
Abstract
Background
To provide safe tracheal suctioning, the American Association of Respiratory Care guideline discusses the length of suctioning catheter, but the most effective tracheal suctioning catheter technique is still unknown.
Objective
The aim of this study is to compare the amount of simulated secretion produced by five different handlings of a catheter at two different viscosities and in two different models to discover the most effective suctioning maneuver in the various mucus conditions.
Design
In vitro experimental design.
Methods
The amount of secretion aspirated by our researcher's manipulation of a suctioning catheter was measured. The tip of the catheter was recorded using a high-speed video camera to visualize the secretion motion.
Results
The most effective suctioning technique differed depending on the viscosity of the secretion. There were no significant differences between five suctioning methods applied to high-viscosity phlegm in a tracheal membrane model, but the flexion technique was the most efficient for low-viscosity secretion.
Conclusions
Our results imply that the flexion technique was reasonably safe and the most effective of these five methods for low-viscosity secretion.
Background
Recently, the number of children under 18 years old with home mechanical ventilators (HMV) has been increasing worldwide (Amirnovin et al., 2018; Sobotka et al., 2018). Approximately 12.8% of children under 18 years old (9.4 million) require special health care in the United States, and few presents with more challenges than those requiring chronic HMV (Sterni et al., 2016). Despite Japan having the third lowest infant mortality worldwide (Cronin, 2019), the number of children 0–19 years old with HMV has soared from 264 in 2006 to 3,069 in 2015 (Tamura, 2017). As children begin HMV at a younger age, due to the technological development of medicine for premature babies, family caregivers struggle to provide routine care for the ventilator-dependent child/children at high risk of emergency (Baker et al., 2016; Gillen & Morris, 2019; Ramsey et al., 2018; Smith, 1991). Therefore, immediate establishment of evidence-based tracheal suctioning techniques is required to satisfy healthcare demands qualitatively and quantitatively for children with HMV (Wise et al., 2019). Additionally, to maintain a good relationship with family caregivers, the education system must be well structured (Brooks et al., 2008; Moore et al., 2016).
The American Association of Respiratory Care (AARC) Clinical Practice Guidelines recommend shallow suctioning rather than deep suctioning (American Association for Respiratory Care, 2010). Shallow suctioning uses a suctioning catheter with the same length as the tracheal tube, whereas deep suctioning techniques involve insertion of the suctioning catheter until the tip of catheter hits the bifurcation of the trachea and then removal of the catheter by 1 cm before application of suctioning pressure. The latter suctioning method risks damaging the tracheal membrane, which causes hemorrhage, but the effectiveness of the actual maneuver, including whether twisting is effective or not, requires further research.
Effectiveness of suctioning catheter control relies on the secretion's viscoelasticity. In the case of pulmonary diseases, such as cystic fibrosis, chronic obstructive pulmonary disease, and asthma, the viscoelasticity of mucus is usually increased (Markovetz et al., 2019). Ciliary action and cough are incapable of effectively clearing the sticky mucus, leading to its accumulation and even the complete blockage of the airway. On the other hand, if the viscosity is too low, it is likely the mucus will slide down into the lung and flood the alveoli (Chen et al., 2019). Several studies have analyzed the action mechanism of the expectative (App et al. 1993; Jory et al., 2018), but to our knowledge, no research paper has studied the most safe and effective catheter operation method for different viscosities. In other studies, viscosity was the most influential factor on suctioning volume over catheter sizes and vacuum pressures (Copnell et al., 2009; Oshima & Matsuyama, 2014). Therefore, the aim of this paper is to discover the relationship between the motion of the tracheal suctioning catheter and the amount of secretion in the context of different viscosities.
Methods
Experiment 1, using an electric portable suctioning machine (Shin-Ei Industries, Inc., KS-700) and a 10-French suctioning catheter with two side tip openings (Terumo Corporation, 40 cm in length, 3.3 mm outside diameter), high-viscosity simulated airway secretion (KOKEN CO., LTD., 66,600 mPa.s (24°C), fruit jam-like) was suctioned on a round plate (5 cm diameter). In Experiments 2 and 3, high-viscosity secretion (Mogitan, KOKEN CO., LTD., 66,600 mPa s (24°C), fruit jam-like) and low-viscosity secretion (MW23, KYOTO KAGAKU CO., LTD., 22 mPa.s (24°C), Worcester sauce-like), respectively, were put into a vinyl chloride transparent tube (10 cm, 22 mm outside diameter, 18 mm inside diameter) and the amount of suctioned secretion was measured. The viscosity of water is 0.91 mPa.s (24°C).
The definitions of catheter maneuvers used are (1) static method; (2) piston method, which moves a catheter forward and backward 20 mm per second; (3) rolling method, which moves a nurse's hand alongside the tracheal tube inside diameter 360° per second; (4) twist method, which turns the outside diameter of a catheter 180° per second; and (5) flexion method, which involves bending the catheter with the left thumb so as not to apply vacuum pressure.
Following the AARC Guideline 2010, suctioning pressure was set at 150 mmHg (≒20 kPa) (American Association for Respiratory Care, 2010). Pressure application time was 10 s, which is less than the 15 s recommended in the AARC guideline. The amount of suctioned phlegm was measured pre- and post-procedure by a digital scale. The procedure was repeated 10 times for each of the five methods by a single researcher to avoid dispersion. Both high- and low-viscosity phlegm were kept at room temperature (24°C) and colored red using food dye to facilitate observation of the absorption. High-viscosity phlegm (5 g, approximately 3 cm diameter) was placed on the flat membrane model for each procedure (Experiment 1). In the trachea membrane model, 2 g of high-viscosity phlegm (Experiment 2) or 3 g of low-viscosity phlegm (Experiment 3) was placed 3.5 cm from its entrance, using a disposable syringe.
The motion of the catheter tip in Experiment 1 was recorded by a high-speed camera (Q1 m, nac, Japan) with a high-intensity LED light (Experiment 4, Figure 1). Q1 m enables capture of 2,000 frames per second at 1,280 × 1,024 pixels. Video data were analyzed by movie editing software (HXLink SP-642, nac, Japan).
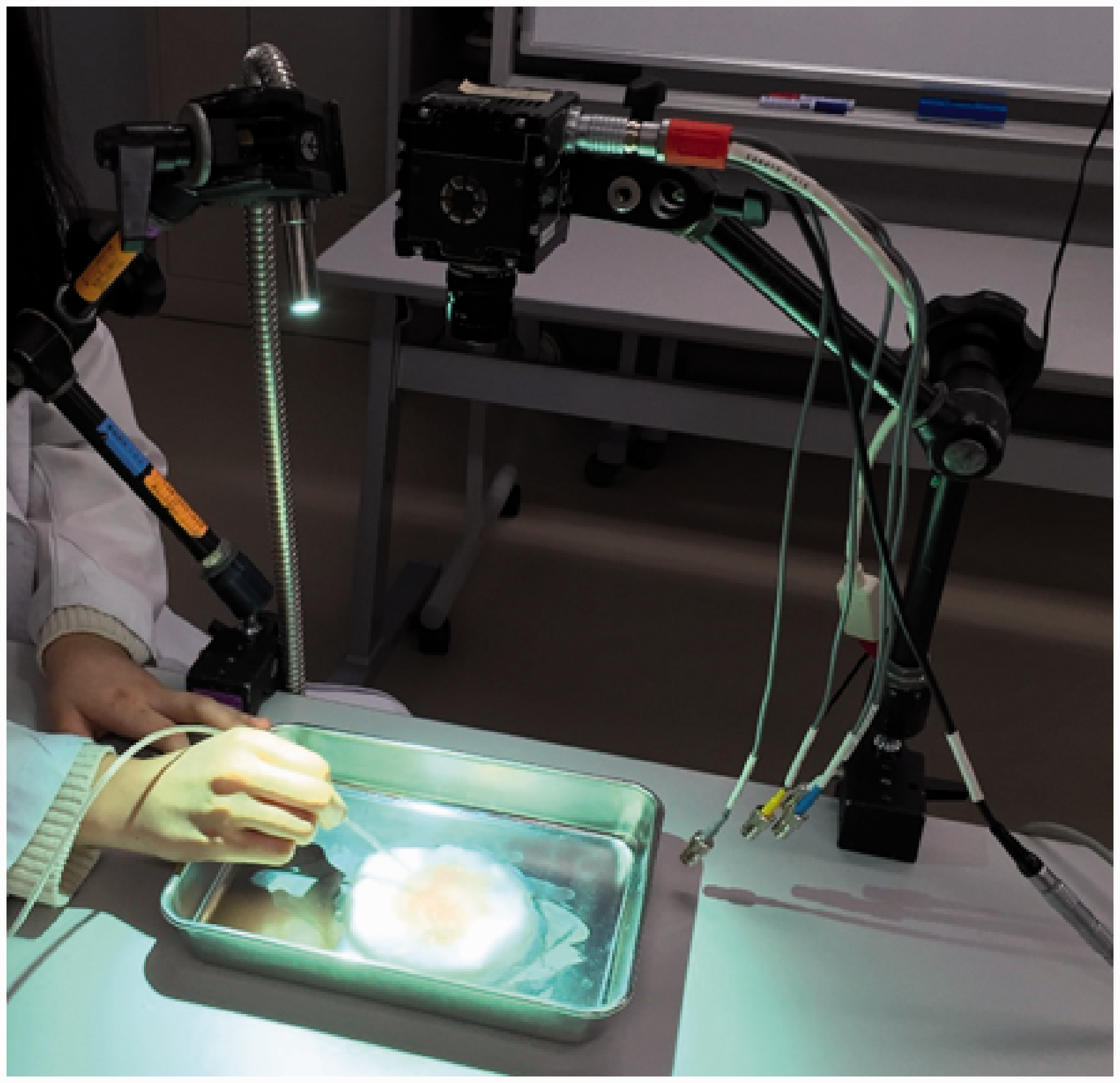
Overview of the Experiments. This picture is an overview of the experiment 1 and 4.
Data were analyzed using SPSS version 22 and Microsoft Excel 2016. One-way analysis of variance (ANOVA) was evaluated with the level of acceptable significance set at p < 0.05 and F-test with degrees of freedom reported. When a significant difference was found using one-way ANOVA, post hoc multiple comparison analyses were performed using Tukey's test. Recorded video data from the high-speed camera were observed by experienced researchers and the description of the results discussed to ensure reliability.
This study does not require any participants, therefore there is no requirement of ethical consideration.
Results
Experiment 1
The average amount of high-viscosity secretion suctioned in the flat membrane model was statistically significantly different between the methods, with 0.31 ± 0.094 g for the static method, 0.480 ± 0.133 g for the piston method, 0.320 ± 0.108 g for the rolling method, 0.430 ± 0.119 g for the twist method, and 0.450 ± 0.120 g for the flexion method by a one-way ANOVA (F(4, 9) = 2.578, p = 0.006). The piston method aspirated the maximum amount of phlegm. Post hoc Tukey's multiple comparisons indicated that there were statistically significant differences between the static and piston methods (p = 0.025) and between the piston and rolling methods (p = 0.039) (Figure 2).
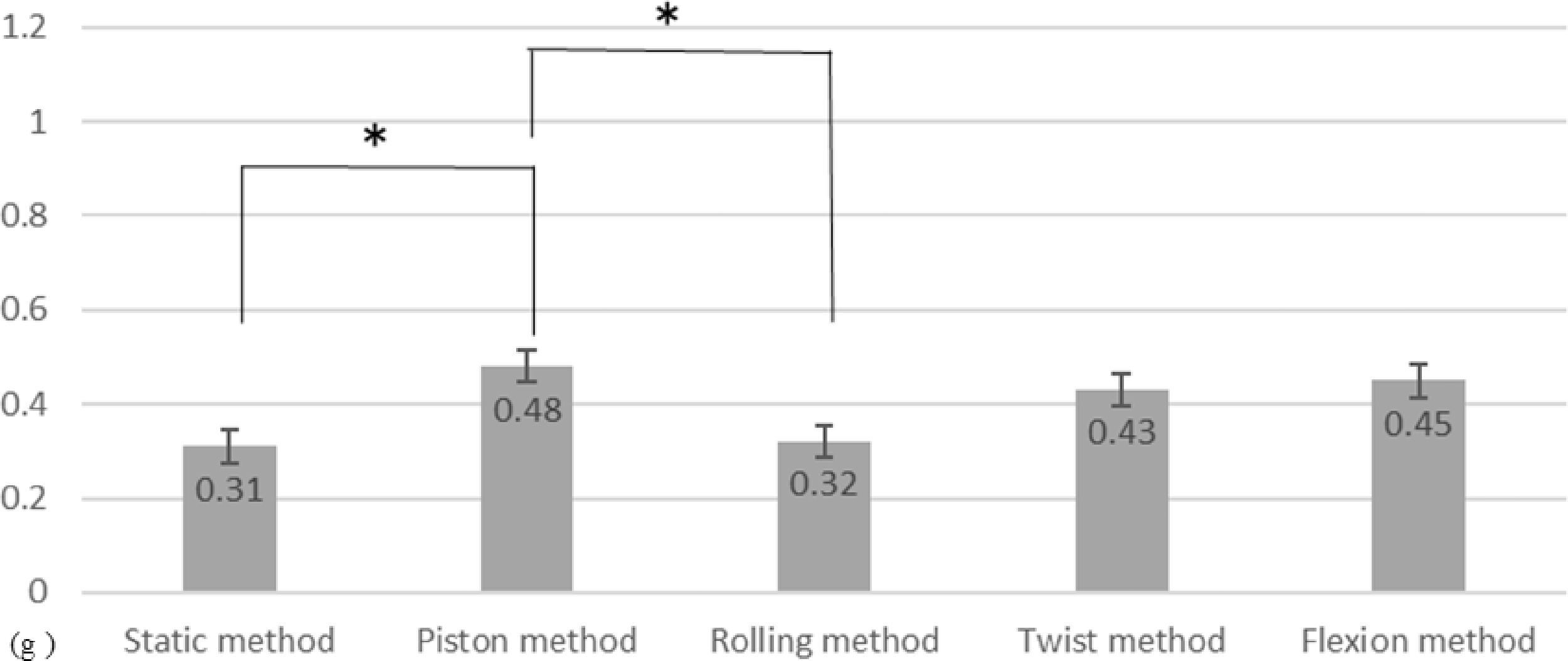
Average Aspiration Volume of High-Viscosity Sputum on the Flat Model. Average sputum suctioned by the five methods was compared, using high-viscosity secretion and the flat membrane model. The piston method was found to be the most effective suctioning method.
Experiment 2
No statistically significant differences were found between the average amounts of suctioned high-viscosity secretion by these five methods in the simulated airway membrane model (F(4, 9) = 2.58, p = 0.086). The mean suctioned secretion weight using the static method, piston method, rolling method, twist method, and flexion method were 0.36 ± 0.080 g, 0.31 ± 0.108 g, 0.30 ± 0.148 g, 0.42 ± 0.125 g, and 0.43 ± 0.090 g, respectively (Figure 3).
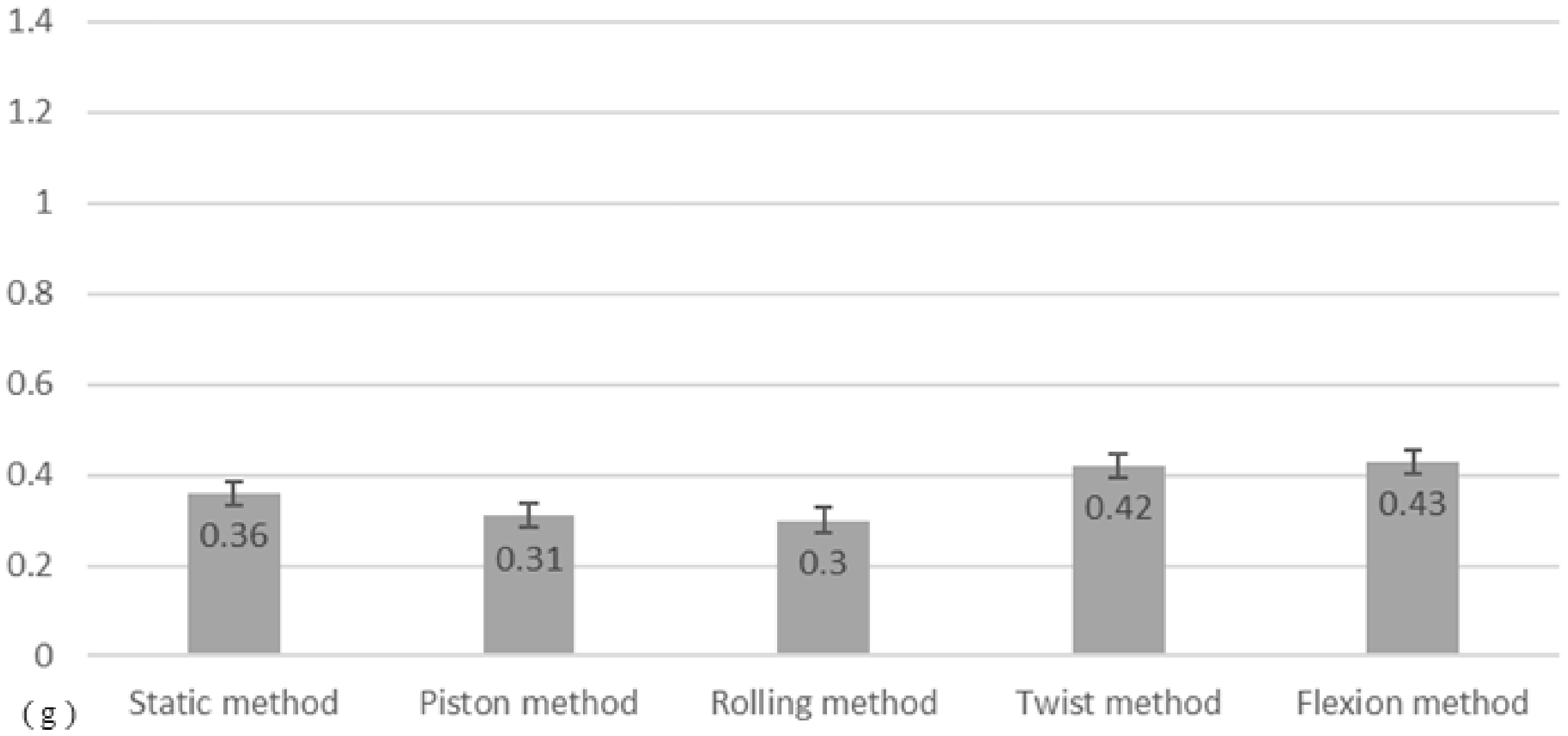
Average Aspiration of High-Viscosity Sputum in the Trachea Model. Using high-viscosity secretion in a tracheal membrane model, average sputum suctioned by the five methods was compared. There were no statistically significant differences between the five suctioning methods.
Experiment 3
Figure 3 shows that the average amount of suctioned low-viscosity secretion using the simulated airway membrane model was significantly different between the methods (F(4, 9) = 2.579, p = 0.001), with the static method aspirating 0.970 ± 0.219 g, the piston method 0.760 ± 0.169 g, the rolling method 0.980 ± 0.193 g, the twist method 1.010 ± 0.130 g, and the flexion method 1.150 ± 0.186 g (Figure 4). Results from post hoc Tukey's multiple comparisons indicated that there were statistically significant differences between the piston and twist methods (p = 0.042), and between the piston and flexion methods (p = 0.000). The flexion method aspirated the maximum secretion.

Average Aspiration Volume of Low-Viscosity Sputum in the Trachea Model. Average sputum suctioned by the five methods was compared, using low-viscosity secretion and a trachea membrane model. The flexion method was found to be the most effective suctioning method.
Experiment 4
From observation of the high-speed video camera, phlegm entering the catheter tip aperture and two side apertures was found in high viscosities. In the case of the high-viscosity secretion, it started moving into these catheter apertures after the catheter tip aperture and two side apertures were imperforated by secretion (Figure 5).

High-Speed Camera Used During Aspiration of Simulated Secretion. High-viscosity secretion does not travel into a catheter until all apertures occluded (white arrows).
Strong vacuum pressure was required to suction high-viscosity airway phlegm. Thus, future studies must define vacuum pressure that is adequate without causing any adverse events based on the viscosity of phlegm.
In the rolling method, holding a catheter and rotating the dominant hand to move the tip of the catheter produced only anteroposterior movement of the catheter tip. Relatively huge amounts of phlegm were aspirated when the participants removed their thumb from bending the suctioning catheter in the flexion method.
Discussion
In our study, the most effective catheter maneuver differed depending on the viscosity of the expectoration. The average high-viscosity secretion suctioned significantly differed between the static and piston methods and between the piston and rolling methods on the flat membrane model in Experiment 1, whereas no statistically significant differences were found between these five methods in the simulated airway membrane model in Experiment 2. In Experiment 3, the average amount of suctioned low-viscosity secretion significantly differed between the piston and twist methods and between the piston and flexion methods.
Despite there are several classifications such as Miller & Jones’ macroscopic classification (Miller & Jones, 1963) and Gecklers’ microscopic classification (Geckler et al., 1977), there has been no classification of airway phlegm viscosity. Therefore, we used two variations of viscosity in this study. Interestingly, high-viscosity secretion does not travel into a catheter until all apertures occluded as shown in Figure 5. This result implies that the thicker the phlegm, the more pressure is required. Considering about the risk of high-pressure for the airway membrane, one of limitations of this study might be examine relationship between viscosity and suctioning pressure.
The other factor we must consider is that the flat model was visible to the researcher. The flat membrane was prepared for observation by a high-speed camera; therefore, the tip of the catheter was able to be controlled as it effectively aspirated the secretion. In Experiment 1, the most effective method was the piston method; however, using a simulated tracheal membrane model in Experiment 3, the piston method aspirated the lowest amount of secretion. Because the position of the sputum inside of the trachea model renders it invisible to the researcher, catheter control is blind. As the high-speed camera reveals that absorption of high-viscosity sputum into a catheter begins when the catheter tip aperture and two side apertures are occluded, a keen-edged sense of the position of the sputum at the catheter tip is necessary when the position of the sputum is invisible.
In addition, a statistically significant difference in aspiration quantity was seen between the piston and rolling method in Experiment 1, but the motion of the catheter tip was the same anteroposterior movement in both methods, according to the high-speed camera results. In the piston method, a manipulator could not completely avoid intentional movement, but the rolling method causes incidental movement of the catheter tip when the catheter is turned. Therefore, visible and prompt feedback might increase aspiration quantity for novice nurses and nursing students.
The flexion method aspirated the most secretion in Experiment 2, but no significant differences were seen across the five operation methods. This implies that with high-viscosity sputum, the absorption pressure and other factors including the position of the side apertures and/or viscosity of phlegm had a greater influence on the quantity of absorption than the catheter operation method.
The flexion method produced the maximum mean absorption quantity in Experiment 3. From the high-speed video camera recording, absorption just after the thumb opening was quick compared with that of other suctioning methods. The twist method ranked second after the flexion method. Catheter contact time on secretion might be another factor to measure the suctioning effectiveness.
In previous research in which we compared two suctioning methods, the dynamic pressure method and the static pressure method, we concluded that the former method is highly effective for aspiration as it increases actual aspiration pressure by bending the catheter (Colley et al., 2018). The dynamic pressure method can be seen as the same procedure as the flexion method in our study. On the other hand, the static pressure method is similar to a vacuum cleaner with side holes; it is slow to reach actual suctioning pressure within 10 s of suctioning. Therefore, the timing of setting pressure application is also an influencing factor for suctioning effectiveness. When the setting pressure was carefully applied to avoid membrane hemorrhage, the flexion method was the most effective for the absorption of low-viscosity sputum because the absorption pressure does not exceed the setting pressure.
In this paper, we focused on five suctioning methods and two viscosities. Further research is still required to unveil the most effective and safe suctioning method, as it might differ depending on conditions such as adequate catheter control for viscosity, adequate pressure for viscosity, adequate catheter size for viscosity, location of the phlegm, adequate length of the suctioning catheter, adequate number and size of side holes for the amount of phlegm, and the inside diameter of the patients' trachea. As the expectorant is non-Newtonian and has a large range of viscosities depending on flow conditions, it will also be necessary to examine the influence of non-Newtonian characteristics on suctioning effectiveness.
Conclusions
The most effective catheter maneuver among the five-catheter motion differed depending on the viscosity of the expectorant. For high-viscosity phlegm, there were no significant differences among the five methods using the trachea membrane model. The piston method was the most effective method in the flat membrane model, when the phlegm was visible. However, in a clinical setting, it is not visible, and the piston method has the risk of damaging the tracheal membrane. For low-viscosity secretions, however, the most effective suctioning method was the flexion method. These results implied that the flexion technique was reasonably safe and the most effective technique for the low-viscosity secretion.
Phlegm is not a Newtonian fluid, thus, examining the influence of non-Newtonian characteristics on suctioning effectiveness will be necessary in future research. Further research is required to determine the most effective and safe suctioning method for any occasion.
Footnotes
Acknowledgements
A part of this study was presented at the International Congress on Pediatric Pulmonology (CIPP) XVIII in 2019 in Chiba, Japan.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a JSPS Grant in Aid for Scientific Research (19H03877).