
Abstract
Limited information exists regarding the natural development of loneliness and its determinants among cognitively intact nursing home residents. We aimed to examine loneliness among nursing home residents by following up for 6 years and to determine whether sociodemographic factors, diagnosis of cancer, sense of coherence, social support, and depression symptoms influence loneliness. The study was longitudinal and prospective and included baseline assessment and 6-year follow-up. After baseline assessment of 227 cognitively intact nursing home residents (Clinical Dementia Rating score ≤0.5), 52 respondents were interviewed a second time at the 5-year follow-up and 18 respondents a third time at the 6-year follow-up. Data from the interviews were recorded using a global question of loneliness, the Social Provisions Scale, Sense of Coherence Scale, and Geriatric Depression Scale. Scores on Groll’s index (p = .02) and the Sense of Coherence Scale (p = .04) were positively correlated with loneliness and negatively correlated with geriatric depression (p = .001). Having a diagnosis of cancer, social support, and age were not correlated with loneliness 6 years from baseline. Loneliness did not change during the 6 years of follow-up, and symptoms of depression and the sense of coherence appeared to be important components of loneliness. Finally, having a diagnosis of cancer and social support were not associated with loneliness.
Background
Loneliness is an unpleasant feeling (Hauge & Kirkevold, 2010), defined as subjective experiences of a lack of satisfying human relationships (Andersson, 1998) or specific subjective feelings resulting from lack of belongingness (Nicholson, 2009). Older people, independent of cancer diagnosis, are especially vulnerable to loneliness because of age-related changes, losing a partner and losing functional abilities (Deckx, van den Akker, & Buntinx, 2014; Savikko, Routasalo, Tilvis, & Pitkala, 2010; Savikko, Routasalo, Tilvis, Strandberg, & Pitkälä, 2005). The prevalence of loneliness ranges from 39% to 72% (Prieto-Flores, Forjaz, Fernandez-Mayoralas, Rojo-Perez, & Martinez-Martin, 2010; Routasalo, Savikko, Tilvis, Strandberg, & Pitkala, 2006). Loneliness has been shown to be associated with a wide range of adverse conditions such as cognitive decline (Wilson et al., 2007), physical inactivity (Hawkley, Thisted, & Cacioppo, 2009), cardiovascular disease (Christiansen, Larsen, & Lasgaard, 2016), depression (Jansson et al., 2017), mortality (Patterson & Veenstra, 2010), and low quality of life (Gerino, Rolle, Sechi, & Brustia, 2017). The many adverse outcomes of loneliness indicate the importance of taking loneliness seriously. Investigating loneliness over time and the factors that influence loneliness is therefore needed.
Some older people live the last phase of life in nursing homes, which also means losing a familiar environment. This means lack of privacy, lack of freedom, and continuity with their past life and loss of autonomy because of the institutional regimen and regulations, which in turn are related to depression and loneliness (Choi, Ransom, & Wyllie, 2008). In addition, nursing home residents are usually vulnerable and fragile, with a high prevalence of chronic diseases, chronic physical and cognitive functional impairments, multimorbidity, and dementia-related symptoms (Selbaek, Engedal, Benth, & Bergh, 2014); 15% to 26% have a diagnosis of cancer (Drageset, Eide, & Ranhoff, 2012; Gozalo, Plotzke, Mor, Miller, & Teno, 2015). Older people with cancer living in nursing homes represent a growing population with complex care needs (Duncan, Bott, Thompson, & Gajewski, 2009). People experiencing cancer and its treatment often experience loneliness (Deckx et al., 2014), which prevents people from engaging in social activities and interpersonal relationships (Duncan et al., 2009). Our previous research has shown that 57% of nursing home residents with cancer experience loneliness (Drageset, Eide, Dysvik, Furnes, & Hauge, 2015). How nursing home residents with and without cancer cope with these challenges and the ability to adapt to the conditions in nursing homes may vary among individuals.
Research on factors that seem to reduce loneliness is limited (Grenade & Boldy, 2008). Social network support and sense of coherence play a role in preventing loneliness (Fry & Debats, 2002; van Baarsen, 2002). Sense of coherence, the central mental construct of salutogenesis (Antonovsky, 1979), is defined as a global orientation that expresses the extent to which one has a pervasive and enduring, although dynamic, feeling of confidence. This means that stimuli deriving from one’s internal and external environments in the course of living are structured, predictable, and explicable (comprehensibility); that the resources are available to meet the demands posed by these stimuli (manageability); and that these demands are challenges worthy of investment and engagement (meaning). An individual with a strong sense of coherence has the ability to define life events as less stressful (comprehensibility), to mobilize resources to deal with encountered stressors (manageability), and to possess the motivation, desire and commitment to cope (meaningfulness).
The significance of sense of coherence on loneliness, health, and the quality of life has been verified for people in different populations (Eriksson & Lindström, 2007; Tomstad, Dale, Sundsli, Saevareid, & Soderhamn, 2017). Sense of coherence is an important component of better functioning in older age (Takkinen & Ruoppila, 2001), of better health-related quality of life among nursing home residents (Drageset et al., 2009), of well-being and lower scores on depression and of reducing loneliness among older people (Lundman et al., 2010; Tomstad et al., 2017). Changes in mental health after 1 year (Langeland et al., 2006) and sense of coherence as a predictor of health-related quality of life in a 6-year longitudinal study among nursing home residents with and without a cancer diagnosis (Drageset, Eide, & Corbett, 2017) have also been verified.
Social support from family and friends is another important factor that has been shown to reduce loneliness (Luanaigh & Lawlor, 2008). Social support means qualitative aspects such as perceived social support, including the content and availability of relations with other significant people (Sarason, Sarason, & Pierce, 1990). Weiss’ (1974) theory incorporates major elements of most current conceptualizations of social support (Cutrona, Russell, & Rose, 1986). The theory identifies six social provisions: attachment (emotional closeness that gives people a sense of security), social integration (relationships in which people share common interests and concerns), opportunity for nurturance (people taking responsibility for caring for other people), reassurance of worth (people achieving a sense of competence and esteem), reliable alliance (people being able to rely on assistance when they need it), and guidance (advice or information on loneliness or loss). Each provision is associated with a specific type of relationship. Studies have shown that social support influences the health and well-being of older people (Deckx et al., 2014; Drageset et al., 2009; Elovainio & Kivimake, 2000; Routasalo et al., 2006) and loneliness among nursing home residents with cancer (Drageset et al., 2015). Thus, regardless of cancer diagnosis, sense of coherence and social support positively influenced the experience of health and well-being and loneliness among older people (Drageset et al., 2009; Elovainio & Kivimake, 2000; Tomstad et al., 2017).
The results on whether loneliness changes with age have been inconsistent. Victor and Bowling (2012) reported no increase in loneliness in a 8-year study among 999 people 65 years and older living in the community in the United Kingdom. A population-based study in Sweden (Nyqvist, Cattan, Conradsson, Nasman, & Gustafsson, 2017) showed limited changes in loneliness among very old people over 10 years. Luo, Hawkley, Waite, and Cacioppo (2012) reported that the average score on a loneliness scale was quite similar in 2002 and 2004 but increased between 2004 and 2006. The increase may have resulted from the change in the data collection method from in-person interviews in 2004 to self-administered questionnaires in 2006 (Luo et al., 2012). Sociodemographic variables such as sex, age, marital status, and comorbidity have been associated with loneliness among older people (Deckx et al., 2014). Many studies highlight associations between loneliness and symptoms of depression (Luanaigh & Lawlor, 2008). Beyond cross-sectional associations between loneliness and depressive symptoms (Luanaigh & Lawlor, 2008), loneliness leads to increasing depression symptoms in longitudinal studies (Luanaigh & Lawlor, 2008; Nyqvist et al., 2017) and is affected by depression symptoms (Luo et al., 2012). Accordingly, we would expect that depression symptoms are associated with loneliness over time.
A previous study from the same population showed that loneliness was positively associated with the social support subdimension of attachment in a cross-sectional study (Drageset, Kirkevold, & Espehaug, 2011) and the subdimension reassurance of worth in a mixed-methods study among residents with cancer diagnosis (Drageset et al., 2015). As is well known, nursing home residents with and without cancer report symptoms of loneliness (Drageset et al., 2011, 2015) and depression (Choi et al., 2008; Jongenelis et al., 2004; Smalbrugge et al., 2008) and have cancer diagnoses (Drageset et al., 2012; Gozalo et al., 2015). Longitudinal studies of loneliness, sense of coherence, social support and depression with and without cancer are sparse, and studies of this association among nursing home residents are lacking.
This study therefore examined loneliness among nursing home residents over 6 years and whether sociodemographic factors, sense of coherence, social support, and depression symptoms might influence loneliness.
Methods
This study was longitudinal and prospective and part of a study of 227 nursing home residents (60 diagnosed with cancer and 167 not diagnosed with cancer) with no cognitive impairment from 30 nursing homes in Bergen, Norway in 2009 and included follow-up after 5 and 6 years (Drageset et al., 2012). All residents lived in the same nursing homes at follow-up as they did at baseline. The inclusion criteria at baseline (and both follow-ups) were 65 years and older, cognitively intact, capable of conversing, and residing in the nursing home for at least 6 months. We defined cognitively intact as being able to score less than or equal to 0.5 on Clinical Dementia Rating (CDR; Hughes, Berg, Danziger, Coben, & Martin, 1982). The CDR comprises a global score derived from six domains of cognitive and functional performance: memory, orientation, judgment and problem-solving, community affairs, home and hobbies, and personal care. Trained nurses who had observed the residents for 4 weeks or more assessed the CDR scores before including the participants. These nurses were asked to base their CDR scores on how the participants functioned mentally and were requested not to include physical frailty in the scores. The summed domains were calculated according to the instructions (Morris, 1993). Exclusion criteria at baseline and follow-up were resided less than 6 months in a nursing home, CDR > 0.5 and residents whose general health status was evaluated by a physician or nurse, who said that the person could not carry out a conversation with the researcher. The same procedure with CDR was used before the follow-up interviews.
The same principal investigator (JD) who had performed the baseline interviews (n = 227) performed the follow-up interviews among 52 and 18 respondents. In all, 98% (52 of the 53) of those who were alive at the second follow-up and 18 of 19 of those who were alive at the third follow-up participated in the interview. The interview was conducted in the person’s room or at another suitable place in the nursing home. The principal investigator recorded the demographic information and performed the interview, read the questions aloud to the participants, and circled the answer. This was necessary, as many of the residents could not easily hold a pen and had poor vision. Each resident was given a printed questionnaire with large font size so that they could read the questionnaire. The principal investigator made sure that the participants understood all the questions. The participants gave informed consent, including allowing access to their medical records.
Measures
Sociodemographic Variables
Sociodemographic and clinical data such as age, sex, and comorbidity were assessed from the residents’ medical records. We assessed comorbidity using the Functional Comorbidity Index (FCI), a clinically based index (Groll, To, Bombardier, & Wright, 2005) that includes the sum of 18 diagnoses scored 1 for yes and 0 for no, as recommended by Groll et al. (2005). The maximum score of 18 indicates the maximum number of comorbid illnesses. The FCI has been used among nursing home residents (Groll et al., 2005). The FCI does not include cancer diagnosis, so this was obtained separately. The residents with cancer were assigned a score of 1 and the residents without cancer 0. All cancer diagnoses were included, including skin cancer (basal cell carcinoma). Cancer diagnoses were obtained from medical records and include active cancer and previously treated cancer.
Loneliness
Loneliness was assessed by an overall question: Do you sometimes feel lonely?. Studies of older people living in nursing homes (Bondevik & Skogstad, 1996; Drageset et al., 2011) and people living at home (Holmen, Ericsson, Andersson, & Winblad, 1992; Tomstad et al., 2017) have used this question. The responses were scored using response categories of 1 = often, 2 = sometimes, 3 = rarely, and 4 = never. Higher scores on the scale indicated lower loneliness. For the statistical analysis, this variable was dichotomized, with response categories 1 and 2 combined into 0 = lonely and 3 and 4 combined into 1 = not lonely.
Sense of Coherence Scale
Antonovsky’s 13-item Sense of Coherence Scale (SOC-13) was used to estimate the residents’ sense of coherence. The SOC-13 has a 7-point semantic differential scale format with two anchor responses: never and very often. The items measured were perceived comprehensibility (five items), manageability (four items) and meaningfulness (four items). The score ranges from 13 to 91, with a high score indicating a strong sense of coherence. A systematic review of the validity and reliability of the SOC-13 (Eriksson & Lindström, 2005) showed that it is generally acceptable among older people.
Social Support
Social support was assessed by using the revised Social Provisions Scale (SPS; Cutrona & Russell, 1987) through face-to-face interview. The revised SPS thus includes four subscales with four items each: attachment, social integration, nurturance, and reassurance of worth. The items were scored using the response categories 1 = strongly disagree, 2 = disagree, 3 = agree, and 4 = strongly agree, and a total score was calculated. High scores indicate high social provision. The revised SPS has shown good reliability when used among older people living in the community (Bondevik & Skogstad, 1996; Saevareid, Thygesen, Lindstrom, & Nygaard, 2010) and in nursing homes (Bondevik & Skogstad, 1996; Drageset et al., 2011).
Geriatric Depression Scale
We detected depression by using the Geriatric Depression Scale (GDS; Yesavage et al., 1982). The GDS was originally developed as a 30-item instrument but was shortened to 15 of the original 30 items. The short version of the GDS has been found to be reliable and valid among older people in different settings (Lesher & Berryhill, 1994), including nursing homes (Jongenelis et al., 2004; Smalbrugge et al., 2008). In this study, Cronbach’s alpha was .79.
Statistical Analysis
The descriptive statistics used are the mean, range, and standard deviation (SD). Loneliness (dichotomized) was analyzed using logistic regression modeling with generalized estimating equations to account for correlation between repeated follow-ups in the same subjects. The predictor variables were time for interview, age, sex, diagnosis of cancer, FCI, the four SPS subscales, SOC-13, and GDS.
Ethics Approval and Consent to Participate
The Norwegian Social Science Data Services and the Western Norway Regional Committee for Medical and Health Research Ethics approved the study (REK.Vest no. 162.03/2009/1550). The participants gave written informed consent to participate at each interview, which included allowing the researchers to access their medical records.
Results
The mean age of the 52 respondents at the 5-year follow-up was 80 years (range: 65–102), with 72% being women. Of the 18 respondents at the 6-year follow-up, 11 (62%) were women and the mean age was 85 years (SD: 7.6 years). The most common cancer diagnoses were colorectal, breast, and prostate. The type of cancer was not correlated with loneliness (p = .76; Table 1). The mean number of comorbid illnesses at baseline was 1.9 (median: 2.0, SD: 1.3, range: 0–5). In unadjusted analyses, FCI (p = .004), social support subdimensions, attachment and reassurance of worth (p < .001 and p < .001, respectively), and SOC-13 (p < .001) were positively associated with loneliness. GDS was negatively correlated (p < .001; Table 2) from baseline to follow-up. The positive correlation still remained for FCI (p = .02) and for SOC-13 (p = .04) and the negative correlation for GDS (p = .001) in adjusted analysis (Table 2). Having a diagnosis of cancer was not correlated with loneliness over time in either unadjusted (p = .49) or adjusted analysis (p = .59) from baseline to follow-up. Time was not correlated with loneliness from baseline to follow-up.
Personal Characteristics at Inclusion of the 227 Respondents in the Bergen Nursing Home Study 2004 to 2005 According to Loneliness at Inclusion.

Note. FCI = Functional Comorbidity Index.aStudent’s t-test; bChi-square test.
Results from logistic regressions analysis for loneliness using GLM among 227 cognitively intact nursing home residents in Bergen, Norway in 2004-2005 - 6 years of follow-up.
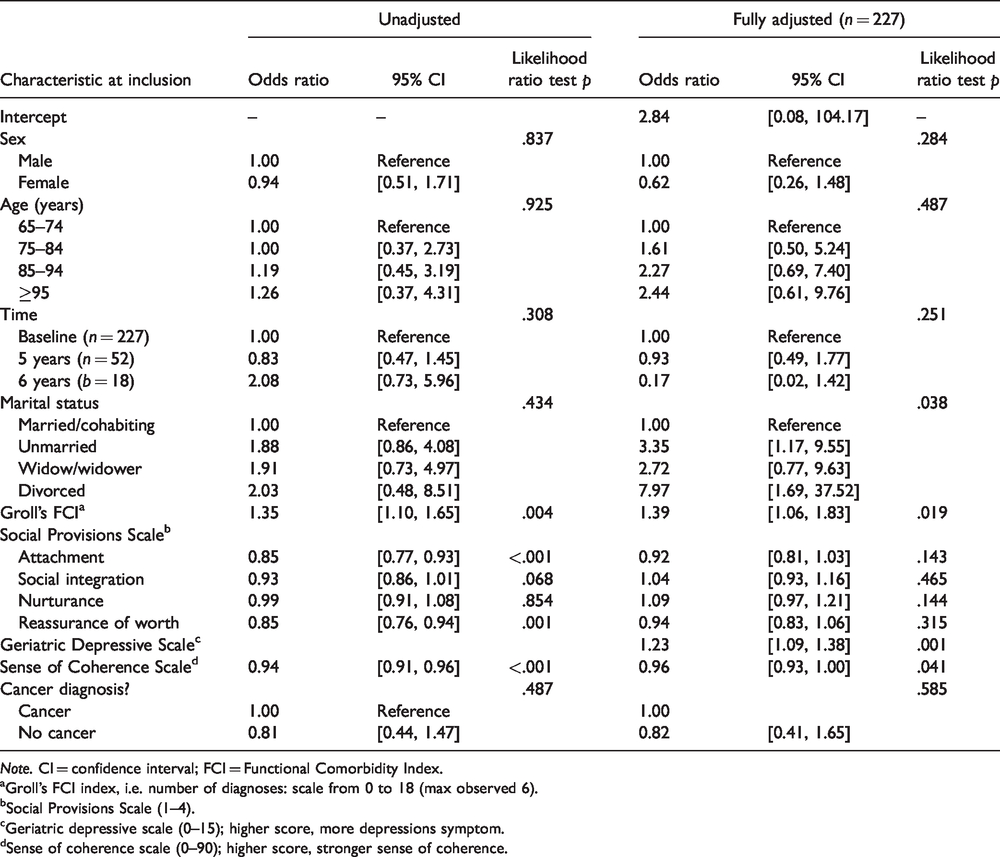
Note. CI = confidence interval; FCI = Functional Comorbidity Index.aGroll's FCI index, i.e. number of diagnoses: scale from 0 to 18 (max observed 6).bSocial Provisions Scale (1–4).cGeriatric depressive scale (0–15); higher score, more depressions symptom.dSense of coherence scale (0–90); higher score, stronger sense of coherence.
Discussion
This study investigated whether loneliness changed over time during a 6-year follow-up period and whether social support subdimensions, sense of coherence, symptoms of depression, and having a diagnosis of cancer influence the experience of loneliness.
In this nursing home study from 2005 to 2011, we found no change over time for loneliness in unadjusted analysis or after adjusting for age, sex, diagnosis of cancer, FCI, SPS, GDS, and SOC-13. Victor and Bowling (2012) also reported no change in time with increased age in an 8-year community-based study among people 65 years and older, as did a population-based 10-year study in Sweden among very old people (Nyqvist et al., 2017). Victor and Bowling (2012) studied different cohorts using different measurement methods, and Nyqvist et al. (2017) studied three cohorts in three different periods. Because of the design in these studies, the association of loneliness over time in the same cohort was not reported.
In accordance with previous research (Andersson, 1998; Cohen-Mansfield, Hazan, Lerman, & Shalom, 2016; Deckx et al., 2014; Luanaigh & Lawlor, 2008), our results showed that marital status is a risk factor for loneliness in adjusted analysis. The highest odds of being lonely were for divorced and unmarried people. A possible explanation may be that nonmarried people (divorced and unmarried) because of loss of partner (Cohen-Mansfield et al., 2016) and close friends have a lack of support in sharing thoughts and feelings (Routasalo et al., 2006), and unmarried people are less likely to have children who give social support.
Similar to a previous study (Luanaigh & Lawlor, 2008), we found that depression symptoms were associated with loneliness. Depressed people probably seek less contact and will thus be more lonely, as loneliness is lack of satisfying human relationships (Andersson, 1998) and belongingness (Nicholson, 2009). However, the relationship between loneliness and depression is complex and likely to be reciprocal (Prieto-Flores et al., 2010), but depression symptoms were associated with loneliness in our 6-year longitudinal study.
However, most importantly, loneliness and depression are common among the oldest people in general (Luanaigh & Lawlor, 2008) and among nursing home residents (Jongenelis et al., 2004; Smalbrugge et al., 2008).
Our longitudinal cohort study demonstrated that SOC-13 was positively correlated with loneliness after adjusting for age, sex, diagnosis of cancer, and FCI. Our findings are in accordance with the studies of the relationship between people’s sense of coherence and loneliness (Eriksson & Lindström, 2007; Tomstad et al., 2017) and with Antonovsky’s (1979) view that sense of coherence is related to health and well-being. Our findings could therefore suggest that residents being able to mobilize the available resources such as social contact to deal with challenges related to everyday life in a nursing home and then experience meaning in doing this may lead to reduced loneliness.
Strength and Limitations
One strength of our study is that it was based on same cohort of older nursing home residents followed for 6 years. Another strength is the high response rates after 5 and 6 years. An additional strength is that all instruments are well validated among older people, including those living in institutions such as nursing homes. No data were missing from the GDS, SPS, and loneliness scale, and very few data were missing from the SOC-13. The respondents did not generally find the questions difficult to answer. Using personal interviews with each individual to collect data on depression symptoms, sense of coherence, SPS, and loneliness ensured qualitatively good data.
However, one limitation is the small sample size, but the sample is unique, and we included 99% of that entire population still alive after 5 and 6 years. In addition, loneliness was measured with a global question that does not distinguish between emotional and social loneliness. Only cognitively intact residents were included, with the result that most residents, who have cognitive impairment, were not included.
Conclusion
This study has three important findings. First, loneliness did not change over time during the 6 years of follow-up. Second, symptoms of depression and the sense of coherence seem to be important components of loneliness. Third, social support dimensions and having a diagnosis of cancer were not associated with loneliness.
Relevance to Clinical Practice
Health-care professionals should recognize that the sense of coherence is associated with loneliness and that strengthening the sense of coherence may reduce the experience of loneliness. Nursing home personnel should therefore observe residents closely for signs of depression and loneliness and facilitate social contacts between the residents and significant others in preventing symptoms of depression and loneliness. Furthermore, identifying residents’ previous strengths and making the residents aware of the resources available help them despite their limitations. In addition, professionals could support residents in engaging in activities in the nursing home they previously valued but had to give up after moving to the nursing home, which in turn may reduce depression symptoms and loneliness. Further studies should consider a larger sample size for studying loneliness and its predictors over time and residents’ own understanding of loneliness to better meet the residents’ needs.
Footnotes
Data Accessibility Statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.