing countries, one of which is that, it limits women's opportunities for education and skills development. However this study could not validate as two why so many women are delaying marriage in the nursing profession although Karamat (2016) further stressed that delayed marriage ensures marital stability, enables a quality partner and allow people to show more maturity in marriage.
Education is one of the key determinants of several socio-economic aspects. The results shows that 45.4 percent of participants have diplomas, whilst, 27.3 percent have certificates, 18.2 percent have bachelor degrees and the remaining 9 percent had obtained master degrees. This implies that MoHSS nursing workforce is knowledgeable as it is comprised of more diploma holders. This is so because it has be noted that government has been sending certificate holders to institutions of higher learning to attain the diplomas which will be an impetus toward career advancement and progression. The findings also illustrate that there is a correlation between education and career progression as all masters’ degrees holders interviewed were promoted and also most degree holders have been promoted as opposed to those holding diplomas and none of the certificate holders has been promoted.
There seem to be a correlation between career progression and years of employment. This is demonstrated by the fact that those nurses who have been in service at MoHSS for 19 years and more are dominant in managerial designations. The study also reported that more than half of the female nurses (53.3) have been promoted. This status quo is disputing the notion as argued by Njiru (2013) that the pattern holds even for women predominated fields such as nursing or elementary school teaching, where men move more quickly than women into administrative and leadership positions.
Literature evidenced that most societies are still patriarchal and social structures intersect with gender and may have an influence on women's career mobility. Carbajal (2018) argued that many writings shows that leadership has been gendered whereby women in leadership encounter their gender's social context. The effect of gender bias diminishes the quality of leadership for women, i.e., women's worth is perceived based on their gender rather than on their leadership qualities. Namibia is not spared from this phenomenon as argued by Ambunda and de Klerk (2008) that until Namibia gained its independence, its society was deeply patriarchal. However, since the advent of the Namibian Constitution in 1990, there has been a paradigm shift in human rights concepts. The rigid gender roles imposed by the patriarchal society gradually began to change. The AA Act of 1998 was passed which enabled women to enter the job market freely and ascend to managerial roles. This legislation fostered fair employment practices with regard to recruitment, selection, appointment, promotion, and equitable remuneration of previously disadvantaged persons. More specifically, previously disadvantaged persons such as women and persons with disabilities were referred to as the designated group (EEC, 2002).
Promoted respondents maintained that qualifications appear to be the most significant contributing variable to promotions followed by work experience, skills, hard work, commitment and employees’ dedication to work. The AA Act is also instrumental because during vacancies advertisement it is clearly indicated that qualified women and people with disabilities are encouraged to apply and it seem that MoHSS’ human resources directorate has mainstreamed gender in its employment policy.
Socio-cultural factors including gender has less impacts on career advancement, however it was noted that despite women taking over managerial roles challenges such as advancing agenda on issues affecting fellow women when in boardrooms still surface which can be an aftermath of women socialization in a patriarchal society; i.e. women must know their place in society and do not talk in presence of men. This coincides with Singh (2016) argument that parents play an important part in this process of gender awareness. Right from infancy, boys and girls are taught gender specific behavior. Girls are taught to be obedient, submissive, tolerant and generous. Thus, the upbringing was related to the gender roles that boys and girls would take up as adults. Whereas boys are taught to be aggressive, dominating, adventurous and outspoken. The main impediment towards career advancement at MoHSS in nursing was found to be systematic within the institution's organigram and affect both male and females nurses.
Strengths and Limitations
Some limitations identified in this study were the use of one setting confined to Khomas region only hence, it is recommended for a national study. The strengths of this study is that it provide an insight into the body of knowledge relating to gender equity and impedes of career progression in the nursing force.
Conclusion
The study concluded that to date, nursing in Namibia, like many other countries in the world has not shown equilibrium of the genders. Women remain the large majority of staff, whereas men continue to represent only a very small minority. However, the study disputed the conventional assertion that despite women being dominant in nursing profession, they are often impeded in accessing managerial roles by cultural factors and metaphors such as the sticky floor and the glass ceiling in the workplace that prevent them ascending in their careers. The main impediment to career progression is found to be systematic, a policy attribute that affect both genders equally.
Footnotes
Acknowledgments
No acknowledgements.
Conflict of Interests
We declare that there is no conflict of interest.
Funding
Authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
We declare that an ethical statement is not applicable as this manuscript does not involve human or animal research.
CORRECTION (January 2023):
This article was updated to provide clearer attribution to some of the sources.