
Abstract
Introduction
Loneliness is a prevalent problem for adult stroke survivors, and a known contributor to hypertension, secondary stroke, functional decline, poorer quality of life, and mortality in older adults. LISTEN (Loneliness Intervention using Story Theory to Enhance Nursing-sensitive outcomes), a theoretically based behavioral health intervention designed to target loneliness, in a sample of lonely survivors of ischemic stroke.
Keywords
Introduction/Background
Approximately 1/3 of adults who suffer stroke concurrently struggle with depression (Benjamin et al., 2019) or loneliness (Theeke et al., 2014). Loneliness is a unique psychological construct known to increase risk for depression (Cacioppo et al., 2006), cardiovascular illnesses (Bhatti & Haq, 2017), stroke (Brown et al., 2018), second stroke (Valtorta et al., 2016), and acute myocardial infarction (Hakulinen et al., 2018). In a recent literature review of loneliness and chronic conditions, 9 of 10 studies comparing stroke survivors to controls concluded that stroke survivors reported more depressive symptoms and loneliness (Petitte et al., 2015).
There is a lack of well-described interventions for loneliness that have been evaluated for translation to clinical practice. Reviews and a meta-analysis of interventions delivered for loneliness recommended that interventions for loneliness should incorporate a solid theoretical base, strategies to target the maladaptive thinking of loneliness, and group delivery methods (Masi et al., 2011). LISTEN (Loneliness Intervention using Story Theory (Liehr & Smith, 2008) to Enhance Nursing-sensitive outcomes), was developed (Theeke & Mallow, 2015) using the process for complex interventions recommended by the Medical Research Council (MRC) (Craig et al., 2013) for the purpose of targeting loneliness.
The LISTEN Intervention
The conceptual basis of LISTEN is framed using both story theory (Liehr & Smith, 2008) and principles of cognitive restructuring (Sharpe et al., 2012). LISTEN was originally designed to be delivered in group sessions to lonely people, aiming to help people with loneliness reframe problematic thoughts associated with loneliness. Participants of LISTEN attend five sequential 2 hour sessions; each beginning with writing (recording for those that cannot write), followed by exploration of five topics designed to facilitate the transition from thinking about loneliness as insurmountable to a mindset of meaningfulness and solutions. LISTEN has previously demonstrated effectiveness for diminishing loneliness and systolic blood pressure in older adults with chronic illness (Theeke et al., 2016).
Based on the results of the first trial of LISTEN, it was determined that LISTEN has potential effectiveness for diminishing loneliness in survivors of stroke (Theeke et al., 2015, 2016). The overall purpose of this project was to assess the feasibility, acceptability, and initial efficacy of LISTEN on loneliness, depressive symptoms, neurological quality of life, and blood pressure in a sample of lonely survivors of ischemic stroke.
Methods
Design
A longitudinal, non-randomized one group design was employed to accomplish the study purpose.
Research Question
The Research Questions for this study was twofold: 1) What is the feasibility and acceptability of implementing LISTEN for loneliness in a sample of lonely survivors of ischemic stroke? and, 2) What is the initial efficacy of LISTEN on loneliness in lonely survivors of ischemic stroke? The study had two specific aims with corresponding benchmarks for aim 1 and corresponding hypotheses for aim 2 as follows:
Aim 1
Assess the feasibility and acceptability of implementing LISTEN in a sample of adult survivors of ischemic stroke who are experiencing loneliness. The study team considered the following benchmarks of success: (1) Successful recruitment and enrollment of 20 participants within the first three months, (2)Retention of nineteen participants who would attend all five sessions of LISTEN, (3) Positive feasibility evaluations by members of the clinical team, and (4) Participants rating LISTEN as acceptable therapy for diminishing loneliness.
Aim 2
Assess the initial efficacy of LISTEN for loneliness in a sample of adult survivors of ischemic stroke. For Aim 2, we tested the following hypothesis:
H1 Participants will report less loneliness, fewer depressive symptoms, enhanced quality of life and will measure lower on systolic blood pressure for within group and within person baseline values.
Sample and Setting
Potential participants were recruited from people who had been discharged from the hospital with a diagnosis of stroke [based on the International Classification of Diseases, Ninth Revision (ICD-9) codes] within the prior 2 years of the study, and who were currently scheduled for ongoing follow-up care at the neurology clinic between July 1, 2016 and January 1, 2017. The clinic was located in Morgantown, West Virginia. Recruitment methods included posters and flyers in the neurology clinic. The sampling goal was for 20 participants. The study took place in the clinical trials research unit (CTRU) located in the West Virginia University Neurosciences Institute. This setting was accessible by public transportation, offered parking and accessibility entrances for people with disabilities.
Inclusion/Exclusion criteria
Interested participants were screened to meet the inclusion criteria of aged 21 or older, loneliness score ≥ 40 on UCLA Loneliness Scale, English-speaking, and able to answer questions without proxy (in person and by telephone). Participants with cognitive impairment (MMSE ≤ 23), loss of spouse within 2 years (to control for grief reaction), illness), or institutional living situation were excluded. The study took place in the clinical trials research unit (CTRU) located in the university Neurosciences Institute, which offered accessibility for persons with disabilities. Informed consent was sought after establishing that potential participants met the initial basic inclusion criteria and it was required for participation. All study participants signed informed consent prior to participating.
Institutional Review Board Approval
Prior to beginning the study, a letter of approval (protocol 1509861611) was obtained from the West Virginia University institutional review board.
Enrollment and Data Collection Procedures
After meeting inclusion criteria, participants were enrolled and initial pre-intervention (Time 0) data was collected. Subsequent to enrollment, LISTEN groups were conducted weekly for 5 weeks with participants enrolling and participating in LISTEN groups and data collection from January 1, 2017 through April 30, 2017. The LISTEN sessions were delivered by a registered nurse and all sessions were audio and videotaped. Participants received a $50.00 gift card after completion of data collection at each of four data collection time points (enrollment, 1, 6, & 12 weeks post intervention). Feasibility data was collected 1 week after the final LISTEN session from members of the research team and participants, and acceptability data was collected at data collection time 3 (12 weeks post last LISTEN session) from study participants. The taped sessions were reviewed to assure fidelity to the intervention.
Study Measures
Feasibility and Acceptability
Feasibility data was collected using multi-item Likert surveys and field notes to track responsiveness to advertisements, enrollment, retention, attrition, and missed intervention sessions. Acceptability data was collected on multi-item Likert surveys and responses to open ended questions about the structure and delivery of the intervention.
Descriptive Person Factors
Sociodemographics
Study participants self-reported age in years at time of enrollment, gender, ethnicity, marital status, highest education completed, number of people living in home, annual household income, current employment status, county of residence, duration residing in county, and time to travel to university facility.
Mental Status
Participants completed the Folstein mini-mental status exam at enrollment to verify eligibility for inclusion into the study. (Folstein et al., 1975)
Stroke Recovery Information
Date of stroke, days in hospital, post-stroke use of rehabilitation facility, post-stroke use of nursing home, post-stroke use of stroke support group, current use of caregiver, caregiver relationship, and use of paid caregiver.
Social Support
The Medical Outcomes Survey for Social Support (Cronbach’s alpha = .97) was used. This scale includes five subscales: Emotional support, tangible support, affectionate support, positive social interaction, and one additional item for social partner. (Sherbourne & Stewart, 1991).
Activities of Daily Living
The Katz Index of Independence in Activities of Daily Living instrument was used to measure functional ability. (Katz et al., 1970) This scale relies on self-reported abilities for basic (6 questions) and instrumental (10 questions) tasks required for independent living including: hygiene, ambulation, elimination, communication, household management, medicine management, and money management. The scale has been reported as both reliable and valid (Cronbach’s alpha = 0.94). (Wallace & Shelkey, 2008) Scores on the IADL range from 10-30 with 10 indicating no assistance needed. Scores on the Basic ADL instrument range from 6-18 with a score of 6 indicating no assistance needed.
Chronic Illness Information
Diagnoses of comorbid chronic conditions were self-reported by study participants.
Structure of the LISTEN Intervention
LISTEN©(Theeke, 2020) reflects a precision health approach to healing loneliness Participants of LISTEN attended five 2-hour sequential weekly group sessions with 3-5 lonely adults who had also suffered stroke within the past two years. Each session includes writing (recording for those who cannot write), group reflection on weekly topics, and homework for the first four sessions. The first session begins with a focus on the need for belonging, and subsequent sessions emphasize relationships, place in community, addressing challenges of loneliness, and exploring what might remedy each individual’s personal experience of loneliness. Specific information about LISTEN (version 2) is available through listenforloneliness.com.
Study Outcome Measures
Loneliness
Loneliness was measured using the revised 20-item UCLA Loneliness scale (UCLS) which includes 20 items with Likert scale answers that range from Never (1) to Always (4) for summed scores that range from 20-80 (Cronbach’s alpha =0.96). (Russell et al., 1978)
Depression
Depressive symptoms were operationalized using the Patient Health Questionaire-9 which includes 9 questions with 4 point Likert scale answers ranging from not at all (0) to nearly every day (3) for a range of scores from 0 to 27. (Wu et al., 2019) The PHQ-9 has been established to be reliable and valid as a screening tool for major depression in primary care. (Arroll et al., 2010)
Health-Related Quality of Life
The Neuro-QoL was used to operationalize quality of life. This scale includes 13 short forms that measure ability to participate in social roles and activities, anxiety, applied cognition (executive and general), depression, emotional and behavioral dyscontrol, fatigue, lower extremity function, positive affect and wellbeing, satisfaction with social roles and activities, sleep disturbance, stigma, and upper extremity function. The tool has demonstrated reliability, internal consistency, and validity. (Cella et al., 2012; Gershon et al., 2012)
Physical Health Measures
Blood pressure was measured using a calibrated sphygmomanometer.
Data Analysis
Data were analyzed using Statistical Package for Social Sciences (SPSS) version 26.0. Prior to analysis, data were cleaned, seeking outliers, impossible, or missing values. Analysis included data exploration of variables for descriptive information. To assess benchmarks, a process evaluation, field notes, and summed evaluations were critically reviewed. To test initial efficacy repeated measures ANOVA and paired t-tests were used to compare within-subject changes at the four data collection time points in loneliness, depression, health related quality of life, and blood pressure. Alpha level for significance was set at 0.10 which is consistent for a pilot study with a small sample.
Results
Sample Description
Table 1 reports sociodemographic information for participants who had all suffered stroke within the 2 years prior to enrollment. There were no gender differences on mean loneliness scores at baseline and neither age nor depressive symptoms correlated with baseline loneliness scores. Five participants were discharged to home after stroke, and one to a rehabilitation facility and nursing home prior to returning home. Participants reported a median of 14 days in hospital (Range 5-55 days). Three participants had comorbid hypertension, two reported diabetes, and one suffered arthritis. At enrollment, mean mini-mental status scores were 29.3 (SD 1.03) indicating normalcy. None were currently attending stroke support groups, diagnosed with depression or anxiety.
Sociodemographics [Mean Age 57 (SD 6.23), 5 Caucasian].

Note. SD = standard deviation, Totals may not exactly be 100 percent due to rounding.
Participants averaged a 21 minute (SD 14.14) commute to the clinic. One participant reported caregiver needs as provided by spouse and none were privately paying for caregiving. Participants averaged 14.5 (SD 3.67) on Instrumental activities of Daily Living (IADL) which indicates mild limitations with transportation, grocery shopping, and phone use. Participants were nearly independent with basic activities of daily living such as bathing with a mean score of 6.5 (SD 1.22).
In general, participants reported moderate emotional support with a mean of 19.3 (SD 5.4, scale range 7-35). Participants reported low tangible support (mean = 10.33, SD 5.2, range 4-20), low affective support (mean = 6.0, SD 2.8, range 3-15), and low positive social support (mean = 8.3, SD 3.2, range 3-15. When asked if they had someone to do things with (the last question on the social support survey), two participants reported never, 2 reported a little of the time, and 2 reported some of the time.
Feasibility and Acceptability
Recruitment was slow and the desired sample of 20 participants was not achieved. Thirteen inquires resulted in 7 enrollees with one enrollee dropping out after the first session. The six participants traveled by car or the university personal rapid transit system for study sessions. Three participants missed one session each due to illness. Research team members evaluated LISTEN as feasible to deliver in a clinical setting.
All participants rated LISTEN as highly useful, organized, and clear. Homework assignments were rated as highly useful and length of sessions, number of people in groups, time of day for meetings, and number of meetings were rated as appropriate. The environment was rated as hospitable and the overall experience was rated as excellent. Participants reported comfort with video recording the LISTEN sessions. Participants described LISTEN interventionists as understanding, sympathetic, empathetic, open, honest, down-to-earth, knowledgeable, and compassionate. Two participants described personal difficulty with speaking and person difficulty with trying something new as a potential barrier to participation
Initial Efficacy
Mean loneliness scores at enrollment were very high (mean 54.5, SD 5.08). In repeated measures comparisons of mean loneliness scores at baseline and 1,6, and 12 weeks post last LISTEN session, within subject loneliness scores did not change significantly [F (3, 15) = 2.028, p = .15, partial eta2 = .289]. However, in paired t testing, mean loneliness scores from enrollment to 12 weeks post-LISTEN changed significantly (t = 2.04, p = .09). In addition, mean loneliness changed significantly (t = 2.744, p = .04) from1 week post last LISTEN session (mean 57.17, SD 6.24) to12 weeks post last LISTEN session (mean = 51.83, SD 3.43) indicating participants continued to become less lonely.
Mean depression scores indicated moderate depressive symptoms at enrollment with mean scores of 11.83 (SD 4.21). In repeated measures testing, mean depression scores did diminish to a score of 8.5 (SD 3.8) but this change was not significant. In paired t-tests, mean PHQ-9 scores diminished significantly from 6-12 weeks post LISTEN (t = 2.52, p = .053).
Participants improved on three subscales of the Neuro-QoL. On applied cognition - executive function, participants reported less difficulty with executive function [F (3, 15) = 2.848, p = .07, partial eta2 = .363]. Participants reported enhanced positive affect and well-being [F (3, 15) = 3.156, p = .056, partial eta2 = .387] which indicates improvement on concepts such as hopefulness, purpose, meaning, balance, and life worth living. Finally, satisfaction with social roles steadily improved [F (3, 15) = 3.889, p = .031, partial eta2 = .437] (see Figure 1).
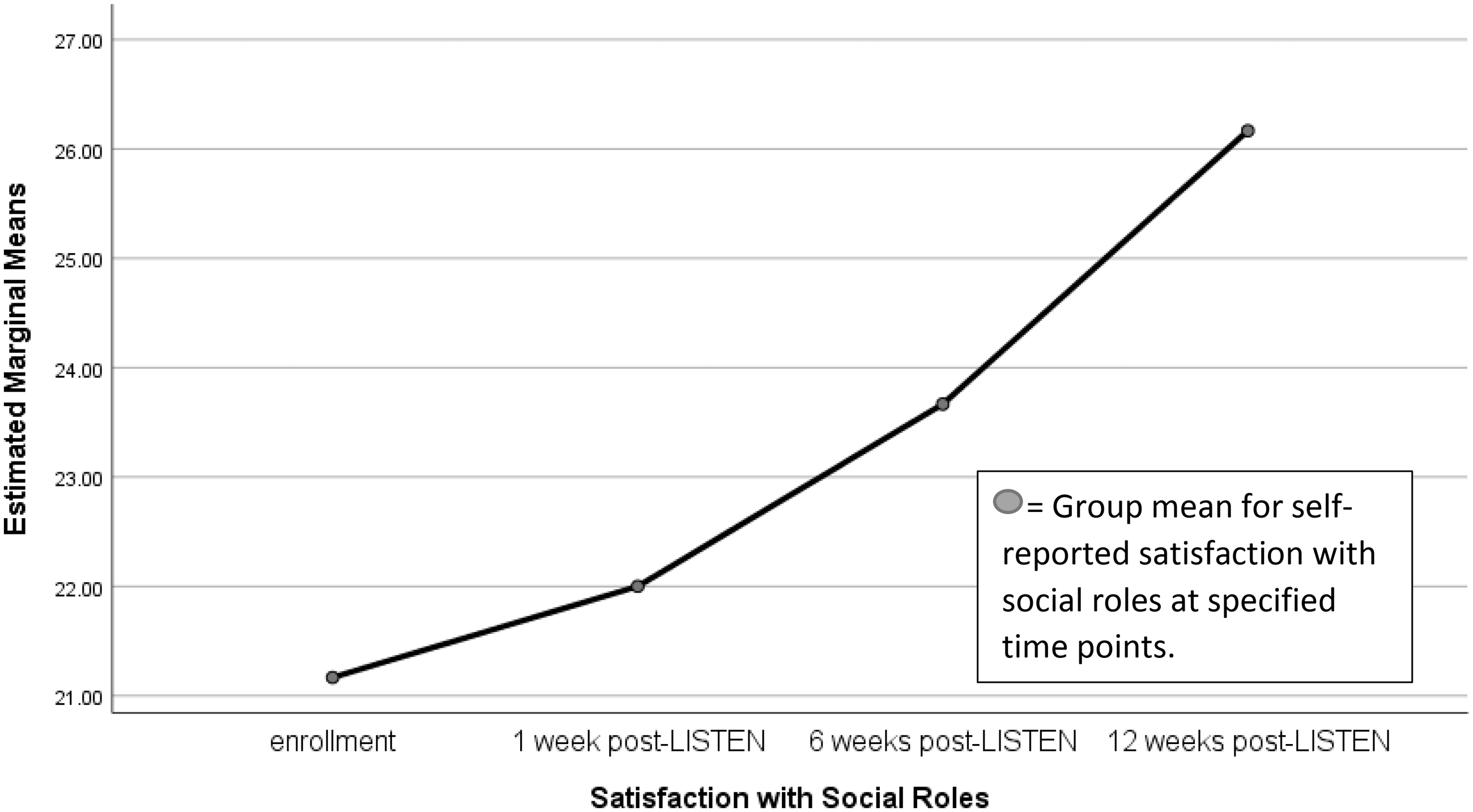
Mean Scores on Satisfaction With Social Roles.
Repeated measures within subject analysis did not show significant decrease in systolic blood pressure [F (3, 15) = 2.207, p = .130, partial eta2 = .306]. However, mean systolic blood pressure decreased from an average of 149 (SD 30.62) to a mean of 135 (SD 19.86) which is clinically relevant in stroke survivors.
Discussion
Study findings elucidate difficulties with recruiting stroke survivors for this type of intervention in Appalachia. The study team has demonstrated cultural competence for recruiting persons with common chronic conditions such as diabetes in Appalachia (Carpenter & Theeke, 2018) so the recruitment difficulties demand new strategies for recruiting stroke survivors.
The positive feasibility evaluations and high acceptability of LISTEN was consistent with the first pilot of LISTEN (Theeke et al., 2015). The efficacious nature of LISTEN provides further evidence that LISTEN is successful as an intervention that targets loneliness (Theeke et al., 2016). LISTEN is rooted in theoretical concepts from story theory (Liehr & Smith, 2008) which likely contributes to its effectiveness as LISTEN honors the individual person’s narratives of loneliness.
The high loneliness score of these stroke survivors who concurrently reported relatively low depressive symptoms indicates that it may be important to screen stroke survivors for loneliness. A prior study of 121 stroke survivors in Appalachia indicated similar results with high loneliness scores (Theeke et al., 2014). Knowing that loneliness predicts depression (Wang et al., 2018) makes it logical to infer that addressing loneliness may be one way to prevent the onset of major depression in this population.
For persons who have survived stroke, controlling blood pressure is paramount to the prevention of second stroke. This is the second pilot of LISTEN that has demonstrated a decline in systolic blood pressure which may be an indicator that addressing the problem of loneliness is diminishing the physiological stress response to loneliness and, thereby, contributing to diminished systolic blood pressure. These findings are consistent with the recent review that reported that higher loneliness scores were associated with both higher blood pressure and a reactive inflammatory response (Brown et al., 2018). It is clinically meaningful that the systolic blood pressure at the final study endpoint had diminished to a mean value less than 140 mmHg, as this is the current clinical goal for adequate blood pressure control for persons with acute stroke. (Whelton et al., 2018)
Strengths and Limitations
The small sample size is a significant limitation to the study and diminishes the ability to generalize the study findings.
Implications for Practice
It is important for nurses to consider loneliness, and screen for it when caring for stroke survivors who are struggling with the sequelae of stroke. The three item UCLA loneliness scale could serve as an effective tool for screening in the clinical settings (Hughes et al., 2004). Recognizing and including loneliness in care planning will be the first step for clinical bedside nurses.
Conclusions
Larger randomized trials or comparative effectiveness trials of LISTEN and other interventions for loneliness would provide evidence regarding the longer term effectiveness of LISTEN on loneliness, depressive symptoms, and quality of life. This project is of translational significance because it establishes feasibility, acceptability, and initial efficacy of LISTEN, an intervention for loneliness, that could be implementable in clinical care of survivors of ischemic stroke who suffer loneliness.
Footnotes
Authors’ note
Laurie A. Theeke was inducted last year as a fellow in the American academy of Nursing.
Author Contributions
L. Theeke, J. Mallow, and E. Theeke participated in study conception and design, intervention delivery, data collection, data analysis and interpretation, drafting the article, and revising the article. L. Theeke finalized the manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research reported in this publication was supported by the National Institute of General Medical Sciences of the National Institutes of Health under Award Number 1U54GM104942-01. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.