
Abstract
Keywords
Introduction
This article aims to contribute to our knowledge on how middle managers understand policy changes and imposed innovation in home care services. Middle managers' understanding of these phenomena is of particular interest due to their position in between top management and the front line. Middle managers in public organizations must handle a variety of interests and dilemmas, for example, the conflict between economic rationality and the rationality of care (Gunnarsdóttir, 2016). Innovation can be defined as “an intentional and proactive process that involves the generation and practical adaption and spread of new ideas, which aim to produce a qualitative change in a specific context” (Sørensen & Torfing, 2011, p. 849). In Norway, the municipalities are currently the welfare state's most important institutions (Teigen, Ringholm, & Aarsæther, 2013). The municipalities are important providers of welfare services in the health-care sector. Ambitions of making Norwegian municipalities more innovative are complex, as the aim is to further develop the municipal services, improve organizational solutions, engage local business and community development, and furthermore create schemes that strengthen democracy (Ringholm, 2013). In line with Saari, Lehtonen, and Toivonen (2015), we acknowledge that there is a problem for managers to match public policy and programs to new practices at the local level. Middle managers in municipalities are considered to play important roles in innovation processes due to their positions as mediators between top management and the front-line workers. Considered the policy changes and imposed innovations in the municipal health-care sector, the research question was as follows: “What can middle managers' stories of imposed innovation tell us about their role in, and some important prerequisites for, innovation processes in municipal health-care services?” Thus, our objectives are twofold: We aim to expand the understanding of middle managers' role in processes of imposed innovations in municipal health-care services and to pinpoint some main prerequisites for such processes.
A study by Birken, Lee, Weiner, Chin, and Schaefer (2013, p. 30) encourage health-care researchers to look at the influence of middle managers on innovation and suggests that health professionals can promote efficiency by employing proactive middle managers. The managers in this study come from health-care services and form communities of both practice and narratives. They share common ground in terms of the services they offer the municipal residents as well as in their stories and the boundaries of participation in a practice. These stories and boundaries offer both difficulties and possibilities when facing challenges or other disciplines (Mørk, Hoholm, Ellingsen, Edwin, & Aanestad, 2010). According to Wenger (2000), cross-disciplinary projects confront people with problems that are outside the realm of their competence but that force them to negotiate their own competence with the competence of others. Mørk et al. (2010) underline that negotiating is an important aspect of practice. Negotiating in a cross-disciplinary working environment was relevant for the informants in our study, and the services were under pressure to cut the budget. A report on differences in the health-care sector in a selection of Norwegian municipalities (Tromso kommune, 2018) pointed out that the threshold for home services was high in the managers' municipality, and there was too little attention to early efforts and prevention. This report resulted in a greater need for long-term services for all age groups, which led to increased resource utilization and higher department costs. A high level of resource utilization in the care and welfare sector led to political decisions to cut NOK 200 million in health services within the next few years. There was a need for innovations in an already pressured health sector. Following Birken et al. (2013), we agree that middle managers have a potentially important yet poorly understood role in health-care innovation. In a literature review of 181 studies of public innovation, De Vries, Bekkers, and Tummers (2016) find that the main emphasis of the studies is qualitative. However, none of the studies mentioned in De Vries' work make use of narrative theory and method. Through a narrative context analysis of middle managers' stories about policy changes and imposed innovation, we want to contribute to the understanding of the necessary conditions for changes in home care services. This underline a research gap on narrative studies on middle managers' stories of innovation in health-care services.
The structure of the remaining part of this article is as follows: First, we describe a selection of research on public innovations and middle managers. Second, we present two dominant discourses on innovation in health-care services. Furthermore, in the “Methods” section, we describe middle managers, thematic analysis, and the interviews. Next, we analyze the stories. We interpret these stories to be related to dominant discourses on innovation at the macro, meso, and micro levels within the storytelling contexts. After the discussion, we reflect on the study's implications for practice. We focus on the practice of negotiating in cross-disciplinary environments at all levels in the organization, before we present the conclusion.
Research on Public Innovation and Middle Managers
Previous research on innovation in the public health sector has been rated inadequate in terms of understanding how innovation takes place in a public-sector context, including public health care (Fuglsang & Rønning, 2014; Karlsson, Skålén, & Sundström, 2014). Likewise, research on the role of middle managers and organizational change processes has yielded no dominant theoretical approach (Gatenby, Rees, Truss, Alfes, & Soane, 2015; Harding, Lee, & Ford, 2014). Although societal development in the 19th and 20th centuries first and foremost was driven by technological progress and economic dogmas, the time is now seen to be ripe for innovation related to societal and systemic changes (Grimm, Fox, Baines, & Albertson, 2013). The term social innovation expresses discontent with innovation, as it was formerly known and with its ability to deliver sustainable outcomes (Ziegler, 2017). De Vries et al. (2016) call for future research that explains the actual impacts of innovations, and they see a need for a wider range of methods in innovation studies. Studies that explicitly consider national culture and governance traditions are needed. According to De Vries et al. (2016), many scholars embrace the idea that innovation can contribute to improving the quality of public services and addressing societal challenges. The rationale for innovation in the public health sector is considered in several research strands that focus on improving productivity and efficiency, reducing costs, increasing quality and responsiveness, reducing variation in practice and increasing access to health services (Williams, 2011). In line with Williams (2011), we agree that innovation can be understood only in context. Middle managers have an important role in facilitating innovation in the local context. Employee-driven innovation can be defined as “the development and implementation of new organizational forms, service concepts, modes of operation, and service processes in which ideas, knowledge, time, and creativity of employees are actively used” (Høiland & Willumsen, 2018; Klitmüller, Lauring, & Christensen, 2007; referred by Wihlman et al. 2014, p. 162). In a study of the relationship between middle management resistance and adaptation strategies for centrally initiated change instructions and employee driven innovation, Høiland and Willumsen (2018) point out that the strategies can be conceptualized as value-based, resistance-driven innovation. This is a type of employee-driven innovation that arises as one by-product of resistance and adaptation, which creates value for the organization's core activities.
In the modern public health sector, middle managers, as mentioned, play crucial roles in the process of implementing changes. Their roles are those of the mediator, the go-between, positioned as they are between top management and the front-line service providers (Gunnarsdóttir, 2016). During organizational changes, such as policy changes or imposed innovations, they can experience pressure from both sides, and loyalty conflicts. Middle managers' reactions (and actions) when faced with directives of policy changes, or pressure for innovation, given from top management, seems to be a relevant and interesting topic for inquiry.
Two Dominant Discourses on Innovation in Health-Care Services
We have chosen to focus on two dominant discourses on innovation in health-care services. The first is related to the reform movement commonly referred to as new public management (NPM). The second is related to traditional gender structures in health-care professions. These discourses were chosen because they are central to the middle managers practices, and the discourses contribute in shaping their understanding and everyday activities.
NPM as a reform movement was introduced in Norwegian health care in the 1990s with a focus on development of the society as a process of bureaucratization. The model encompasses ideas from market economics and has influenced the health-care field in relation to documentation, quality control, competition, and user orientation (Christensen, 2018). The ideology of NPM implies that public resources are limited and need to be carefully rationed (Wrede & Henriksson, 2018). Public sector innovation has been linked to reform movements such as NPM (Alonso, Clifton, & Díaz-Fuentes, 2015). The relationship between NPM practices and public organizational performance is still an important issue, as governments continue to search for means of reducing public sector budgets in the ongoing crisis (R. Andrews & Van de Walle, 2013). According to Kristiansen (2016), NPM and market-based ideas are often added on top of existing practices in health care and create tensions in daily work.
The discourse on NPM as contrary to traditional health practices, with changes toward an increased number of managerial tasks distributed among professionals, is a culturally dominant narrative. Research that focuses on the effects of NPM ideas on health-care organization often underlines the contrast between new managerial tasks and traditional professional management (Allen, 2014; Kristiansen, 2016). NPM-inspired reforms are described as threatening because health professionals are being taken away from their true vocation (Kristiansen, 2016), which is patient care and coordination of patient care. Ethical aspects of nursing care are challenged by NPM-like reforms. Several studies (Allen, 2014; Numerato, Salvatore, & Fattore, 2012; Olsvold, 2012) focus on how NPM changes force nurses to alter their professional culture, identity, and autonomy. These studies explore how NPM-like reforms influence nursing work, professional identity, and health care in general (Kristiansen, 2016).
The second dominant discourse on innovation in health sector we have chosen to introduce is related to gender. The sector is dominated by women, not only in Nordic countries but also in the European Union (European Union Information Agency for Occupational Safety and Health, 2013). Demanding health and social care tasks are primarily carried out by women, often in low status professions (Vänje, 2015). The professionalization of care led to the fact that the female body became a tool for physical contact with patients, used, for example, to lift and touch patients (Vänje, 2015). Emotional commitment, care giving and heavy physical labor became central values within the profession. Throughout the years, this has also become a dominant narrative, as the values are seen as necessary for what is considered good health services, relying on the female body. The traditional gender structures and images still exist in the profession, with different effects on working life (Vänje, 2015). NPM development, with emphasis on the market economy, is understood as a more competitive-masculine value (Thomas & Davies, 2005). There is also a professional gender hierarchy in our study, with mostly female nurses and health professionals as middle managers and mostly men working in the municipal bureaucracy and management. In the material we have looked for signs of these dominant discourses in the middle managers stories and identified them as expressions of how the managers relate to their roles in imposed innovation processes.
Methods
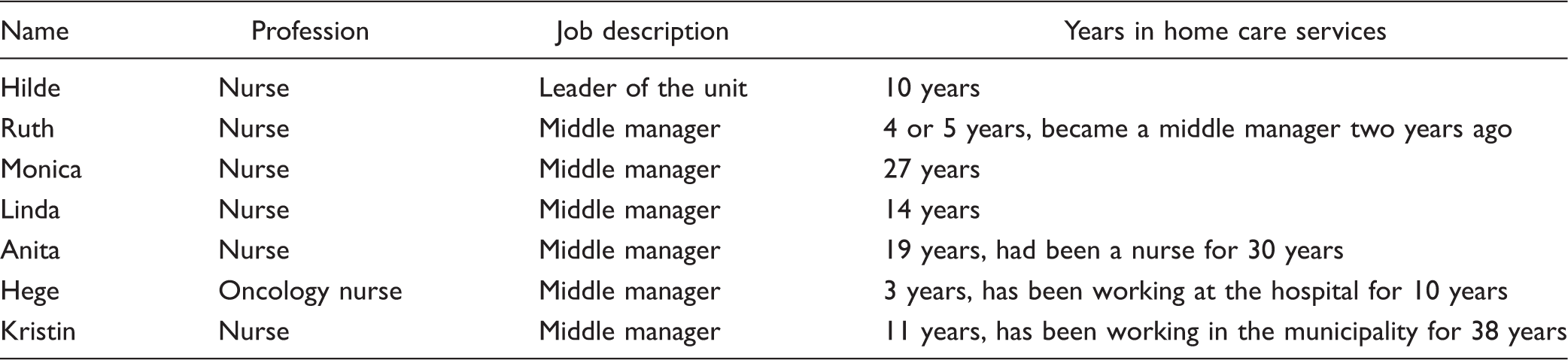
The interviews analyzed in this article have been conducted as part of a larger research project. The project was approved by the Norwegian Center for Research Data in 2017 and is a broad inquiry of innovation in health care and welfare services among 32 middle managers in two municipalities. The informants represent a multitude of experiences related to innovation. In this article, we analyze a selection of interviews with seven middle managers from a home care service department in a city municipality; an individual interview with a unit manager, and two focus group interviews with a total of six middle managers in the same service. The interviews lasted for approximately 60 to 90 minutes. There were three informants in both focus group interviews. We made this selection on the basis that these informants had many stories related to their unit on how they managed to deal with the limits of a tight budget. The care service also had low sick leave and little overtime among the employees. Neither did the unit use many temporary workers from the private sector. We wanted to investigate what made this department handle changes, apparently unproblematic.
The Middle Managers
The Middle Managers.
Thematic Analysis in Relation to Dominant Discourses
The empirical data are generated through qualitative interviews and has been analyzed using narrative theory. This analytical approach was chosen in accordance with our aim to look deeper into how stories about innovation can shed light on middle managers' roles in, and prerequisites for innovation. According to Gubrium (2005), stories are produced, distributed, and circulated in society. Understanding how stories relate to specific contexts requires an understanding of what those contexts do with words. The same story can have different meanings in different contexts (Klausen, Karlsson, Haugsgjerd, & Lorem, 2016). Narratives maintain and reproduce power relationships, but narratives also allow resistance to and change in such relationships (Sørly, 2017). Resistance stories always relate to dominant discourses and, within organization studies, everyday practice (Thomas & Davies, 2005). The stories told by our informants are understood and analyzed in relation to dominant discourses on innovation in health-care services. Discourses are blueprints that offer an identification of what is assumed to be a normative experience (M. Andrews, 2004). We understand the dominant discourses on innovation as intertwined with the managers' stories. Traditions, beliefs, understandings, values, professional knowledge, cultural norms, and listening to others' stories related to innovation affect the stories our managers tell in the interview setting. The stories told are shaped to fit or resist against the dominant discourses on innovation, and both the interviewer and the interviewee draw upon a “cultural stock of knowledge” (Mishler, 1999, p. 10) of how innovations in municipal health care may affect the health professionals' working day.
We have chosen to do a thematic analysis, with emphasis on what was said, rather than how it was said (Klausen et al., 2016). We created themes by assessing whether an opinion was expressed in the data material that was central to understanding the managers' experiences of the policy changes affecting their workplace. In line with Riessman (2008), we performed an experience-oriented thematic analysis, working with a single interview at a time and isolating and ordering relevant excerpts into different themes. After doing this with the interviews, we sharpened focus and attempted to identify four common themes. We found themes that captured something important about the data and that represented a meaning (Braun & Clarke, 2006). The excerpts are representations of the different themes. By interpreting innovation in relation to dominant discourses at the micro, meso, and macro levels within the storytelling contexts, new understandings can reach the surface. The micro level is related to the intersubjective sphere, which is the immediate relationship and interaction that occurs in the interview context (Klausen, Haugsgjerd, & Lorem, 2013; Zilber, Tuval-Mashiach, & Lieblich, 2008). The meso level is the social field, related to the sociohistorical context in which life is lived (Klausen et al., 2013). In this article, this level includes the relation between the middle managers and other employees or other disciplines. The macro level includes larger, cultural metanarratives that “reflect cultural themes and beliefs that provide a local story with coherence and legitimacy” (Zilber et al., 2008, p. 1054).
The Interviews
We analyze the stories from one department that dealt with the limits of a tight budget in the municipality. The imposed innovations in the unit seemed to be transformed to value-motivated resistance-driven innovation from a ground level that included the employees in the process (Høiland & Willumsen, 2018). We wanted to investigate how the managers' stories related to policy changes and imposed innovations. In the following, we will present four different stories. These stories tell us about the managers' experiences of innovation in their everyday working life. The narratives do not tell a clear story but shed a light on the experienced challenges of imposed innovation among the middle managers.
Results: Stories of Policy Changes and Innovation
During the interviews, it became clear that the women considered municipal projects as “a line of fatigue syndrome” 1 and imposed innovations as a troublesome burden that created alienation among the employees. The budget cuts meant new changes, with expectations for more effective service. When the gap between demand and supply in health care appears set to grow wider, budget holders are required to find innovative ways to allocate dwindling resources and make savings while preserving standards of care (Williams, 2011). Innovations are nonlinear processes in which negotiations of interests play a crucial role (Mørk et al., 2010). The seven nurses in the home care service department questioned the municipality's policy changes and said that they felt that their effectiveness and effort were weighed and measured in economic terms. The managers said that the municipality continued with ever new innovations, but they rarely lasted long, and evaluations were not carried out. The leader of the department said, “It feels like you're being taken by a wind that passes by.” The middle managers all related their stories to the two dominant discourses we have identified; the dominant discourse on innovation as NPM demands in practice and to traditional gender structures in health-care professions. A masculine-oriented universe on the top-level management was considered a threat to the middle managers' professional autonomy. Despite this, the data show that they both reject and accept innovations. Through the analysis, we found that the nurses emphasize that certain prerequisites must exist in the organization to introduce innovations while retaining a good health service. The stories told are filled with ambiguity. The nurses are balancing between good care and expectations of innovations from the policy makers. Four themes were derived from the analyses to provide descriptive accounts of the richness, breadth, and complexity of the managers' experiences of being exposed to continuous change in their everyday working life. By presenting excerpts from the interviews, followed by interpretation in relation to dominant discourses on innovation at the micro, meso, and macro levels within the storytelling contexts, we offer knowledge on the middle managers' reaction to government imposed “innovations,” i.e. policy changes.
Theme 1: Trust-Based Management; “There Is an Acceptance for Both Praise and Criticism”
The nurses spoke about the importance of having a leader that “kept the door to the office open” and let everyone operate and lead as they want in their zone. The department had staff meetings every second week and “everybody knew everybody.” One of the middle managers, who had been working as a nurse for 14 years, reported that trust-based management was very important: It is important with a close management; we middle managers are present and participate in the daily report; we are present at the morning report and the report in the middle of the day. We do not have the time to be out with the patients, but we catch up with what the employees want and get to know them well. […] Close management … we see it immediately, if there is something going on, we get much feedback [from the employees] that is how we lead our zones; that it feels safe and secure, they [the employees] dare to ask questions. It is all about stability, continuity and predictability. We nurses are good examples. We talk about being good examples. There is an acceptance for both praise and criticism. If you [an employee] have done something wrong, you discuss it with your middle manager; do you want your middle manager or a colleague to write a deviation notification. Deviation notifications can be written by a colleague, too. We have discussed the basic values in appraisals; they [the employees] have a great trust in management, both in the leader of the department and in us [the middle managers].
Theme 2: Flexibility and Dynamics: “We Work as a Zipper Function”
An important value is the ability to take care of patients and perform good services. One of the managers, a nurse for 30 years and a middle manager for 19 years, told about the flexibility at the department: We [the middle managers] are “self-propelled” workers. We work as a zipper function, and we have to be flexible. New changes have come into our home care services; the patients are written out of the hospital earlier, when they still are in need of nursing services, and we can take care of them. There is a lot of community spirit going on, across the zones … We work across the zones, when another [middle manager] needs help in a zone, we help her, and they help us when we are in need. We use one another like that often. Parts of the specialist services are moved out of the hospital, out to the patients … The allocation office at the hospital must send patients home earlier. The office has made calculations; 3 minutes to give medicine … they have calculated how long a time we should use on each patient … I just borrowed a nurse assistant during daytime in my zone, I have borrowed three shifts this month, and then X [name of another middle manager] comes and asks me, how should we solve this? When I have few hours with the patients, I might have red numbers in my budget … I think this exchange is culture and practice! I wonder why they [management in the municipality] have not asked us how we manage this—that is so Law of Jante!
2
That is unbelievable.
Theme 3: Continuity of Care: “We Need Our Heads and Hands”
The informants in our study emphasized the importance of continuity of care. It was in the best interest for the organization, the employees, and the patients to have full-time employment stability. The leading middle manager clarified that this had been a targeted investment in her department for the last 10 years. Full-time employment was prioritized: We have a lot of full-time employment. There are many full-time positions. We have made special agreements so that the employees should get a higher pay rate. We need our heads and hands … We need safe leaders, with the right personality and experience to fulfill their role … We have diversity and complexity in our service tasks, both as leaders and among the employees … We need to delegate responsibility, and trust is a key word … We have a philosophy in the department; to take good care of our employees. Low sick leave is due to well-being at work. We don't need anybody from outside to tell us that. It is the culture, the people, the attitudes; what we talk about in the department means a lot. What it is that makes us like our work; humor is important, to dare to take up things, most people are seen, this is reflected on the top [of the organization], we laugh a lot. We are few men. We can sit around the table, we can say “life is good.” Our organization does have a gender perspective. It is men that have invented the resource base [an arrangement where the measures in the services are to be decided by a central team and not locally in the individual department]; it take us away from close leadership. We are a woman-dominated profession: the organization of our services is central.
Theme 4: Emphasis on Competence: “We Are Met With Silence”
The leading middle manager in the department underlined the importance of having nurses as middle managers in every zone: We have nurses in every zone. There are specialized nurses, nurses, and health professionals. (…) We move between the formal and the informal. It is important to build good relations and stick to the frame instead of details. We need safe middle managers, with personality, experience on how to perform their role … Middle managers need certain characteristics. They have to dare. And they must support each other. People have had the opportunity to continue their education and take courses. Our department has converted positions from assistant nurses to nurses. When we attend meetings with the management in the municipality and we talk about this, we are met with silence … Where does the good [working] culture stop? The municipality management often has big training days for the employees, where some people from the south come and present a model. We are often placed in groups to find the right answers, often we think “but we have done this ourselves.”
On a macro level, the managers' stories on competence are not only a rejection of the municipal management but also an acceptance of the need for order and structure within the department. According to Olsvold (2012), nurses contribute to care services not only through having direct contact with patients but also through coordinating, planning, communicating, mobilizing, organizing action, finding available resources, taking responsibility, and facilitating handovers. Nurses play a key role in health-care services, and the informants in our study are no exception.
Discussion
According to Williams (2011), we need to account for the complexity of innovations and the specific contexts where they belong and acknowledge and identify strategies for local decision makers and organizations to recognize the reality of resource scarcity in health care. The managers expressed resistance narratives toward the policy changes, which was seen as an extension of the NPM movement. Budget cuts represented expectations to manage the home care service department more efficiently and cost-effectively, while the middle managers could not see the reason for the expected changes, as their department was not in financial deficit. Middle managers draw on the learning they have gained through daily interaction with their employees and the service users to nurture service innovation (Karlsson et al., 2014). The four themes in our article are understood as prerequisites for innovation in the service. The middle managers underline trust, flexibility and dynamics, continuity among employees, and competence as necessary frames for the organization. There are still local and contextual challenges related to all these themes; the close leadership related to trust is being challenged by other structural solutions related to NPM values. These values are also understood by our informants as gendered values; the municipality management is compared to a male culture that does not understand the philosophy of care and nursing. This is shown in a middle manager's story stating that when they share their organizational solutions at municipality meetings, they are met with silence. Hence, we can understand these resistance stories as stories targeting not only NPM values but also “male-valued management.” The female community, among the interviewees, is interpreted as a community of care. Although the women accept certain municipal regulations, they build their organization on nursing values related to patient care and the coordination of patient care. Other challenges related to communities of practice are professional identity and power. Power can be understood as productive, both producing and being produced by social and material relations (Mørk et al., 2010). Power can also be described as layers of a framework; the first layer is decision-making power, the second layer is processes of restricting and extending access to decision making, and the third is how interest groups manage meaning and shape a legitimate agenda. A fourth layer is within the organizational system that everyone takes for granted (Mørk et al., 2010). Mørk et al. (2010) add a fifth layer—the uncertainty of change in potential futures as grounds for negotiation. Lave and Wenger (1991) underline the importance of looking at the social structure of practice and its embedded power relations. Many of the managers in this study were nurses, who seemed to share a common view on power relations and professional understanding. It is unknown whether a professional conspiracy might have caused innovations to fail to be translated into practice because they cross professional boundaries and do not align well with these managers' nursing practice (Newell, Robertson, & Swan, 2006; Robertson, 2007). The stories analyzed show that nurses are defending their competence and practice. In a deinstitutionalization period within health services, the nurses claim that the municipality need them to be able to meet the patients who come home earlier from the hospital. The “male-valued management” must negotiate its reforms and expectations and work in dialogue with the local departments.
Implications for Practice: Negotiating at All Levels in the Organization
The primary issue is to create municipal innovations in the health sector that acknowledge and appreciate the work of health professionals and achieve what is best for the patients. The health professionals' values related to their mission as care givers must be taken into consideration, and the municipal management should create a negotiating, cross-disciplinary practice in cooperation with the units, the patients, and their relatives. The municipal management must negotiate values, ethical standards, and budget expectations with the different departments. This dynamic is in accordance with the uncertainty of change from potential futures as grounds for negotiation (Mørk et al., 2010). The health-care sector in welfare states is in constant change, and it is time to change the services and their municipal management in favor of what is best for the help-seeking population. It is time to create a negotiating, flexible culture at all levels of the organization where high-quality services characterize the sector.
Conclusions
In this article, we aimed to answer what middle managers' stories of imposed innovation can tell us about their role in, and some important prerequisites for, innovation processes in municipal health-care services. In the modern public health sector, middle managers play crucial roles in the process of implementing changes. In line with Gunnarsdóttir (2016), we see the roles of the middle managers as of the mediator, the go-between, positioned between top management and the front-line service providers. The main finding in this study is the development of an understanding of which frameworks are required within a home care service to meet constant demands for innovation. We find the prerequisites for implementing innovations to be (1) trust-based management, (2) flexibility and dynamics, (3) continuity of care, and (4) emphasis on competence. These prerequisites are necessary to treat imposed innovation as something more than just a troublesome burden that led to more pressure in an already pressed service. Nevertheless, the managers responded to the expectations of innovation by facilitating certain changes to their units. These changes were not always what the system expected; they were adapted to the practical everyday life at the unit. Some prerequisites had to be in place for innovation. These were important organizing factors for each unit. In agreement with Høiland and Willumsen (2018), we understand the strategies used by the middle managers in this study as value-based, resistance-driven innovation. The employee-driven innovation arose as one by-product of resistance and adaptation, which creates value for the organization's core activities. The loyalty to the system and the municipal management seemed to outweigh the disadvantages of changes.
Footnotes
Acknowledgments
The authors wish to express their sincere gratitude to all the managers who shared their time, experiences, and thoughts so generously with them. The authors also acknowledge the contribution of the participants. The authors would also like to thank the reviewers, as well as the editor, for good comments on previous versions of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The article is written on the basis of data from the project “KOMII—Municipal Innovation Management and Innovation Culture,” funded by the Regional Research Fund North, Norway.