
Abstract
Purpose
To develop a linguistically and psychometrically validated Thai version of the Simplified Diabetes Knowledge Scale (T-SDKS) for adults with Type 2 diabetes mellitus (T2DM).
Design
A cross-sectional study was carried out among people with T2DM.
Methods
Consecutive sampling was undertaken to recruit participants at the outpatient diabetes clinic of a hospital in Northern Thailand.
Results
A total of 502 patients with T2DM were recruited. The mean age of the participants was 60.2 years, and 60.5% were female. The T-SDKS attained a reliability coefficient of .79. The item-total correlation value was greater than 0.20 for each item, and the inter-item correlation ranged between 0.03 and 0.49. Respondents attained a mean percentage knowledge score of 42.39% ± 15.45 on T-SDKS.
Discussion/conclusions
The T-SDKS has demonstrated to be a brief and simple diabetes knowledge assessment tool to use in a busy clinical setting.
Implication for practice
The findings can be used to improve health education interventions.
Introduction
An increasing prevalence of diabetes has been reported worldwide (Meetoo, 2014; Selvin, Parrinello, Sacks, & Coresh, 2014). In the United States, Selvin et al. (2014) found that the prevalence of diabetes among older adults had risen from 5.8% in 1988–1994 to 12.4% in 2005–2010. In Canada, Greiver et al. (2014) estimated the population prevalence of diabetes to be 7.6%. There is also an increasing prevalence of diabetes in developing countries (Whiting, Guariguata, Weil, & Shaw, 2011). Thailand is a developing country which is facing the problem of undiagnosed and late treatment of diabetes mellitus. Approximately 7.5% of the Thai population have been diagnosed with diabetes, and an additional 35.4% of the population have impaired fasting blood glucose levels (Aekplakorn, 2011). Although diabetes is common in Thailand, more than half of the population remain undiagnosed and hence may lack diabetes knowledge for self-management (Gakidou et al., 2011).
Research has demonstrated that knowledge about the disease, medications, diet, glucose monitoring, and foot care is essential for self-care management among people with diabetes (Ajala, English, & Pinkney, 2013; Desalu et al., 2011; Dorresteijn, Kriegsman, Assendelft, & Valk, 2012; Nemcova & Hlinkova, 2013; Rodbard, 2016). In a study undertaken on 307 participants in India with Type 2 diabetes mellitus (T2DM) and a mean age of 55.6 years, only 23.8% had good knowledge of diabetes and its management (Chavan et al., 2015). Another study undertaken on 515 patients in Bangladesh reported that 45.6% participants with T2DM had good knowledge of diabetes (Islam et al., 2015). The evidence also indicated that having knowledge was significantly associated with compliance to medication, nonpharmacological management (Chavan et al., 2015), and glycemic control (Islam et al., 2015).
Knowledge can empower self-management; hence, the assessment of diabetes knowledge is a fundamental aspect of diabetes care and assists in providing individualized diabetes education (Nemcova & Hlinkova, 2013). Despite the importance of knowledge for self-management, there are few reliable and valid questionnaires that measure diabetes knowledge, particularly in the Thai language which can be used in the busy clinical setting.
The 20-item Simplified Diabetes Knowledge Scale (SDKS; Collins, Mughal, Barnett, Fitzgerald, & Lloyd, 2011) developed from the Michigan Diabetes Knowledge Scale (Fitzgerald, 1998) has been extensively used to measure knowledge about diabetes. The SDKS consists of 20 items pertaining to diet, risk factors, and self-management. The patient is required to provide a yes or no response to each item. A high score of correct answers indicates high knowledge of diabetes. The internal reliability (Cronbach’s α) for the SDKS ranged from .69 to .71 (Collins et al., 2011).
Given that a Thai version of the scale has not been developed, the aim of this study was to develop a linguistically and psychometrically validated Thai version of the SDKS (T-SDKS) for adults with T2DM.
Methods
Instrument
Development of the T-SDKS
Permission to translate the SDKS (English version) was obtained from the instrument developers. The SDKS was translated according to the World Health Organization (2016) procedure for translation and adaptation of instruments. First, forward translation was undertaken by translating the scale from English to the Thai language to produce a version that was semantically and conceptually as close as possible to the original version. The translation was done independently by two people. The first person was a translator who was bilingual (English and Thai) and the second a Thai health professional who was familiar with the technical terms and had experience with translation from Thai to English. Second, an expert panel comprising a nutritionist and questionnaire development expert reviewed the primary version and compared it with the original version; changes were then made if required. The third step involved back translation of the Thai version of the questionnaire to English. This was undertaken independently by two bilingual Thai nurses. Both nurses had more than 20 years of nursing experience. The translated English version and the original English version were then compared to identify any discrepancies. The Thai version of the instrument was called the T-SDKS.
Pilot testing the T-SDKS
Pilot testing of the T-SDKS was undertaken on 30 Thai patients with T2DM who attended the diabetes clinic in the 2 weeks preceding the commencement of data collection. The T-SDKS was completed by 30 patients in a one-to-one interview with the researcher. In addition, the researcher asked the patients if the words or expressions in the T-SDKS were easy to understand, relevant, and did not cause offense. The researcher made notes of all the comments made by the patients. When comments were received from participants, the item was discussed with the expert panel who were involved in translation, and the panel provided recommendations for linguistic improvement. After the expert panel agreed on all the linguistic improvements, the final version of the T-SDKS was obtained for psychometric evaluation. In pilot testing, the overall self-administration for the T-SDKS questionnaire took on average 10 minutes to complete. Pilot testing of the T-SDKS was included in the institutional review board approval procedures for the larger study. Data from pilot testing were not included in the final analysis.
Study design, sample, and setting
Recruitment for the study was undertaken between September 13, 2016, and November 13, 2016. A consecutive sample of patients attending the outpatient diabetes clinic at a large urban teaching hospital in Northern Thailand were recruited to the study. This hospital provides health services to both rural and urban patients in the region. The inclusion criteria were patients aged more than 18 years old, people attending the outpatient diabetes clinic, and people diagnosed with T2DM and willingness to participate in the study. People who were unable to communicate in Thai were excluded.
Data collection
Information about the study was provided by an assistant researcher at the diabetes outpatient clinic. Written consent was obtained from all participants who were willing to participate in the study. The questionnaire was then distributed to participants. The questionnaire consisted of three parts which included data on demographics (age, gender, and education), clinical characteristics (diabetes duration, HbA1C, body mass index [BMI], and diabetes therapy), and knowledge of diabetes. Data on clinical characteristics (up to 6 months) were collected from the medical records. For those willing to participate but could not complete the questionnaire by themselves, a face-to-face interview was conducted to complete the survey. All interviewers were trained by the principle researcher and the interview took approximately 10 minutes.
Data analysis
Validity
Validity is a key criterion for evaluating how well an instrument measures what it is intended to measure. Face validity is used to measure how relevant, credible, and acceptable the instrument is following the translation process (Polit & Beck, 2012). An expert panel assessed the face validity of the translated T-SDKS. To ensure content validity, Thai clinicians and a dietitian reviewed the final Thai version of the instrument to assess its relevance, appropriateness, clarity, and comprehensiveness within the Thai context. They completed an open-ended questionnaire that explored the comprehensiveness of the T-SDKS, ease of understanding and completion, length of time taken to complete the instrument, and any other issues.
All data were entered into Survey Monkey© and exported to SPSS version 21.1 for analysis. Categorical data were presented as percentages, and continuous data were presented as means and standard deviation. Item-total correlations were used for testing the hypothesis construct total and then correlating the items with the total. Items with scores lower than 0.20 demonstrate weak correlation and are usually removed from a scale during development (Streiner & Norman, 2003). Also, the inter-item correlation was employed for testing the correlation in each item. The inter-item correlation value in the range between 0.30 and 0.70 but not over 0.8 was considered acceptable (Polit & Beck, 2012).
Internal consistency
Internal consistency was used to assess the reliability of the T-SDKS. Internal consistency is a measure of the degree of correlation between the items in the instrument. It has been established that the items should correlate moderately with each other and should contribute independently to the overall score. A perfect correlation of 1.0 indicates that the questions are measuring an identical construct. Hence, the interitem correlation value in the range between 0.30 and 0.70 but not over 0.8 was considered acceptable (Polit & Beck, 2012). The items were also examined for homogeneity of content using the corrected item-total correlations. Items with scores lower than 0.20 demonstrate weak correlation and are usually removed from a scale during development (Streiner & Norman, 2003). Although the responses to the items in the T-SDKS were binary (Yes or No), Cronbach’s α has been reported to be suitable to establish the reliability of the instrument (Sharma, 2016). Hence, the internal consistency was evaluated using the standard Cronbach α coefficient. The guideline by Tavakol and Dennick (2011) was used to determine the values greater than or equal to 0.9 that were considered as excellent, 0.8 to −<0.9 good, 0.7 to −<0.8 acceptable, 0.6 to −<0.7 questionable, 0.5 to −<0.6 poor, and less than 0.5 unacceptable.
Ethical consideration
Participants provided informed written consent before participating in this study. This study was approved by the Human Research Ethics Committee of both the University of Wollongong (HE16/209) and Uttaradit Hospital, Thailand (21/2016).
Results
Linguistic Validation
Comparison of the original version and the back-translation of the SDKS identified two items that required modification in order to be suitable within the Thai context. Some words that were not related to Thai culture were changed. Item 3 originally asked: “A pound of chicken has more carbohydrate in it than a pound of potatoes.” This was changed to “500 grams of chicken has more carbohydrate in it than 500 grams of rice.” The word potatoes was changed to rice as rice is the staple food of the Thai people and pound was changed to gram as it is the metric unit for measurement commonly used in Thailand. In Item 8, olive oil was changed to rice bran oil because olive oil is not commonly used in the Thai context.
Demographics and Clinical Characteristics (n = 502).

Note. HbA1c = glycosylated hemoglobin A1c.
Reliability
Thai Version of Simplified Diabetes Knowledge Scale (T-SDKS) Item and Reliability Analysis.
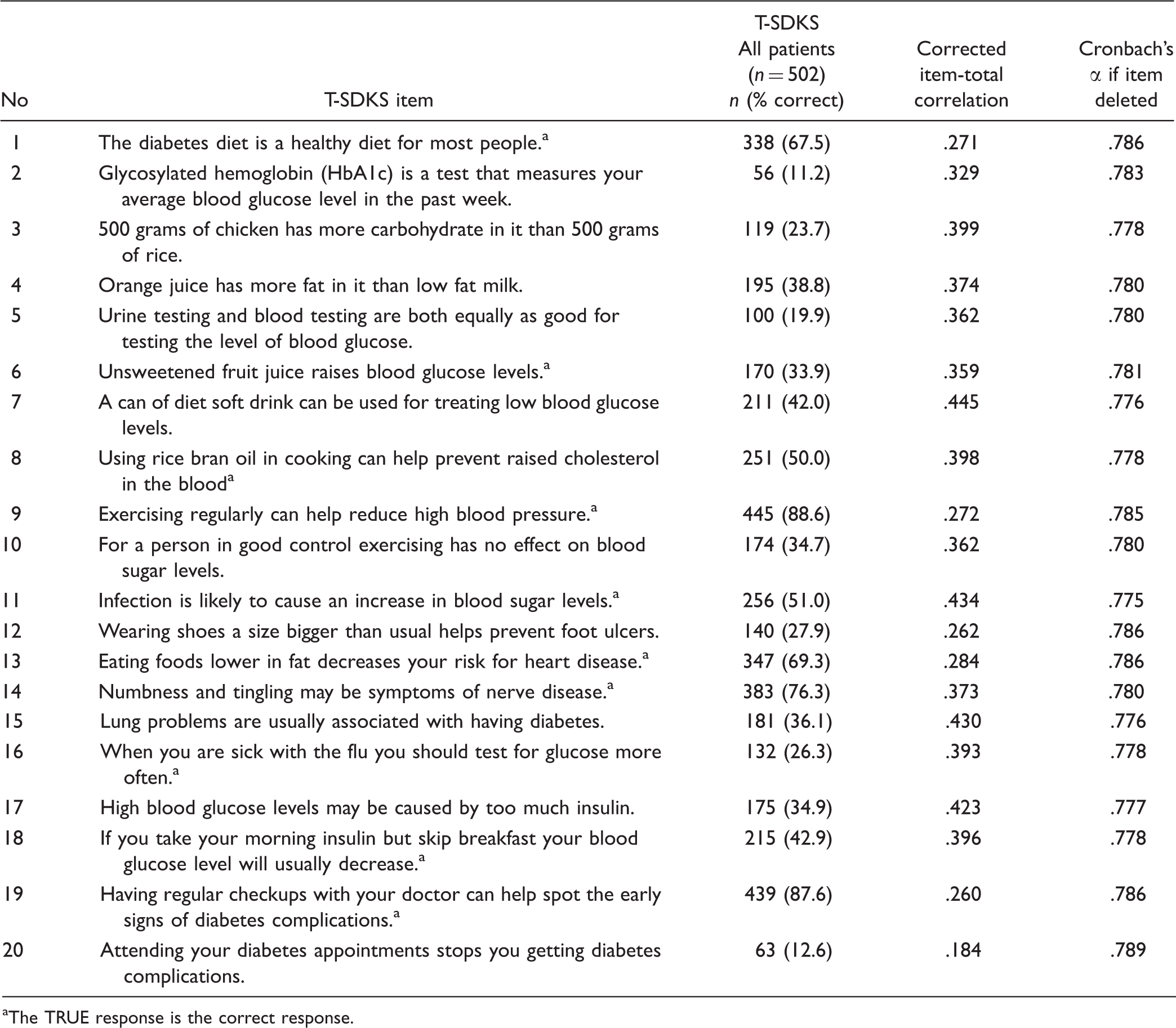
The TRUE response is the correct response.
inter-item Correlation Matrix.

Knowledge Related to Diabetes Known Groups Validity
Overall, the mean percentage of correct answers on the T-SDKS was 42.39% ± 15.45. The questions which patients answered correctly were about knowledge related to high blood pressure (88.7%), numbness and tingling (75.7%), and regular checkups (87.8%). In contrast, only 11.3%, 12.8%, and 20.6% of participants had knowledge about glycosylated hemoglobin (HbA1c) levels, attendance at clinic appointments, and testing blood glucose (Table 2).
Discussion
The aim of this study was to develop a linguistically and psychometrically validated T-SDKS for adults with T2DM. The major strength of the study was the rigor in which the instrument was translated and validated. Forward and backward translation was undertaken according to the World Health Organization guidelines. Validation was undertaken using expert, independent translators, discussion with an expert panel, and interviews with patients. The content validity phase indicated that in order to be consistent with the Thai culture, some items required modification as simply translating and using a questionnaire in another linguistic context is not appropriate (Wang, Lee, & Fetzer, 2006). Hence, the unit of the measurement in Item 3 was changed from pounds to grams which is the metric system commonly used in Thailand. In addition, as most of the Thai people eat rice as a main meal (Aekplakorn et al., 2015), a pound of potatoes was changed into 500 grams of rice, and olive oil was changed to rice bran oil (Item 8). These changes were made following extensive discussions with Thai dietitians and the research team. The large sample size was another strength of the study which enabled psychometric evaluation of the T-SDKS.
Measurement of reliability showed acceptable (Cronbach α = .79) results for the T-SDKS (Tavakol & Dennick, 2011). This is similar to the original SDKS English version (Collins et al., 2011).
Item 9 related to high blood pressure had the highest percentage (88.6%) of correct responses. The results obtained in this study are lower than other studies (Collins et al., 2011) where a larger percentage of people (96%) had the correct answers. The majority of the participants in this study had high levels of knowledge related to high blood pressure (88.6%), numbness and tingling (76.3%), and regular checkups (87.6%) which is not congruent with other studies. In the study by Collins et al. (2011), the majority of the participants had knowledge related to diabetes diet (96%) and foods low in fat (95%). These results could be due to the extensive prevention and awareness programs conducted in the United Kingdom (Collins et al., 2011) and indicate that some of these programs are not being conducted in the Thai context where our study was undertaken.
The results obtained in our study about knowledge of high blood pressure and need for regular checkups could be due to the fact that a large proportion of people in Thailand have high blood pressure (Aekplakorn, 2011). It is possible that participants in our study had received education about blood pressure management during routine visits to the general practitioner.
Low levels of knowledge were demonstrated in the following items: glycosylated hemoglobin (HbA1c; 11.2%), testing blood glucose (19.9%), and clinic appointments (12.6%; Table 2). This low level of knowledge could be due to the fact that the majority of the participants had only primary education (65.73% of all participants) which could also affect their health literacy levels as there is a strong association between educational attainment and health literacy (Wannasirikul, Termsirikulchai, Sujirarat, Benjakul, & Tanasugarn, 2016). It could be postulated that the participants had a caregiver looking after them who had knowledge related to diabetes; but as this was not investigated in this study, it would require further investigation. Given the low literacy levels, strategies such as audiovisual aids could be used to supplement education to people with T2DM in the Thai setting. The T-SDKS takes less than 10 minutes to complete and can be used in busy clinical clinic settings to identify patients with limited knowledge in order to provide targeted health education interventions.
Despite the strengths of the study, the limitations of this study need to be considered. First, the sample was recruited using a convenience sample from a single center in Northern Thailand. Second, the majority of participants had only primary education which may have influenced their knowledge levels related to diabetes and, hence, caution needs to be used when generalizing the results to the wider Thai population. In addition, the author had to use interview techniques for some participants with low literacy levels which may have led to potential bias in data collection. Therefore, further well-designed research studies need to be undertaken to test the T-SDKS in a diverse sample of Thai people with T2DM. In addition, evaluation of the construct validity of the T-SDKS using a large sample is needed.
Further research is required to investigate whether the T-SDKS has comparable reliability and validity in this population group across other regions in Thailand.
Conclusion
The simplified (true or false) version of the T-SDKS provided an acceptable content validity and reliability for assessing diabetes knowledge in the Thai context. This instrument can be used as a diagnostic tool for targeted health education intervention in Thailand. The T-SDKS is a reasonably easy to use survey that measures general diabetes knowledge and also can be used in a busy clinical setting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.