
Abstract
Introduction
Considering the situation where the number of people with diabetes is increasing, we need to find ways to support more efficient and effective outpatient clinics. Therefore, it is necessary to develop effective support methods and to elaborate a strategy as a system for support after grasping the characteristics of the entire population of people with diabetes.
Objective
The purpose of this study was to identify the characteristics of the diabetes population in outpatient settings by differences in self-care agency and to examine how to support them based on the recognized characteristics.
Methods
Participants were 261 people with diabetes under outpatient care in Japanese institutions from whom demographic data on age, gender, HbA1c, and treatment method were collected as well as self-care agency data based on the Instrument of Diabetes Self-Care Agency consisting of 40 items. The data were analyzed using cluster analysis to compare age, gender, HbA1c, duration of diabetes, type of diabetes, and insulin therapy between clusters.
Results
The analysis identified six clusters, including a group with favorable HbA1c but low total self-care agency scores that were likely to affect their blood glucose control in the future, although accounting for as small a portion as 3% of the total. In addition, a cluster with poor HbA1c and generally low self-care agency was also identified accounting for about a quarter of the total population. These clusters were considered to require further support. Clusters having markedly low self-care agency items, stress-coping ability, or the ability to make the most of the support available were also identified.
Conclusion
The six clusters need to be assisted in focusing on mental or social support. Accordingly, consideration of the support system for people with diabetes based on an understanding of the cluster characteristics seemed to enable more efficient and effective support.
Introduction
An increase in the number of people with diabetes and the health-care cost has become a major problem worldwide (Gregg et al., 2014; International Diabetes Federation, 2017; Ministry of Health, Labour and Welfare, 2015). Consultation time per person in Japanese clinics is very short, even in outpatient clinics for diabetes, due to the increase in the number of people with diabetes. Kabeya et al. (2017) found that the mean consultation time per person was 10.1 minutes. Under such circumstances, nurses need to support self-care, not only treating diabetes by improving blood glucose but also treating people’s quality of life and well-being so that the people can live with dignity. However, it is difficult for nurses to secure enough time for supporting each person.
Considering the situation where the number of people with diabetes is increasing, we need to find ways to support more efficient and effective outpatient clinics. Therefore, it is necessary to develop effective support methods and to elaborate a strategy as a system for support after grasping the characteristics of the entire population of people with diabetes.
Many studies conducted from such a viewpoint used demographic data such as the type of diabetes, the presence or absence of complications and differences in treatment, the physical condition of the glycemic control state, age, and gender (Kobayashi et al., 2006; Lee, Colagiuri, & Flack, 2018; Zhang & Padman, 2017). However, we thought that it would be important to grasp the characteristics of a population of people with diabetes about self-care when nurses do provide support. Orem (2001) defines self-care as the “practice of activities that individuals initiate and perform on their own behalf in maintaining life, health, and wellbeing.” (Orem, 2001, p. 43). Nurses aim to improve the glycemic control of people with diabetes and the quality of life by supporting their self-care, but to do so, it is necessary to change the self-care behavior of people with diabetes. However, we cannot directly change their behavior. We believe that it is a key role to encourage and support self-care agency inherent in them so that they lead to the voluntary and intentional behavior of people with diabetes. Therefore, we considered that focusing on the self-care agency is important in considering the nurse’s support method.
The purpose of this study was to identify the characteristics of the population with diabetes based on differences in the self-care agency of people with diabetes during outpatient visits. And then we examined the guidance based on the characteristics of the population with diabetes.
To grasp the self-care agency of people with diabetes, we selected Instrument of Diabetes Self-Care Agency (IDSCA), which consists of 8 elements and 40 items. This is a scale on which validity and reliability are verified after qualitatively and functionally extracting what sort of self-care agency the people are paying attention to when nurses support people with diabetes. We considered that we could capture the characteristics of group self-care agency in a way that could be utilized for nursing support by utilizing this scale.
Methods
Selection Criteria of Participants
Participants were people with diabetes who were in an outpatient clinic, who were able to communicate by language, and who gave consent for research cooperation. The data collection period was 15 months. People with a high necessity of assistance from a viewpoint other than self-care support, such as mental instability and physical suffering, were excluded from the participants because the use of self-care agency measurement tools may cause mental and physical adverse effects on them. The participants were selected to represent a population of persons who met all of the following criteria: (1) 18 years of age or older; (2) diagnosed with diabetes (either type 1 or 2); (3) currently undergoing outpatient treatment; (4) taking medication for diabetes (daily insulin or oral hypoglycemic); (5) able to read, write, and speak Japanese; and (6) did not have gestational diabetes.
Data Collecting Site
Data were collected from hospitals and clinics where each researcher and research collaborator could collect data and where people with diabetes who gave consent for data collection were receiving treatment.
Process of Recruitment and Consent of Research Collaborators and Participants
Research collaborators
At a workshop for certified diabetes care nurse, under the permission of the organizer, we explained the contents and main purpose of this study to participants and requested research cooperation in writing and then confirmed the intention of consent for research cooperation in writing.
Directors of cooperating institutions
We explained the contents and purpose of this study in writing to the directors of the institutions where the researcher would collect data and to which the research collaborators belong. If necessary, we obtained approval from the Ethics Review Board of each facility.
Participants
Researchers or research collaborators explained the contents of the study while presenting the document to participants, and consent for research cooperation was confirmed by signing the consent form.
Data Collection Method
Basic data of participants such as age, gender, type of diabetes, treatments, and HbA1c values (at the time of IDSCA measurement) were collected from the medical record. HbA1c values were measured by taking blood samples on the day of answering the IDSCA.
Researchers or research collaborators asked the participants to respond to the IDSCA (modified version), tool for measuring diabetes self-care agency, and collected them on the spot.
Instrument
The IDSCA was developed to assess self-care agency in people with diabetes. The IDSCA was verified as demonstrating internal consistency and validity in a previous study (Miyawaki et al., 2015; Shimizu et al., 2011; Waki et al., 2016). This scale consisted of the following eight subscales, each with five question items: ability to acquire knowledge, stress-coping ability, ability to make the most of the support available, monitoring ability, application or adjustment ability, motivation to self-manage, ability to self-manage, and ability for body self-awareness. Each item is rated on a 6-point Likert scale ranging from 0 (strongly disagree) to 5 (strongly agree). IDSCA is a self-rating scale. Obtaining a high score on each subscale indicates that the self-care agency of an individual with diabetes is good. Permission to use the instrument in the present study was granted by the original authors.
Statistical Analysis
All statistical analyses were conducted using PASW Statistics 18, the JMP Pro 14.0.0. To evaluate the demographics and characteristics of the participants, descriptive analysis included the means, standard deviations, and percentages. We used the Ward method, which is a hierarchical approach of cluster analysis to clarify the characteristics of the self-care agency of the group of people with diabetes.
After the cluster analysis, we compared the differences in age, gender, HbA1c value, average duration of diabetes, type of diabetes, and presence of insulin therapy between clusters using the Kruskal–Wallis test, Chi-square test, and Fisher’s exact test. The threshold for statistical significance was set at a p value of .05. In addition, each effect size was calculated. If the effect size was 0.2 or more, the result was adopted.
Ethical Considerations
The procedures and protocols used in this study were approved by the Human Ethics Review Committee of Osaka University and by the ethics committees of the participating hospitals. This study was conducted in accordance with the Declaration of Helsinki. All patients gave informed consent to participate.
Results
Characteristics of the Sample
The participant’s characteristics are shown in Table 1. The mean age of the participants was 60.2 years (SD = 12.6, range = 19–88). There were 105 females and 148 males. The duration of diabetes ranged from 2 months to 50 years (M = 12.4, SD = 9.4). The majority (91.2%) of them had type 2 diabetes mellitus. In addition, 50.6% were undergoing insulin therapy. Mean HbA1c was 7.3% (M = 7.3, SD = 1.3).
Demographic Summary of Participants (N = 261).

Note. HbA1c = glycated hemoglobin.
Score for diabetes self-care agency
Table 2 shows Cronbach’s alpha values of the IDSCA as the internal consistency reliability of the IDSCA. The Cronbach’s alpha of each subscale on the IDSCA ranged from .763 to .842. The mean score of each subscale on the IDSCA ranged from 17.5 to 22.2 out of 25 points. The mean total score of the IDSCA was 157.7 out of 200 points.
Cronbach’s Alpha and Mean Score of IDSCA (N = 261).

Clustering of subscale score of the IDSCA
A cluster analysis of the eight subscales of diabetes self-care agency classified the participants into six clusters. The numbers of participants in each cluster were 46 (17.6%) in Cluster 1, 71 (27.2%) in Cluster 2, 38 (14.6%) in Cluster 3, 30 (11.5%) in Cluster 4, 69 (26.4%) in Cluster 5, and 7 (2.7%) in Cluster 6 (Table 3). Subscale scores of IDSCA for each cluster are shown in Figure 1.
Characteristics of Each Cluster (N = 261).
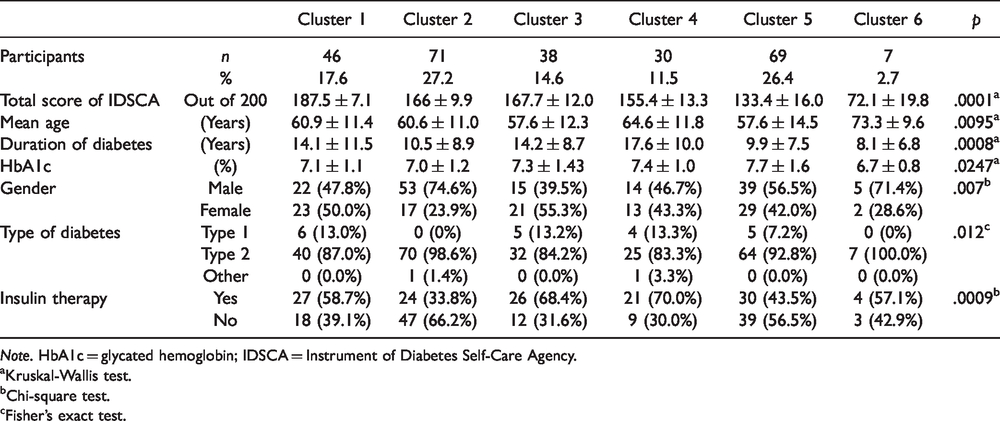
Note. HbA1c = glycated hemoglobin; IDSCA = Instrument of Diabetes Self-Care Agency.
aKruskal-Wallis test.
bChi-square test.
cFisher’s exact test.
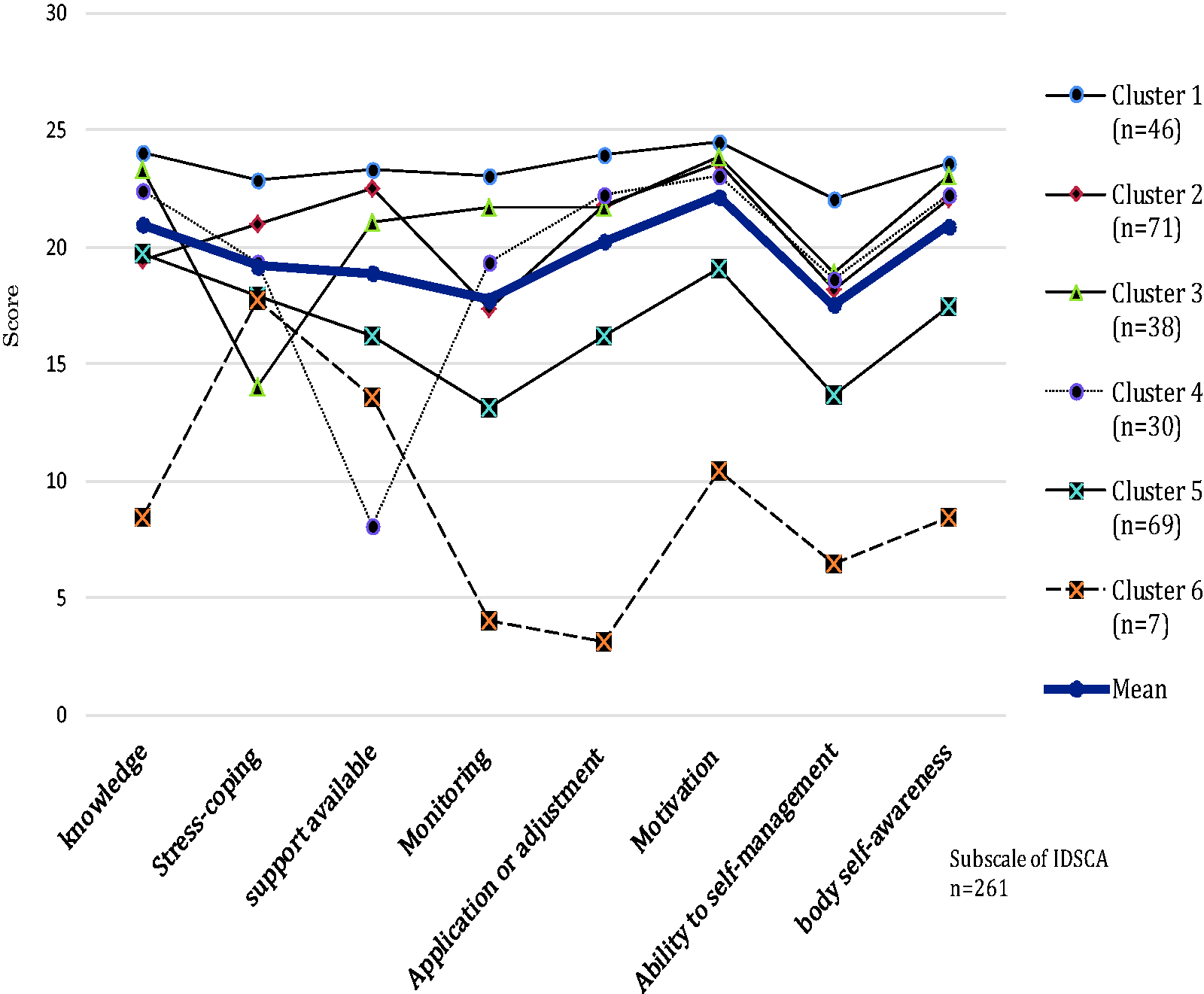
IDSCA scores for each cluster. IDSCA = Instrument of Diabetes Self-Care Agency.
Characteristics of the six clusters
Cluster 1 had the highest total score for self-care agency at 187.5 points, and all subscale scores were highest in six clusters. Cluster 2 was the second highest score for “ability to make the most of the support available” for Cluster 1, but the “ability to acquire knowledge” and “monitoring ability” were lower than the mean score. Cluster 3 had the lowest score for “stress-coping ability” in six clusters, while the other subscale scores were above the mean score for all subscale scores other than the average score of each subscale. Cluster 4 had the lowest score for the “ability to make the most of the support available” in six clusters, while the other subscale scores were above the mean score. In Clusters 5 and 6, the scores for all subscales were lower than the mean. In particular, Cluster 6 had the lowest total score for the IDSCA at 72.1 points and the lowest subscale score, except two subscales (“stress-coping ability” and “ability to make the most of the support available”) among the six clusters (see Figure 1).
Diabetes-specific clinical characteristics
We compared diabetes-specific clinical characteristics among the clusters and found differences between the clusters with respect to age, duration of diabetes, HbA1c, gender, type of diabetes, and insulin therapy (Table 3). As shown in Table 3 and Figures 2 to 4, there were significant differences in age and the duration of diabetes, HbA1c. Cluster 6 had the oldest mean age of 73.3 ± 9.6 and had the shortest mean duration of diabetes of 8.1 ± 6.8 in six clusters. Cluster 4 had the longest mean duration of diabetes of all clusters at 17.6 ± 10.0 and the highest HbA1c (7.4% ± 1.0%). Of the six clusters, the percentage of males was the highest (74.6%) in Cluster 2 and the percentage of insulin therapy was the highest (70.0%) in Cluster 4. The ranking of the average value of IDSCA scores for each cluster was not consistent with that of HbA1c. However, with the exception of Cluster 6, Cluster 5 with the lowest score for IDSCA had the highest HbA1c (7.7% ± 1.6%) and Cluster 1 with the highest score for IDSCA had the lowest HbA1c (7.1% ± 1.1%), which was the second lowest to Cluster 2, the highest. The difference between the HbA1c value and the total score for the IDSCA of each cluster and the mean were plotted in Figure 4.

Mean age in each of the six clusters.

Mean duration of diabetes in each of the six clusters.

Mean HbA1c in each of the six clusters.
Discussion
Characteristics of Each Cluster
In this study, people with diabetes were classified into six clusters based on different characteristics using the IDSCA, a diabetes self-care agency measurement tool. We attempted a cluster analysis of self-care agency to characterize the entire diabetes population and to examine an effective assistance and support system.
First discussed is the most distinctive Cluster 6. Cluster 6 had the best HbA1c despite the far lower total self-care agency score than that of other clusters. Cluster 6 included as few as seven participants and could be considered a unique population. Since Cluster 6 had a shorter history of diabetes than that of other clusters and relatively high ability to make the most of the support available, the cluster might be characterized by the insulin secretion capacity maintained to a certain degree and avoidance of worsening in blood glucose with support from others despite the low self-care agency. A precedent study indicated that some people misunderstood their disease or treatment although they had favorable HbA1c (Holmström & Rosenqvist, 2015). Since the cluster had the highest age, they possibly failed to obtain knowledge that could be used in self-care through conventional initial education alone. Customized support needs to be provided for them to prevent worsening of blood glucose control in the future rather than leaving them without support although they have favorable HbA1c. The percentage in this study population was as low as <3% (7/261 individuals). This cluster is expected to be a minority in outpatient clinics where a number of patients visit. Therefore, progress of diabetes may be prevented and efficiency of support may be improved by positioning the cluster as a cluster requiring intensive assists.
Next discussed is Cluster 5, which had the second lowest total self-care agency score next to Cluster 6 and the highest HbA1c among the six clusters. This cluster definitely needed support because they had high blood glucose even without measuring the self-care agency score and improvement of blood glucose control in this cluster was the key to prevention against worsening in the total diabetes population. In this study, Cluster 5 accounted for a fairly large portion of about one quarter of the total population (26.4%). Therefore, they could deserve considering a strategy different from the usual support as the key cluster for prevention against worsening. Their self-care agency subscale scores were all lower than the mean scores. This seemed to be due to the lack of general self-care knowledge. Their monitoring ability was particularly low among the total items, and it was, therefore, likely that they had general knowledge of diabetes but could not link the knowledge to self-management suitable for their lifestyle with the use of monitoring ability, which prevented improvements in their blood glucose values. A study in the United States found that diabetes-related knowledge level was high among adults with and without diabetes, but that this knowledge could not be easily applied to oneself (Piccinino, Griffey, Gallivan, Lotenberg, & Tuncer, 2015), suggesting that educational interventions that keep patients’ knowledge current are necessary. Although no specific strategy can be determined based on the present result only, it is important to perform further analysis and develop a strategy on the basis of the importance of supporting this cluster.
Although Clusters 3 and 4 were middle ranked for both total self-care agency score and HbA1c, Cluster 3 was characterized by its extremely low stress-coping ability and Cluster 4 was characterized by its extremely low ability to make the most of the support available compared to other subscales. Clusters 3 and 4 both had a substantial number of people accounting for more than 10% of the total. When blood glucose was not improved, support targeted to change the individual’s behavior tended to be considered. However, the presence of the clusters where mental assistance and assistance to resolve problems regarding support by others are prioritized has been identified as an important factor to consider as effective and efficient support to resolve problems. The preceding studies demonstrated evidence of the effect of mental assistance and assistance for support by others. One of such studies concluded that diabetes distress improves blood glucose control. Other studies demonstrated the effectiveness of an emotion-focused educational program in reducing diabetes distress (Chew, Vos, Stellato, Ismail, & Rutten, 2018) and indicated the effects of intervention by family (Gomes et al., 2017) or potentiated social support (Vissenberg et al., 2017). Therefore, such attempts were meaningful.
Clusters 1 and 2 were both characterized by higher total self-care agency scores than that of the other clusters with relatively favorable HbA1c. Compared to Cluster 1, Cluster 2 had a lower ability to acquire knowledge, monitoring ability, and ability to harmonize self-management with their own lives. This might be because the self-management was not customized to their lifestyles. Although other clusters were prioritized when considering effective and efficient support in the outpatient settings where many patients visit and time and manpower involved were limited, assistance for people in Cluster 2 was important as the role of nurses not only to improve blood glucose but also to support life with diabetes harmonized with their own lives.
Understanding of the Characteristics of the Population Through Cluster Analysis
This study characterized the population consisting of people with diabetes visiting outpatient clinics in Japan through cluster analysis to study effective and efficient supports. Needless to say, people living with diabetes have their past life histories under the effect of the environment where they have lived and need complex and highly customized support. Although individual assistance is required in accordance with such situations, resources of manpower are actually limited. In this context, the result from this study was able to indicate the direction of support through an analysis, including not only the blood glucose control status but also the view of self-care agency, suggesting the efficacy of the analysis as a method to examine a data-based strategy.
Fazio et al. (2019) demonstrated in their study results that the success of the people with diabetes included not only improvement of HbA1c but also change in mindset or awareness, change in engagement with healthcare resources, and change in physical or emotional health. They stated “when healthcare professionals focus on HbA1c as the main indicator of diabetes management success, important changes in individuals’ health and well-being may be overlooked or undervalued.” (Fazio et al., 2019, p. 10). When we consider effective and efficient support, we should not only focus on the improvement of blood glucose control but also evaluate and discuss from a broad view taking self-care agency into consideration.
Limitations
The IDSCA was used in this study to evaluate self-management ability in patients with diabetes, but the participants were all Japanese. Thus, the generalizability of this study is limited. In addition, this study performed cluster analysis focusing on self-care agency, and based on these results, further analysis is needed, including a broad range of data, such as blood glucose control status and treatment method.
Implications for Practice
The nurses have a role to support self-care targeted to improvement not only in blood glucose but also in patient’s well-being. To achieve these goals, comprehensive assessment is required including not only patient’s physical status but also their self-care status.
Many patients visit the outpatient clinic, and it was suggested that characterizing the diabetes population, including self-care agency, may allow discussion of a strategy to support them more efficiently and effectively.
Currently, studies have identified evidence of various educational programs. To consider which educational program is suitable for the diabetes population, adaptation of such analytical approach to identify the rationale may lead to better support.
Conclusions
A cluster analysis of 261 people with diabetes in the outpatient settings was performed to characterize this population. As a result, the analysis identified a group with favorable HbA1c but low self-care agency that may affect blood glucose control in the future and another group with poor HbA1c with generally low self-care agency, suggesting that these clusters need further support. It also identified groups with markedly low stress-coping ability or ability to make the most of the support available, indicating that support focusing on mental and social support may be necessary.
Accordingly, it was suggested that consideration of a support system for people with diabetes based on the characterization of each cluster may lead to more efficient and effective assistance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Grant-in-Aid for Scientific Research (KAKENHI 19599013, 16H05575).