
Abstract
Introduction
In hospitals, the nurse uses the bed alarm system for patients’ safety, which may have some forms of physical restraints included, depending on the situation. However, the nurses’ perceptions of the bed alarm system with reference to restraints are yet to be clarified. Moreover, there were no reports that can shed light upon the factors that relate to nurses’ perceptions about the bed alarm system in Japan. The objective of this study is to investigate the nurses’ perception on whether the bed alarm can be considered as a form of physical restraint and to elucidate the factors that pertain to the nurses’ perceptions regarding the bed alarm.
Methods
This study conducted a quantitative cross-sectional survey. We used bivariate logistic regression analyses to investigate the nurses’ perception and the factors affecting these perception. Ethical approval was obtained from the research ethics committee of the Kyoto University. Participants opted for answering the questionnaire voluntarily.
Results
The sample population comprised of 289 nurses from 10 acute-care hospitals. Out of these, 214 (74.0%) nurses considered the bed alarm system as a form of restraint, and 75 nurses (26.0%) did not. Furthermore, the nurses’ perception was relevant to the hospitals that they belonged to, their years of experience, and the content of education. It was especially interesting that the group of nurses with little experience had the consciousness of being considered the bed alarm as restraint compared with nurses with many years of experience.
Conclusion
The alarm systems are gradually being considered to be classified as a restraint. Hospitals should ensure providing an ethically sensitive climate and appropriate educational opportunities to help nurses build these perceptions for patient care. An ethically sensitive climate and appropriate educational opportunities would lead to an environment that nurtures nurses with the ability to recognize problems in daily care.
Background
In principle, physical restraints should be prohibited in all situations; however, in acute-care hospitals, restraint tends to be recognized as a necessity in emergency cases because treating patients’ injuries and saving their lives are prioritized in acute-care settings. However, adverse effects of applying physical restraints have been reported, such as direct injuries and asphyxiation, and even increased chances of sudden death (Evans et al., 2003).
Furthermore, the use of physical restraints violates human rights (Dodds, 1996). Therefore, bed alarm systems are being used as an alternative to physical restraints (Hilbe et al., 2010; Markwell, 2005). Because the alarm system can be used without being noticed by the patient, it has become a common method for managing difficult clinical situations.
Various types of bed alarm systems (also called the bed exit alarm or motion sensor) are available, such as clip alarm that consists of a magnet and pull-cord activation, infrared bedside monitor, sensor pad alarm that is applied to the bed, or chair alarm that gets triggered by the patients’ weight. Nurses usually prefer the bed alarm system, especially when patients tend to leave the bed (Hilbe et al., 2010) or wander about the hospital. These alarm systems are used for ensuring the patients’ safety. The previous study stated that bed alarms are the least expensive and the easiest to implement among all the fall-prevention methods; therefore, hospitals and/or nursing leadership might encourage the use of bed alarms as a less costly endeavor (Fehlberg et al, 2017).
However, its effectiveness is debatable. Previous research has indicated a significant decrease in the mean number of falls per patient when using a bedside chair and a bed pressure sensor in an orthogeriatric rehabilitation ward compared with the preintervention period (Sahota, 2009).
On the contrary, some conflicting reports suggest that the use of bed alarm systems did not have any statistically or clinically significant effects on fall-related events or the use of physical restraints (Shorr et al., 2012). Moreover, the ethical aspect of employing bed alarm systems requires clarification. Generally, bed alarm systems are not included in the list of systems that employ physical restraint because they are usually defined as a restriction of the patient’s actions to inhibit movement by using a cord, belt, bedsheet, or a restraining band (Arai & Leibowitz, 2001). It is difficult to define alarm systems as part of physical restraint systems because they do not directly bind a patient to the bed; therefore, it can sometimes be considered as a protective device.
Furthermore, most studies on alarms focus on the innovation of novel techniques of restriction that may be seemingly gentle to patients. In addition, the criteria for the use of bed alarms are not comprehensively established (Hubbartt et al., 2011). The use of bed alarms has, therefore, been controversial from the ethical viewpoint.
In 2017, the Centers for Medicare and Medicaid Services (CMS) implemented restrictions on the use of bed and chair alarm systems in senior housing because of the question for their efficacy, the problem of “alarm fatigue,” and the problem potentially harmful emotionally and physically to the resident (The CMS, 2017). While alarms are not prohibited from being included as part of a plan, they should not be the primary or sole intervention to prevent falls. Therefore, the use of alarm systems in the hospital should be reconsidered.
Bed Alarms: Standard Unstandardized Practices
In Japan, strict standards about the application of physical restraints have been established; however, the criteria regarding the use of bed alarms have not been standardized yet. In some hospitals, nurses are forced to make a decision on the use of bed alarms without any guidelines. In other hospitals, family members are required to sign a letter of consent without the provision of a detailed explanation of the merits and disadvantages of the alarm system. Apart from the observed effect of the bed alarm system, previous reports have also highlighted nurses’ controversial perceptions on the use of the system. For example, a study showed that 25.5% of patients, relatives, and care professionals, including doctors, nurses, physiotherapists, and occupational therapists, agree that bed alarms are a restraint (Vassallo et al., 2005). In addition, a revision of the State Operations Manual for long-term care facilities classifies bed and chair alarms or any position-change alarms that make an audible noise near the resident as a restraint (The CMS, 2017).
Purpose
The aim of this study is to express nurses’ perceptions of the bed alarm system from the viewpoint of considering it as a form of physical restraint. In addition, this research also seeks to identify the factors that may have been related to these perceptions. To achieve this, we used a self-administered questionnaire and compared the background of the nurses who regard the system as a physical restraint with that of the nurses who do not.
Research Question
Do the nursing staff regard the bed alarm system as physical restraint? Which factors are related to the nurses’ perception of the bed alarm system?
Method
Design
This study followed a quantitative cross-sectional survey. The instrument used was a self-administered questionnaire.
Participants
This survey was conducted in 10 acute-care hospitals in Kyoto, Japan. The questionnaires were delivered to the hospital, either directly or indirectly via mail. The hospitals subsequently distributed the questionnaire among the nursing staff. The questionnaires were collected from the hospitals or were mailed directly to the researcher by nurses. The pediatric ward, emergency department, obstetrics department, and intensive care unit were excluded from this research because of the critical features of these wards.
Measurement Tools
The questionnaire was developed after gaining insights from the existing research following a careful and extensive literature review. We drew from previous studies to ensure that the phrasing in our queries would be easily comprehensible to the participants. A pretesting questionnaire was done by three hospital nurses and two professionals in the department of nursing science in our university to ensure the validity and reliability. It consisted of two parts. The nurses were requested to provide their demographic information in the first one, including gender, age, years of experience, position, educational background, and their education levels on issues of ethics, body restraint, and bed alarm system. The second part focused on the question including the nurses’ perception regarding whether the bed alarm system is included in restraint.
Data Collection and Analysis
To perform the collection and analysis of data without compromising confidentiality, each questionnaire was implemented anonymously and managed by code number.
The survey data were analyzed using the SPSS 18.0 J software for Windows (IBM Corporation, Tokyo, Japan). Following this, descriptive statistics was performed to summarize the data. The mean and standard deviation for age and years of experience were calculated and compared, using student’s t test.
The participants were divided into two groups. The former group comprised of nurses who were of the opinion that the bed alarm system is a form of restraint; the latter group consisted of nurses who did not perceive the system as a restraint.
For each group, frequencies and proportions per hospital, gender, position, years of experience, educational background (diploma in nursing school, associate or junior college, or bachelor’s or master’s degree), and educational opportunity (ethics education, physical restraints education, and bed alarm education) were calculated and compared using a χ2 test. Years of experience was defined as being comprised of three categories: newly graduated nurse (less than 2 years), midcareer nurse (3–7 years), and expert nurse (more than 8 years). Furthermore, educational opportunity was divided into five categories (school, introductory course, on-the-job training, out-of-hospital training, and study sessions at hospital wards). The frequencies and proportions for them were calculated and compared using a chi-squared test. Residual analysis was performed on items that had significant differences in the chi-squared test for education and years of experience.
Bivariate logistic regression analyses were conducted to identify the factors that are independently associated with nurses’ perception of whether bed alarms are included in physical restraints using hospital (categories), gender, position, years of experience (categories), and educational opportunity (categories) as predictor variables. Odds ratios (95% confidence interval) were adjusted for gender and hospitals.
Ethical Considerations
Ethical approval was obtained from the research ethics committee of Kyoto University. Each questionnaire had an accompanying letter, explaining the purpose of the research and elaborating on the ways in which the data collected would be used. The identity of the participants was kept confidential, and the returns of the questionnaires were considered as an indication of informed consent for participation in the study. Each questionnaire was assigned a code number to avoid disclosing the hospital name or the identity of the individuals, and the responses provided by the hospital and nurses were kept confidential.
Results
Demographics
From the 737 questionnaires distributed, 469 responses were retrieved. Out of these, 180 had missing values and hence were excluded from the analyses; 269 (93.1%) of the total 289 nurses who answered the questionnaire were females; 20 were males (6.9%), with a mean age of 32.9 years (SD = 8.9, range = 20–58). The mean number of years of their experience was 9.5 years (SD = 8.0, range = 1–39). Among the sample population, 245 (84.8%) of the nurses had a nursing diploma, 24 (7.3%) had a bachelor’s degree, and 3 (1.0%) had a master’s degree; 17 (5.9%) were junior college graduates. With respect to educational opportunities, 257 (88.9%) nurses had attended a medical ethics course, 159 (55.0%) had participated in a body restraints course, and 85 (29.4%) had enrolled in a bed alarm systems course (Table 1).
Chi-Square Test of Factors Regarding the Nurses’ Perceptions (N = 289).

at test.
bχ2test.
**p < .01. ***p < .001.
Nurses’ Attitude Toward the Use of Bed Alarm Systems
In total, 214 (74.0%) nurses considered the bed alarm system to be a form of physical restraint. Those who considered the bed alarm system to not be included in the physical restraint systems amounted to 75 (26.0%; Table 1).
Factors Affecting Nurses’ Perceptions
To analyze the factors that pertained to the nurses’ perceptions of bed alarm systems, we applied a chi-squared test for evaluating significance (Tables 1 and 2). The difference in the perceptions of the nurses regarding bed alarm systems was significant as per the hospitals they belonged to (p < .001; Table 1). More number of nurses belonging to Hospitals 2 and 8 regarded the bed alarm sensor as a restraint. On the other hand, fewer nurses who worked in Hospitals 1 and 10 considered the sensor as a restraint. In addition, the nurses’ perception was also affected by their years of experience; 45 newly graduated nurses regarded the bed sensor as a restraint (15.6%; p = .008), which was significantly higher than nurses of other experience ranges. Education was observed to not affect the nurses’ perception, irrespective of whether they had completed the ethical, physical, or bed alarm systems education (Table 1). However, 150 nurses who had received education about ethics in school (51.9%; p = .026) and 11 nurses who had completed the physical restraints instruction during out-of-hospital training (3.8%; p = .045) significantly tended to consider the bed alarm system as a form of physical restraint (Table 2).
Chi-Square Test of Factors Regarding the Nurses’ Perceptions About Education (N =289).

*p < .05.
Relationship Between Education and Years of Experience
The chi-squared tests were performed for assessing the relationship between the education received and years of experience. There was a significant difference in relation to professional experience (newly graduated nurse, midcareer nurse, or expert nurses) and ethics education (p = .014), ethics education at school (p < .001), physical restraints education (p = .003), and physical restraints education in school (p < .001; Table 3).
Chi-Square Test of the Relationship for the Education and Years of Experience (N =289).

aχ2test.
*p < .05. **p < .01. ***p < .001.
Residual analysis was conducted to identify the cells that accounted for the significant effects (i.e., a residual greater than 2.00 indicates the factor was a major influence for the significant chi-squared test statistic).
A significant number of 47 newly graduated nurses had especially received ethics education at school (adjusted residual = 4.04), and 29 newly graduated nurses had received physical restraints education at school (adjusted residual = 4.09). Eighty-two midcareer nurses had received ethics education at school (adjusted residual = 4.45), 64 midcareer nurses had received physical restraints education (adjusted residual = 2.52), and 43 midcareer nurses had received physical restraints education at school (adjusted residual = 3.15). Contrariwise, 116 expert nurses had received less ethics education (adjusted residual = –2.85), 63 expert nurses had received less ethics education at school (adjusted residual = –7.32), 62 expert nurses had received less physical restraints education (adjusted residual = –3.43), and 20 expert nurses had received less physical restraint education at school (adjusted residual = –6.13).
Results of the Logistic Regression Analysis of the Nurses’ Perception of Bed Alarm Systems
Table 4 shows the results of the logistic regression model. The regression analysis concluded that the hospital that nurses belong to was one of the important factors that can affect nurses’ perceptions. Furthermore, the newly graduated nurses were observed to be 4.1 times (p = .003) likelier than the expert nurses to consider the bed alarm systems as a restraint.
Logistic Regression Analysis of the Nurses’ Perception of the Bed Alarm System (N =289).
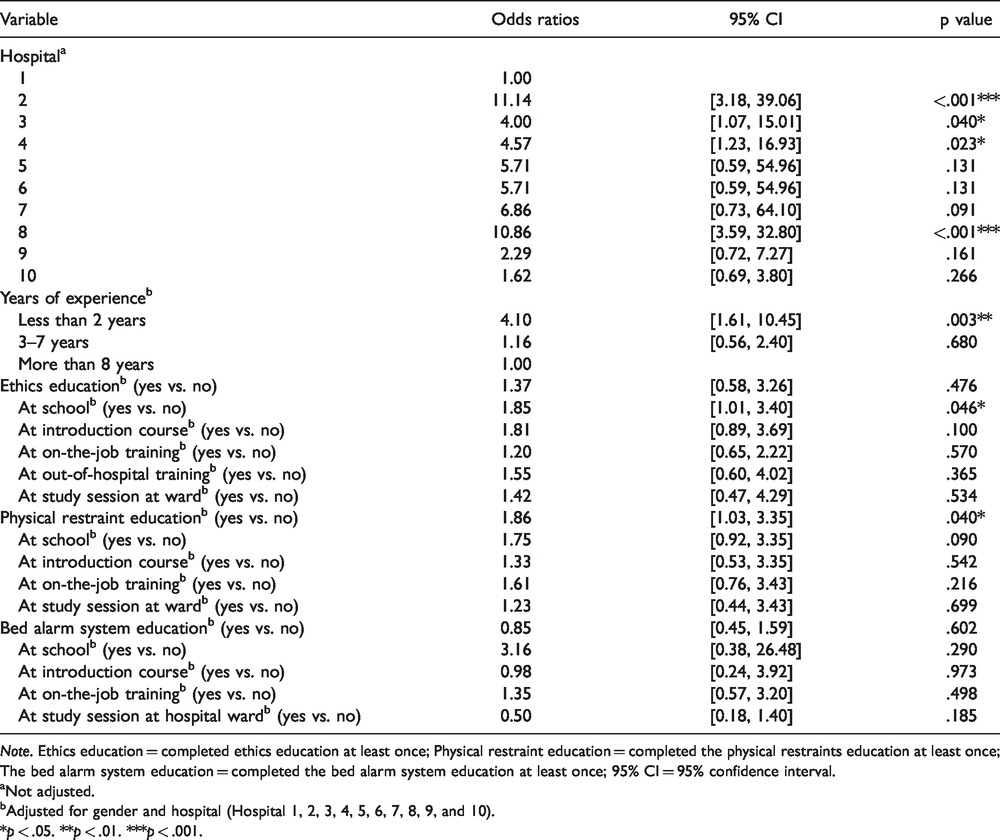
Note. Ethics education = completed ethics education at least once; Physical restraint education = completed the physical restraints education at least once; The bed alarm system education = completed the bed alarm system education at least once; 95% CI = 95% confidence interval.
aNot adjusted.
bAdjusted for gender and hospital (Hospital 1, 2, 3, 4, 5, 6, 7, 8, 9, and 10).
*p < .05. **p < .01. ***p < .001.
When gender and hospitals were adjusted, the nurses who had completed the physical restraints education (odds ratio = 1.86, p < .040; 95% CI [1.03, 3.35]) and who had received ethics education at school (odds ratio = 1.85, p < .046; 95% CI [1.01, 3.40]) considered bed alarm systems a restraint.
We identified several novel factors from this study that are significantly relevant to nurses’ perception of bed alarm systems as a restraint, namely, the educational opportunities that predominantly relate to nurses’ perception was ethics education at school, the physical restraints education, and the physical restraints education at out-of-hospital training.
Although not significantly, the nurses who had received other types of education tended to regard the bed alarm system as a restraint. This indicates that any type of education may be effective in making nurses notice the ethical aspects of the alarm system.
Discussion
Nurses are required to make ethical decisions regarding patient care every day, such as ones relating to patients’ safety, rights and autonomy, advance care planning, surrogate decision making, and so on (Ulrich et al., 2010). In the context of patient safety, inefficient fall-prevention techniques are one of the critical challenges in today’s acute-care hospitals. However, even in emergency, nurses should consider the patients’ rights, privacy, and dignity as well as safety. The recognition of the significance of this has led us to investigate the ethical aspects involved in the use of bed alarm systems.
As initially stated, bed alarm systems are not considered to be included in the list of systems employing physical restraint; therefore, most previous studies on restraint have focused on the innovation of novel techniques of restriction. However, the ethical aspect of employing the bed alarm system has not been investigated entirely and still requires clarification.
This study, for the first time, demonstrated nurses’ ethical perceptions of bed alarm systems and analyzed the relevant factors that could potentially be relevant to their perceptions. Hospital (their workplace), newly graduated nurses, ethics education (especially at school), and physical restraints education were revealed to be factors that affect the perception of bed alarm systems as physical restraints.
The significance of the employing hospital as a factor relating to nurses’ perception is unexpected and fascinating from a research perspective. It indicates that ethical policies may vary between hospitals. Presumably, nurses in some hospitals tend to assume that the bed alarm system is not included in the physical restraint, while in others, they recommend using bed alarm systems for actively preventing falling. This led us to conclude that the ethical atmosphere might be the most important factor in the hospital with respect to providing care. According to a previous report, the ability of the nursing staff to adequately address the ethical issues that they confront can be influenced by the ethical climate in which they work (Schluter et al., 2008). Another report by Hart (2005) also showed that one of the most important factors in moral decision making is the availability of an ethically sensitive environment. We speculate that in our study, the perceptions on bed alarm systems might be significantly concerned with the ethical climate; hence, it warrants the inclusion in this study as a significant parameter.
The second factor was the years of experience. Previous research indicated that 20% of health professionals (doctors, nurses, physiotherapists, and occupational therapists) and 30% of patients and relatives consider bed alarms to be a restraint, respectively (Vassallo et al., 2005).
We hypothesized that newly graduated nurses may have similar views as patients and relatives about the bed alarm system because compared with other expert nurses, they had not used the bed alarm system frequently. In addition, according to a study in 2008, 43.0% of nurses had received ethical education during their professional basic and/or advanced educational program (Grady et al., 2008). In our study, 89% of nurses had received training in ethics education, thereby implying that the significance of ethics education is now understood and is widespread. Table 3 shows that younger nurses have had more opportunities to obtain ethics or physical restraint education compared with expert nurses.
For the aforementioned reasons, we assume that newly graduated nurses in this study may have easily considered the topic as an ethical issue by employing sensors.
The last factor was education. From the results of our study, we infer that the most effective ethical education regarding the bed alarm system is ethics education delivered at school and physical restraints education.
Unexpectedly, education about the bed alarm system itself was not relevant to their perceptions. It is known that ethics education has a significant positive influence on moral confidence, moral action, and the use of ethics resources (Grady et al., 2008). Regarding the education on restraints, existing literature indicates that 85% of the nurses received only a few hours of instruction on the use of restraints on adults and that 53% of them were provided instructions even less than 1 hour (Stilwell, 1991). On the other hand, in Japan, there was a report stating that only 36.3% of the nurses had on-the-job training related to the use of physical restraints (Arai & Leibowitz, 2001); in our report, however, the number of nurses who had undergone this education at school or during their on-the-job training was as high as 55.0%. Thus, it can be concluded that the importance of education on physical restraints has gradually become recognized. However, with respect to bed alarm systems, only one third of the nurses responded in the affirmative to having received instructions on alarm systems. This indicates that the education for alarm systems is not sufficient, as shown in our study. Similar reports were previously published, stating that the education dispensed regarding alarms was insufficient (Bach et al., 2018; Coyle & Mazaleski, 2016; Yue et al., 2017). However, in their report, the researchers cited previously focused only on the training to use alarm systems safely or to respond more promptly and accurately and did not focus on its ethical aspects. These trainings/instructions may not convey the most important message for preventing fall-related incidents, which nurses think is the reason why patient wants to move. Therefore, we assume that the bed alarm education did not impact nurses’ perception. This result may possibly be due to the fact that the current instruction on the same focuses primarily on the means to use the system effectively but does not comment on the involved ethical issues, such as the fact that the sensors may violate the dignity and privacy of a patient. Some types of bed alarm sensors do not directly restrain the patient’s body. However, they can be a result of restraint by suppressing behavior or instilling a sense of mental restraint. Therefore, nurses should keep in mind the possibility that sensors might be restraints for patients even if they are in acute-care hospitals.
The bed alarm system is reported to cause another problem to nurses—alarm fatigue. It sometimes gives false alarm, which can lead to alarm fatigue (Sendelbach & Funk, 2013). Thus, the nurses could possibly consider the alarm to be a nuisance sound; resultantly, its ethical aspect may be overlooked or even neglected.
As mentioned earlier, alarm systems are gradually being considered before being classified as a restraint depending on the situation (The CMS, 2017). Their use should hence be strictly limited to medical necessities, and even then, it must be continuously reevaluated. For this change, nurses’ perception change is required. From this study, we can speculate that appropriate education can make an impact on nurses’ perceptions that leads to effective use of the bed alarm system. Hospitals are especially responsible for instructing staff nurses about its proper use, including the ethical aspect, and should also address the difficult task of creating an ethically sensitive climate to ensure high-quality nursing care in all situations. Continuing ethical education courses and discussions to promote positive ethical climates will enhance the quality of the care provided by nurses to patients who need the alarm system.
Limitations
There are, despite the various valuable insights given, several limitations to this study. The participants joined the study voluntarily; therefore, these results reflect only the perceptions of nurses who were interested in this survey. The study was conducted in 10 acute hospitals in one city. Thus, this result may not be generalized because the data were collected from one urban area. Further research is required with more participants in various areas.
Implications for Practice
Hospitals need to provide educational opportunities regarding both alarms’ advantages and disadvantages including ethical aspects. This knowledge enables nurses to make informed decisions in using the alarms by themselves. It will lead to create a sensitive environment to nurture nurses who can provide better patient care.
Conclusion
This study provides data on the education of nurses regarding the ethical aspects of bed alarm systems. It sheds light on the factors that affect their perceptions in Japan. Our study indicated that more than half of the participating nurses considered the bed alarm system to be a form of physical restraint, and this perception is observed to have been related to the following factors: the hospital they worked at, their years of experience, and the education system.
These factors, which have not been reported in the existing literature, are novel ones that can pertain to nurses’ perceptions toward the bed alarm system. More factors that affect their perceptions should be clarified from an ethical point of view.
Footnotes
Acknowledgments
The authors are grateful to all the participants for their involvement in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the management expenses grants of Kyoto University.