
Abstract
Introduction
Community integration is an essential component for rehabilitation among traumatic brain injury (TBI) survivors, which yields positive outcomes in terms of social activities, community participation, and productive work. A factor that usually facilitates community integration among TBI survivors is social support, whereas physical environment and fatigue are most often found as barriers.
Objectives
This study aimed to (1) describe the level of community integration, fatigue, physical environment, and social support of persons after TBI, and (2) examine the relationship between community integration and these three factors.
Methods
This is a descriptive correlational study. One hundred and twenty TBI survivors living in the communities of Province Number Three, Nepal were enrolled using the stratified sampling technique. The data were collected using the Community Integration Questionnaire, Modified Fatigue Impact Scale, Craig Hospital Inventory of Environmental Factors, and the Multidimensional Scale of Perceived Social Support. Descriptive statistics and Pearson’s correlation were used to analyze the data.
Results
Community integration, fatigue, and physical environment showed a moderate level, while social support revealed a high level. Fatigue was significantly correlated with overall community integration, whereas physical environment was found to correlate with two subscales of community integration, home integration and productive activities.
Conclusion
To enhance the level of community integration among TBI survivors, health care providers, in particular rehabilitation nurses and community nurses, should plan and implement strategies such as follow-up appointments or continued rehabilitation at home.
Globally, more than 50 million people suffer from traumatic brain injury (TBI) each year (Maas et al., 2017). In Nepal, 22% of TBI survivors live with disabilities (Gupta et al., 2015). The most common issues affecting TBI survivors are related to a decrease in participation at home, productive life, social activities as well as community integration (Parvaneh et al., 2014). Community integration (CI) is defined as one’s active participation into three major areas: (1) home integration as an active participation of the individual in the operations of the home; (2) social integration as participation in a variety of activities outside the home, e.g., social events; and (3) productive activities such as employment, and educational and/or volunteer activities (Willer et al., 1993). Previous studies have shown different levels of CI in TBI survivors. A high level of CI has been reported to associate with one’s ability to return to meaningful work, engage in home activities, and receive support from family, friends, and significant others (Forslund et al., 2013; Sandhaug et al., 2015). On the other hand, a low level of CI has been shown to lead to social isolation, reduced participation in daily activities, and low productive activities (Abrahamson et al., 2017; Mollayeva et al., 2015). Hence, the successful CI of TBI survivors depends on favorable factors.
Review of Literature
Factors such as fatigue symptoms, physical environment, and social support are related to the CI of TBI survivors. Fatigue is one of the most common disabling symptoms in such persons (Lequerica et al., 2017). It has a negative impact in their ability to live in the community (Juengst et al., 2017). The physical environment is also a sensitive CI factor in this patient group. The aspects of physical environment like the characteristics of the building, bright or dim lighting, hot or cool weather are associated with a low level of CI in TBI survivors (Fleming et al., 2014; Pappadis et al., 2012). However, the availability of automatic doors and provisions of assistance to access directions and route transit information at a bus station enhance their CI (Lefebvre & Levert, 2014).
Moreover, social support may facilitate their access to interaction with community members (Donker-Cools et al., 2018). The support from family and friends has been found to associate positively with a high level of CI, whereas support from co-workers, employers, and health professionals tends to relate to a low CI level (Donker-Cools et al., 2018; Nichols & Kosciulek, 2014).
In a developed country or Western countries, rehabilitation for TBI survivors includes both inpatient and community rehabilitation, which help them in the process of recovery to integrate into their home, society, and productive activities (Khan et al., 2003). A recent systematic review conducted in low- and middle-income countries identified barriers to rehabilitation such as distance to a health service access point, inaccessibility of transportation, and unaffordability of services (Bright et al., 2018). However, Nepal is a developing country with different in terms of its culture, geography, and availability of the healthcare system services compared to such countries. Nepal consists of a diverse culture with a communal society, and accessibility to healthcare resources is challenging in some parts of the country.
This study was, therefore, conducted to (1) describe the level of CI, fatigue, physical environment, and social support in TBI survivors; and (2) examine the relationship between these factors. Its findings would be helpful in the further development and implementation of nursing interventions that would assist in enhancing the community integration of persons who have suffered from TBI.
Methods
Design
This is a descriptive correlational study.
Research Questions
The research questions are (1) what is the level of community integration, fatigue, physical environment, and social support in TBI survivors? and (2) what is the relationship between these three factors (fatigue, physical environment, and social support) and community integration?
Sample
The participants in this study were TBI survivors that had been discharged from five hospitals and were living in the communities of Province Number Three in Nepal.
The stratified sampling technique was used to select the target sample based on an assumption of a bivariate correlation test (Pearson’s Product Moment Correlation Coefficient) where the power is set at .80 and the alpha value is .05 (Polit & Beck, 2012). Consequently, 120 participants were enrolled in this study.
Inclusion Criteria
The inclusion criteria were: (1) people diagnosed with TBI and living in the community for 6 to 12 months after discharge from hospital/rehabilitation center; (2) 18 years of age or older; (3) able to communicate in and understand the Nepali language; and (4) with a good level of consciousness at the time of the interview indicated by a GCS score of 15. As TBI survivors engage in their home, social, and productive activities from 6 to12 months, the selected duration of living in the community among TBI survivors would be helpful to examine the level of CI, and also the level of barriers from the physical environment.
Individuals with a history of any other condition resulting in progressive cognitive decline (e.g., dementia), a current active psychotic or bipolar disorder, or currently involved in injury-related litigation were excluded.
A stratified random sampling procedure was used for selecting the participants in this study. The stratification was based on five hospitals, one public trauma hospital, one tertiary level hospital for military personnel and their families, and three private neuro hospitals.
Settings
The study was conducted between 2018 and 2019 in the communities of the thirteen districts of Province Number Three in Nepal. In this province, there are five major neuro-trauma hospitals. Of these five hospitals, one is the only public trauma hospital in Nepal, another is the only tertiary level hospital for military personnel and their families, and the other three are renowned private neuro hospitals in Nepal. Only one hospital has a neuro rehabilitation center, whereas the other four hospitals provide rehabilitation services in their outpatient departments (OPDs). Therefore, in those four hospitals, the patient needs to be followed-up in the physiotherapy OPD to receive rehabilitation services.
Measurement Tools
Five instruments were used for data collection: (1) Demographic and Clinical Characteristic Questionnaire, (2) Community Integration Questionnaire (CIQ), (3) Multi-Dimensional Scale of Perceived Social Support (MSPSS) Nepalese version, (4) Craig Hospital Inventory of Environmental Factors (CHIEF), and (5) Modified Fatigue Impact Scale (MFIS).
The CIQ was used to measure CI. It consists of 15 items that measure aspects related to the home environment (5 items) with a score range from 0 to 10, social network (6 items) with a score range from 0 to 12, and productive activities (4 items) with a score range from 0 to 7. The possible scores range from 0 to 29, with a higher score indicates greater integration (Willer et al., 1993). The score was interpreted into three levels (as cited in Gray et al., 2017) as low (0 to 9.67), moderate (9.68 to 19.33) and high (19.34 to 29.0). The CIQ was translated into the Nepali language using the back-translation process proposed by Brislin (as cited in Polit & Beck, 2012).
The MSPSS (Nepalese version) by Tonsing et al. (2012) was used to assess social support. It consists of 12 items related to support from family, friends and significant others. The mean score of MSPSS (Nepalese version) was interpreted as low (1 to 2.9), moderate (3 to 5), and high (5.1 to 7.0).
The CHIEF was used to evaluate environmental factors. Whiteneck et al. (2004) developed the original tool that consists of 25 items, and it is a self-rated questionnaire measuring the environmental barriers encountered by people with disabilities. In this study, the researcher modified the tool after getting permission from the author; it included only six items of the questionnaire describing the physical structure domain, which is appropriate for this study’s variables. The six items include (1) availability of transportation, (2) design of home, (3) design of school or work, (4) design of community, (5) temperature, climate, terrain, and (6) lighting, noise, crowds. A frequency-magnitude score of 0–8 was adopted, with a higher score indicating a greater impact of the environmental barrier. The score of the physical environment was interpreted into three levels (as cited in Gray et al., 2017) as low (0 to 2.67), moderate (2.68 to 5.33), and high (5.34 to 8.0).
The MFIS is a multidimensional scale, which is a modified form of the fatigue-impact scale used to measure fatigue and developed by Fisk et al. (1994). It consists of 21 items measuring domains related to the physical fatigue subscale (9 items) with a score range of 0 to 36, the cognitive fatigue subscale (10 items) with a score range of 0 to 40, and the psychosocial fatigue subscale (2 items) with a score range of 0 to 8. The total score ranges from 0–84, with higher scores indicating greater fatigue. The score of fatigue was interpreted into three levels (as cited in Gray et al., 2017) low (0 to 28.0), moderate (28.1 to 56.0), and high (56.1 to 84.0).
The Cronbach’s alpha coefficient was used to evaluate the internal consistency of each item of the instruments and to estimate the extent to which each item is reliable to measure the intended construct (Polit & Beck, 2012). In this study, the Cronbach's alpha coefficients for the Nepalese version of CIQ, MSPSS, CHIEF, and MFIS were .75, .92, .90, and .93, respectively.
Data Collection
After obtaining ethical approval, the researcher collected detailed information related to TBI survivors that had been discharged from the five hospitals specified above and who were living in the communities of Province Number Three, Nepal.
A brief explanation was provided to the potential participants regarding the objective, purpose, procedure, risk, and benefit of the study via telephone. If the participant agreed to participate, an appointment was made regarding the place and time of the home visit. Most data were collected at home, and some participants were approached at a convenient place.
The researcher asked each eligible participant to sign an informed consent form. If the participant could not sign, the researcher asked his/her family member to sign the informed consent with the agreement of the participant. The participants completed the questionnaires on their own, and for 21 participants who could not do so by themselves, the researcher helped to read and fill the questionnaire on their behalf. It took around one hour for each participant to complete the set of questionnaires. Finally, the completion of the questionnaires was checked.
Statistical Analysis
Descriptive statistics were used to measure the level of CI, social support, physical environment, and fatigue. Pearson’s correlation was used to examine the relationship between CI and factors associated with it after the assumption was met. The level of significance was set at p < .05.
Results
Participant Demographic Characteristics
Of the 120 participants, most of them were aged between 18 and 45 years and had a mean age of 34.46 years. The majority were male (79.2%) and married (71.7%). A motorcycle accident was the most common cause of TBI accounting for 41.7% of cases. Around 75.0% of the participants were working after their TBI. Most of them (82.5%) had mild TBI, followed by moderate-level TBI (15.8%) at discharge from hospital. The highest number of the participants (66.7%) had been injured 6–9 months prior to the study. Approximately 97.0% of the participants were independent regarding their activities of daily living (Table 1).
Frequency and Percentage of the Participants Classified by Demographic and Clinical Characteristics (N = 120).

Level of Community Integration, Fatigue, Physical Environment, and Social Support
The overall CI score of the participants was 15.99 (SD = 3.32), which indicated a moderate level of CI. Based on the mean percentage, the social integration subscale showed a higher level (66.1%) than the subscales of productivity and home integration. The participants experienced a moderate level of fatigue after TBI (M = 49.93, SD = 11.77) and faced a moderate level of barriers (M = 3.16, SD = 1.24). Meanwhile, the social support the participants received was of a high level (M = 5.39, SD = 0.67) (Table 2).
Mean, Standard Deviation, Score Range, Mean Percentage and Level of Community Integration, Fatigue, Physical Environment, and Social Support (N = 120).
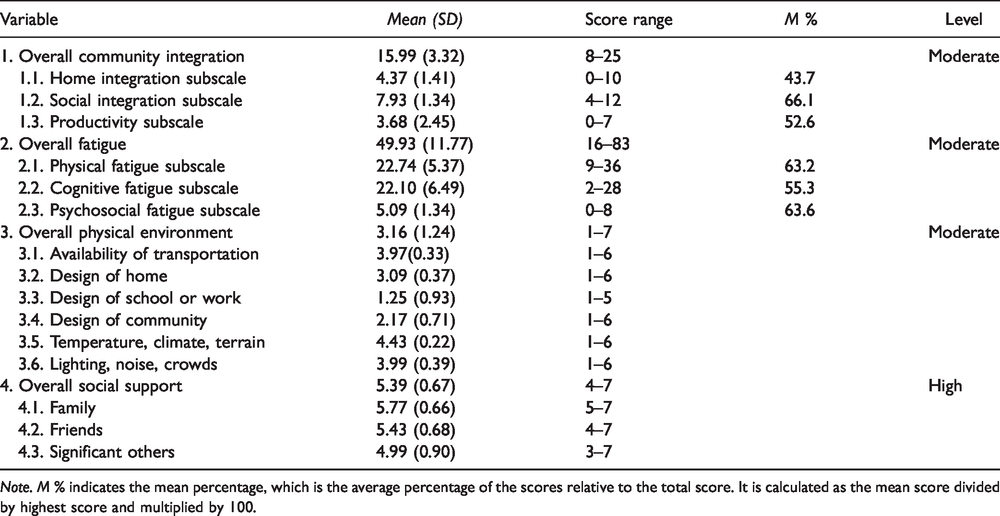
Note. M % indicates the mean percentage, which is the average percentage of the scores relative to the total score. It is calculated as the mean score divided by highest score and multiplied by 100.
Relationship Between Community Integration and Fatigue, Physical Environment, and Social Support
The relationship between the study variables was analyzed using the Pearson correlation. It was found that fatigue had a significant negative relationship with overall CI and its subscales (r = –.31, p < .01). Physical environment showed a significant correlation with the home integration subscale (r = –.19, p < .05) and the productive activities subscale (r = –.19, p < .05). However, social support was not significantly related to CI and its subscales (p > .05) (Table 3).
Pearson Correlation Coefficients of Overall Community Integration and Community Integration Subscales with Fatigue, Physical Environment, and Social Support (N = 120).

**p < .01. *p < .05.
Discussion
Level of Community Integration, Fatigue, Physical Environment, and Social Support
The overall CI among Nepalese survivors of TBI was found at a moderate level, which was similar to the findings of a previous study (Gerber et al., 2016). Predominantly, our participants were male and engaged in independent activities of daily living. The subscale scores for social integration were high. Moreover, the majority of the participants were young adults and were still working, which had a positive influence on their abilities to visit friends or relatives and participate in leisure activities. Out of all age groups, it is a known fact that young adults are the one who engage in social activities such as visiting friends and confiding in their best friends the most (Migliorini et al., 2016). The subscale score regarding productive activities was moderate. Although most of the participants were employed, their participation in volunteer activities was low. This is because, after TBI, they tended to be employed within the home environment and may have felt too fatigued to travel outside to engage in such activities. Furthermore, volunteering is uncommon among people in developing countries (Butt et al., 2015).
The score of the home integration subscale was lower when compared with the other two subscales of CIQ; this is in contrast to the finding of a previous study (Mollayeva et al., 2015). It has to do with the fact that most of our participants were male. In Nepal, men have a higher authority, whereas females are given the responsibility of household activities, and they rely on their husbands for financial support (Pokharel, 2008).
A moderate level of fatigue was perceived by the participants of this study. Fatigue may either be related to neuroendocrine abnormalities from their brain injury or be reported as a long-term problem among TBI survivors. As a result, fatigue in TBI survivors interferes with the person’s ability to perform their daily activities (Cantor et al., 2013). When considering subscale scores, psycho-social fatigue had the highest score as the majority of the participants worked within the home environment and rarely traveled outside the home. The physical fatigue subscale had a moderate score that may have resulted from the presence of concurrent symptoms, e.g., headache (25.4%), anxiety (24.5%), pain (14.0%), depression (3.5%), and sleep disturbance (6.1%), which are common symptoms in mild TBI cases (Donker-Cools et al., 2018; Mollayeva et al., 2015; Stocchetti & Zanier, 2016). The subscale of cognitive fatigue had the lowest score as the majority of the participants indicated low impairment levels in cognitive function. Most of the participants reported a low score for items such as being forgetful, having trouble concentrating, and experiencing a slower ability to think.
A moderate level of barriers from the physical environment was perceived. The majority of the participants after TBI were working within the home environment and rarely ventured outside. This could have reduced the frequency of potential problems caused by the physical environment. Another possible explanation may be the post-discharge period living in the communities. In this study, the participants were living in the communities that constituted the study setting for 6 to 12 months. A previous study found that TBI survivors reported environmental barriers at 1, 3, or 6 months after discharge (Fleming et al., 2014). Most of the participants perceived temperature and climate as big problems. The season during data collection was winter with the temperature ranging from 8°C to 12°C; in some parts, the temperature fell below 3°C, and at times, snowfall was present (Department of Hydrology and Meteorology, 2019).
However, the majority of the participants perceived a high level of social support. In Nepal, family relationships are highly regarded by those living in joint or extended families. Relatives usually support and care for each other whenever there is a sick member in the family (Boreson & Askesjo, 2015).
Relationship Between Community Integration and Fatigue, Physical Environment, and Social Support
A negative significant relationship between fatigue and CI was discovered in persons after TBI. This finding concurs with those of previous studies on persons surviving TBI (Englander et al., 2010; Juengst et al., 2013). Most of the participants reported that they felt weak, less motivated to participate in social activities, and needed to rest more often or for longer periods. Hence, the negative relationship between fatigue and CI in TBI survivors owes its explanation to traveling less, taking rest more often, and being less motivated to participate in social activities.
No significant relationship between the physical environment and CI was observed. This finding goes contrary to those reported by previous studies (Fleming et al., 2014; Wong et al., 2017). Persons with moderate-to-severe TBI have high cognitive impairment compared to mild TBI as it leads to ongoing functional limitation (Fleming et al., 2014). Most of the participants in the study suffered from mild TBI, which could have decreased the frequency of such barriers. Moreover, a few participants had sensory impairments such as hearing and vision loss that could have reduced the frequency of perceived barriers such as lighting, noise, and crowds. The low frequency of items related to physical environment barriers could have led to the findings of the non-significant relationship between physical environment and CI.
Furthermore, no significant relationship between social support and CI was observed. The majority of the participants suffered from mild TBI at discharge, and most of them were able to perform the activities of daily independently. The participants stayed in the hospital for short durations and returned home directly without undergoing any brain-injury rehabilitation. This finding was a clear indication of the Nepalese healthcare system’s unpreparedness regarding rehabilitation practice. However, in Western societies, rehabilitation practice in TBI survivors after discharge from hospital has been shown to motivate TBI survivors to get involved in activities outside the home (Khan et al., 2003).
Due to the contextual differences in research setting, severity of injury, and dependency in performing the activities of daily living, the findings of previous studies and those of this research were contradictory. In Nepal, rehabilitation centers are mostly located in urban areas. There are mainly steep mountains and hills with paved roads in rural areas of Nepal where public transportation are nearly non-existent. Therefore, the TBI survivors living in rural areas of Nepal may spend more than an hour and up to 4 hours for accessibility to rehabilitation centers (Center Bureau of Statistics, 2011). The findings of the present study could provide health policy makers and the Nepalese governmental authorities with useful insight for the development of strategies aimed at enhancing the facilitators of and reducing the barriers to community integration among TBI survivors in Nepal.
Strengths and Limitations
This is the first study conducted in Nepal, which explores community integration among persons after TBI. Its findings have made a significant contribution toward raising awareness regarding this topic among policy makers and health care providers in Nepal as well as informing the provision of better care and services for TBI survivors. However, there is also a limitation to the interpretation of this study’s findings. The study employed only single time-point assessment of CI among TBI survivors living in the communities of province in Nepal. Furthermore, it did not explore any other potential confounding factors related to CI.
Implications for Practice
The study findings showed the moderate level of CI among TBI survivors in Nepal. Therefore, to enhance a higher level of CI, the health care providers, in particular the rehabilitation nurses or community nurses should plan and implement strategies for TBI survivors such as follow-up appointments or continued rehabilitation at home. In addition, it is necessary to provide knowledge and information for TBI survivors in order to manage all types of fatigue after discharge from hospitals or rehabilitation centers.
Conclusions
The study showed a moderate level of CI in persons that have survived TBI and were living in Province Number Three of Nepal. Fatigue showed a significant relationship with CI. This suggests that TBI survivors living in these communities experience fatigue as one of the main barriers to rehabilitation outcomes causing a delay in their return to home, work, and normal community life. It is, therefore, necessary for the healthcare team in hospitals and rehabilitation centers to provide a timely management of fatigue in order to improve rehabilitation outcomes and overcome delays in these patients’ integration in the home, social, and productive activities. A longitudinal study is recommended to determine the predictive factors for CI.
Footnotes
Acknowledgments
The authors would like to express a gratitude to the Higher Education Research Promotion and the Thailand’s Education Hub for Southern Region of ASEAN Countries Project Office of the Higher Education Commission and Prince of Songkla University. The authors are thankful to Annapurna Neurological Institute & Allied Sciences, Dirghayu Guru Hospital and Research Center, National Trauma Center, Shree Birendra Hospital, Upendra Devkota Memorial National Institute of Neurological and Allied Science, and all the participants of the study. In addition, the authors would like to acknowledge for providing permission to use and modify tools based on the context.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to express a gratitude to Prince of Songkla University, Thailand, for the partial financial support in the form of a grant.
Ethical Considerations
This study was approved by the Center for Social and Behavioral Sciences Institutional Review Board at the university (IRB 2018-Nst 050), the Nepal Health Research Council (Reg. No.777/2018), and the ethics review committees of the five respective hospitals. Written informed consent was obtained from all participants before commencing the data collection. The anonymity and confidentiality of the participants were ensured in every step of the study. There was no risk to the participants related to their participation in this research.