
Abstract
Introduction
There is documented evidence pointing to the fact that there are numerous challenges with postoperative pain (POP) management globally. However, these challenges with POP management are more profound in developing countries.
Purpose
The purpose of this study is to examine the knowledge, attitude, and practices of nurses concerning POP management in four selected district hospitals in Ghana.
Methodology
A descriptive, cross-sectional survey was employed to evaluate nurse's knowledge, attitude, and practices pertaining to POP management. Multistaged sampling was used to draw the respondents. An adapted version of the Nurses Knowledge and Attitudes Survey Regarding Pain instrument was used to test the knowledge, attitude, and practices of nurses and midwives. Descriptive statistics were used to analyze the data in order to present quantitative descriptions of variables in this study.
Results
This study showed that nurses in the four district hospitals had knowledge deficits regarding POP management. Eighty-one representing 48% of nurses had low knowledge on POP management. An overwhelming majority of nurses (97.6%) relied on routinely rendered basic nursing skills to relieve POP and a few used pharmacological interventions. However, nurses had good attitudes toward POP management.
Conclusions
POP is ineffectively managed by nurses in district hospitals in Ghana. Nurses and midwives in Ghana need to adhere to best practices in POP management by increasing their theoretical and practical knowledge, so that there will be tangible positive change in POP management in Ghana.
Recommendations
Nurses must be empowered through continuous development programs to keep abreast with changing trends that pertain to POP management.
Background
Although the aim of the International Association for the Study of Pain (2018) is to translate the study of pain management into improved pain relief worldwide, postoperative pain (POP) continues to be an issue of concern in modern day surgical practice. Despite the availability of many preoperative, intraoperative, and postoperative interventions and management strategies for reducing and managing POP, most surgical patients still experience acute POP, of which less than half report adequate POP relief (Chou et al., 2016). POP has costly implications as it is associated with legal and ethical ramifications (Francis & Fitzpatrick, 2013). There is also documented evidence pointing to the fact that there are numerous challenges with POP management that is more profound in developing countries as a result of inadequate resource allocations for pain management (Kizza, Muliira, Kohi, & Nabirye, 2016; Murray & Retief, 2015; Woldehaimanot, Eshetie, & Kerie, 2014). Half the number of postoperative patients still report inadequate pain management despite efforts from worldwide authorities in creating awareness on the effects of inadequate POP management (Admassu, Hailekiros, & Abdissa, 2016; Albrecht et al., 2013; Chou et al., 2016; Fletcher et al., 2015; Kolvekar, Pilegaard, Ashley, Simon, & Grant, 2016; Lorentzen, Hermansen, & Botti, 2012). Inadequate assessment and documentation is attributed to the high incidence of acute pain experienced by patients. A study by Eder, Sloan, and Todd (2003) showed that documentation of pain subsequent to therapy was noted on only 39% of charts evaluated, and a pain scale was used only 19% of the time.
Empirical evidence has shown that there is need to relieve POP within a reasonable time frame because of its negative effects on clinical outcomes (Bruckenthal & Simpson, 2016; Francis & Fitzpatrick, 2013). Inadequately controlled pain negatively affects quality of life, function, and functional recovery (Kehlet, Jensen, & Woolf, 2006). Inadequately controlled pain can also lead to postsurgical complications and persistent postsurgical pain (Kehlet et al., 2006). Acute pain can lead to the development of chronic pain syndromes (Kehlet et al., 2006). Although it is common to expect some pain after surgery as part of the inflammatory process, POP must be minimized by the health-care team to ensure patient satisfaction and comfort (Meissner et al., 2015).
Literature Review
As cited in literature, ineffective or inappropriate POP management may affect the health system especially in these modern times when healthcare is a business and patient satisfaction is a key to sustaining the business (Glowacki, 2015; Macrae, 2008). Often, POP management is particularly challenging to assess and manage. This is because, accurate assessment of pain depends on patients' ability to describe or verbalize pain. Patients may not be able to describe their pain as they recover from the effects of anesthesia. It is also difficult to diagnose other discomforts that occur with surgical procedures such as having an intravenous line in situ (Pasero, 2009; Turk & Melzack, 2011). However, there are several effective assessment tools and therapeutic approaches for POP management that nurses can utilize (Aziato, Dedey, Marfo, Asamani, & Clegg-Lamptey, 2015; Chou et al., 2016; Hawker, Mian, Kendzerska, & French, 2011). These therapeutic approaches include increasing analgesic doses or adding other analgesics if behaviors indicating pain persist or increase, or if additional painful pathology or procedures occur (Pasero, 2009). In patients who are unresponsive, no change in behavior will be evident; therefore, the optimized analgesic doses should be continued (Pasero, 2009). Recent studies also suggest the use of an interdisciplinary pain team and multimodal regimens in many situations (Glowacki, 2015; McDaid et al., 2010). Thus, no surgical patient deserves to suffer unnecessarily.
Nurses play a vital role in POP management and therefore require thorough knowledge and skill in managing POP (Chatchumni, Namvongprom, Eriksson, & Mazaheri, 2016). In most health-care settings, nurses constitute the biggest population of the health workforce and have 24-hour direct contact with patients (World Health Organization, 2016). Consequently, nurses are well placed to manage pain in the postoperative setting and must ensure that their interventions are tailored to suit individual preferences and comfort. However, some previous studies in POP management identified suboptimal pain management practices among nurses which were attributed to nurses' professional culture, ward culture, inadequate requisite theoretical knowledge, lack of priority toward pain management, and lack of clarity on the evidence base for different pain management interventions (Eccleston, 2011; Twycross, 2007).
Successful pain management must be developed by nurses working in postoperative units (World Health Organization, 2016). Some previous studies have also indicated that POP management should involve caring, commitment, therapeutic communication, appropriate assessment, good knowledge, and use of evidence-based multimodal approaches as well as proper evaluation of interventions in the presence of other variables such as cultural factors (Abdalrahim, Majali, Stomberg, & Bergbom, 2011; Elshamy & Ramzy, 2011; Yüceer, 2011).
Interestingly, there are reports of lack of patient assessment, negative perceptions, poor documentation, and inappropriate use of analgesics as challenges to pain management by nurses worldwide (Masigati & Chilonga, 2014; White & Kehlet, 2010). Some authors have attributed increased nursing workloads, communication gaps, lack of knowledge on POP management, and organizational change issues as the possible barriers to effective POP management (Glowacki, 2015; Meissner et al., 2015; Subramanian, Allcock, James, & Lathlean, 2012). For effective and appropriate pain management after surgery, patients require a combination of treatment modalities. It has been shown that nurses rely on and use sparingly singular strategies to manage pain (McDonald, LaPorta, & Meadows-Oliver, 2007).
Pain management by nurses is widely researched in developed countries (Francis & Fitzpatrick, 2013; Schreiber et al., 2014; Wang & Tsai, 2010). However, in developing countries like Ghana, this phenomenon is not well understood due to dearth of research on the subject of POP management. Recently, Aziato and Adejumo (2013) conducted a qualitative study in Korle-Bu Teaching Hospital in Accra and discovered that there were major challenges affecting POP management in Ghana. These authors suggested that quantitative studies on POP management are urgently needed to give a complete understanding of the phenomenon. To the best of our knowledge, existing Ghanaian studies have been qualitative in nature, focused on other health professionals, and have explored pain in the larger teaching hospitals. This study examined the knowledge, attitude, and practices of nurses regarding POP nursing management in four selected district hospitals in Ghana.
Methods
Research Design
A descriptive, cross-sectional approach was used to evaluate nurses' knowledge, attitude, and practices pertaining to POP management. Multistaged sampling was used to draw the respondents. Descriptive statistics were used to analyze data.
Study Setting
Number of Nurses by Hospital.

Sample Size and Sampling Technique
Israel's (1992) method of determining sample size for small population was applied to arrive at a sample size of 194 nurses from a total population of 374 (at ±5% precision level with 95% confidence level and a p value of .05). In the first stage, stratified sampling was done.
The sample size for each of the hospitals (stratum) was then calculated using Israel's (1992) formula: f = n/N, where n is the sample size, N is the size of population, and f is the constant proportion.
Therefore, f = 194/375 = 0.52.
Site 1 = 45 × 0.52 = 23.40 = 23 nurses and midwives Site 2 = 95 × 0.52 = 49.4 = 49 nurses and midwives Site 3 = 88 × 0.52 = 45.76 = 46 nurses and midwives Site 4 = 146 × 0.52 = 75.92 = 76 nurses and midwives.
After determining the sample size for each facility (stratum), simple random selection was used to select respondents using the lottery method, to ensure equal chance of selection. Of the 194 surveys sent out, 168 respondents answered and returned questionnaire, and 26 questionnaires were not returned.
Inclusion and Exclusion Criteria
Nurses and midwives with a minimum qualification of a certificate from the Nursing and Midwifery Council of Ghana, who have practiced or nursed a surgical patient for at least 6 months or more and work in the selected hospitals were eligible to participate in the study. The exclusion criteria included staff otherwise referred to as “nurse” in the Ghanaian context, yet without the minimum qualification and not licensed to administer strong analgesia.
Instrument for Data Collection
An adapted version of the Nurses Knowledge and Attitudes Survey Regarding Pain (NKASRP; Ferrell & McCaffery, 2012) instrument was used to test the knowledge, attitude, and practices of nurses and midwives. The modified final instrument consisted of four parts. Part 1 sought Demographic Information. Part 2 was the Knowledge Scale and made up of 13 questions about pain management. Part 3 (Attitude Scale) was made up of a 3-point Likert Scale and consisted of 14 questions that asked respondents opinion on attitudinal statements. Part 4 (Practice Scale) was also made up of a 4-point Likert Scale and consisted of 27 items that asked respondents opinion on how often they utilized pain assessment tools (8) and other practice interventions (19). Multiple choice questions within original NKASRP instrument was modified into true or false questions to make it easier for respondents to complete. Some questions that were found in literature to be important in an African setting were added to the original NKASRP instrument. Case studies with subsequent questions in original instrument were also modified into a Likert scale for easy response. Cronbach's coefficient alpha was calculated for the various scales. The overall Cronbach's alpha coefficient was .869 which indicated that the instrument had an adequate internal consistency.
Data Collection Procedure
Institutional review board (IRB) approval was granted by the University of Cape Coast (UCC). Introductory letters from the UCC were sent to the institutions where the study was to be carried out. After determining the sample size for each facility (stratum), simple random selection was used to select respondents using the lottery method. Written consent was obtained from nurses who agreed to participate in the study. Respondents were met in a group and informed about the purpose of the study and its procedures. Data collection spanned 2 months from December 2013 to January 2014. Respondents who agreed to partake in the study were assured of confidentiality as they were required not to provide any form of identification on the questionnaire. Each of the questionnaires had an informed consent form attached for respondents to fill out before participation. Approximately, 45 minutes were spent on completing the questionnaire.
Data Analysis
Demographic Data of Respondents (n = 168).

Ethical Considerations
IRB approval was granted by the UCC. Introductory letters from the UCC were sent to the institutions where the study was to be carried out. IRB approval was obtained from only the UCC because the study sites had no IRBs. Research assistants signed consent for confidentiality and were trained to ensure protection of confidentiality of subject's information. Written consent was obtained from participants before the start of data collection. The questionnaire used to collect the data contained numbers and no names were used to identify participants.
Results
Demographic Data of Respondents
There were 79.8% respondents being females and 20.2% being males. The results revealed that 115 (68.5%) of respondents were aged 20 to 30 years. The results indicated cultural and ethnic diversity among the respondents. Majority of the respondents had diploma and certificate qualifications in nursing with a few respondents being degree holders. Majority (67.3%) were staff nurses and midwives while the remaining were nursing officers, principal nursing, and senior nursing officers. Most nurses had below 5 years surgical nursing experience (Table 2).
Knowledge of Nurses and Midwives on POP Management
Knowledge of POP Management (n = 168).

Note. POP
Attitudes of Respondents Toward POP Management
Attitudes of Respondents Toward POP Management (n = 168).

POP = postoperative pain.
Practices of Nurses on POP Management
With regard to management interventions, an overwhelming majority (97.6%) of the nurses said they provided clean, calm, and a well-ventilated ward environment postoperatively. Another highly effective intervention used by the nurses was the encouragement of early ambulation/exercise with analgesia. Here, as many as 97.0% claimed to have used this measure. About 73% and 25.6% of the respondents reported that they usually dressed, bandaged, splinted, and reinforced wound sites postoperatively. Most of these interventions mostly chosen by the nurses are among the basic treatments of POP by nurses globally.
Nursing Interventions Used in POP Management.
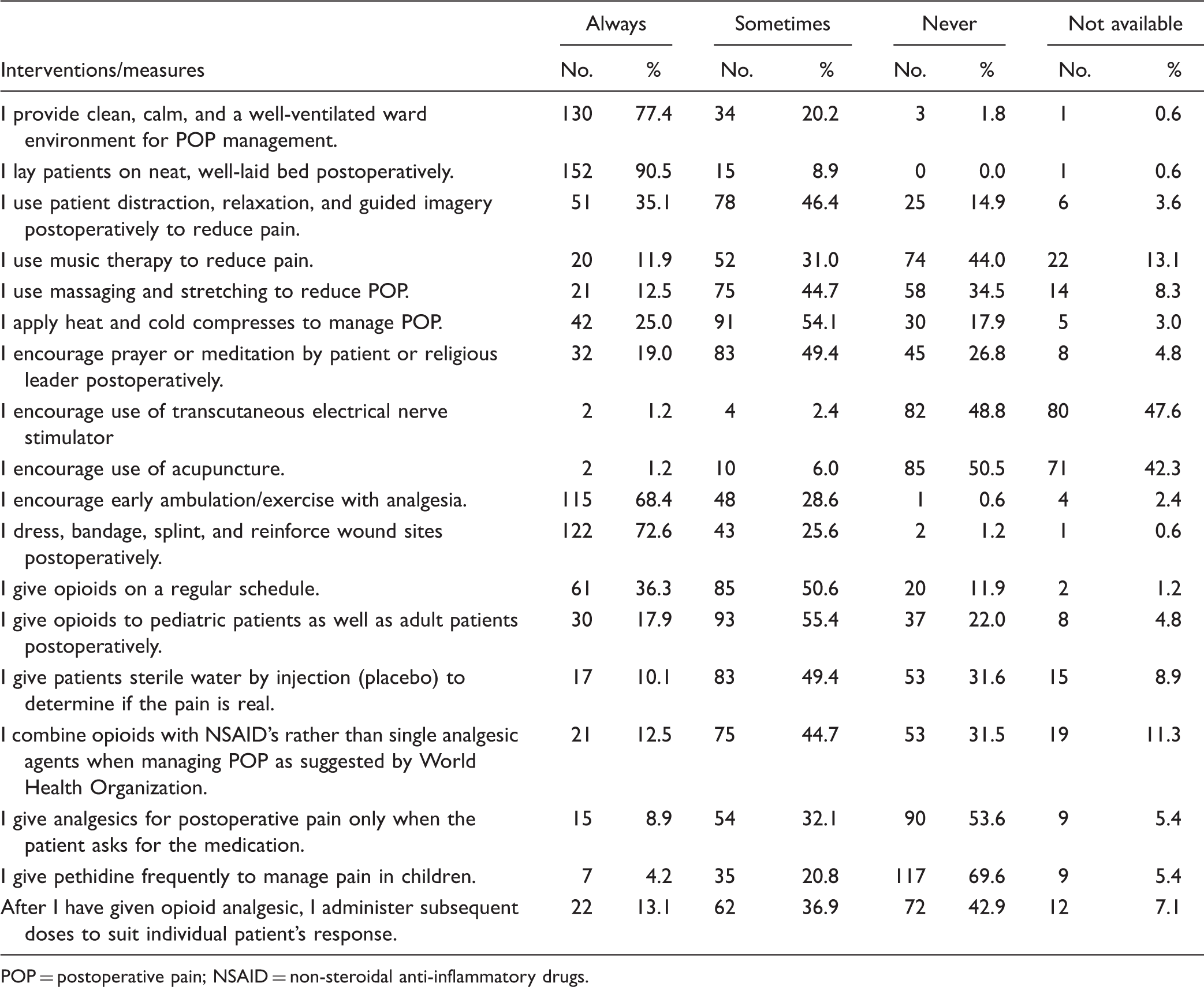
POP = postoperative pain; NSAID = non-steroidal anti-inflammatory drugs.
Discussion
Nurses and midwives are key stakeholders where POP management is concerned as they have more patient contact around the clock. Unfortunately, literature cites these professionals as faulting in effective POP management. This study sought to examine the knowledge, attitude, and practices of nurses on POP management in four selected district hospitals in the Ashanti region of Ghana.
This study revealed that nurses in the four hospitals had inadequate knowledge regarding POP management. These findings are consistent with other studies by other researchers (Aziato & Adejumo, 2013; Francis & Fitzpatrick, 2013; Lewthwaite et al., 2011) who also found inadequate knowledge of nurses in POP management. Several reasons could be linked to this finding. The study was conducted in district settings where nurses seldom had access to training programs on pain management. In addition, most nurses who answered the questionnaire had less than 5 years' experience and this could have impacted negatively on their knowledge.
Also, the majority of nurses had basic qualifications in nursing (74.4%) and only a few (19.0%) possessed degrees as shown in Table 2. Although 52% scored above 8 out of the 13 questions on knowledge scale, they could be rated as having inadequate knowledge since the total percentage of respondents answering more than half of the 13-point scale fell short of the 60% needed to be rated as having adequate knowledge. Many nurses (48%) lacked sufficient practical knowledge to function effectively in managing POP. These findings are similar to other studies which concluded that nurses faulted in their knowledge of pharmacological remedies in POP (Abdalrahim et al., 2011; Francis & Fitzpatrick, 2013; Rafati, Soltaninejad, Aflatoonian, & Mashayekhi, 2016; Wang & Tsai, 2010). A study by Se, Yc, Rozainiee, and Ho (2009) concluded that nurses require regular in-service education to boost their knowledge in pain management. Similarly, a previous Ghanaian study found inadequate knowledge on pain management by nurses (Aziato & Adejumo, 2013). Their study identified gaps in student curricula during training, reduced clinical supervision, limited workshops for practicing nurses among others. Evidence available shows that significant positive change in knowledge can be achieved through brief interactive workshops to correct misconceptions and equip practicing nurses with safe and sound knowledge to deliver their duties (Gustafsson & Borglin, 2013). It has been highlighted that nurses have a low appreciation for pain management in general and this could be attributed to flaws in the curriculum (Chow & Chan, 2015; McCaffery, Pasero, & Ferrell, 2007). Nurse leaders need to use advocacy to make a strong case for continuing education programs in pain management and must ensure that all stakeholders including the Ministry of Health are aware of this problem. Moreover, Ghana has a deficiency in Bachelor prepared nurses. Meanwhile evidence shows that clinical outcomes are maximized with degree prepared nurses (Yakusheva, Lindrooth, & Weiss, 2014). In one study, researchers found that bachelor prepared nurses had good pain management practices as they administered opioids to patients better than nurses with lower qualifications (Rafati et al., 2016). Thus, a strong case must be made for degree nursing in Ghana.
Our study revealed that nurses had positive attitudes toward pain management. Respondents had good attitudes as they identified that lack of pain expression was not lack of pain and also identified that nurses must anticipate pain before assessment and treatment. In addition, most of the respondents agreed that POP management was part of the management in postoperative care and part of the patient's rights. A previous study showed that in some circumstances, nurses may have inadequate knowledge but good attitudes and are able to practice good POP management when their attitude is positive (Miller, 2012). However, respondents seemed to agree that visual assessment influences their response to managing patients' pain. This attitude, as may pertain to some cultures (Narayan, 2010), is a potential barrier in achieving optimal pain relief after surgery. Numerous studies show that this must not be relied on as the only indication or assessment and that the patient's verbalization of pain regardless of facial expression should be taken seriously (Chatchumni et al., 2016; Francis & Fitzpatrick, 2013; Koneti & Jones, 2013; Ruben, van Osch, & Blanch-Hartigan, 2015).
When examining management practices, there was a mismatch between what respondents described in the attitude section and what they actually practiced. Although many respondents (92%) indicated that effective analgesia is part of pain management, only 4.2% suggested they would administer a narcotic analgesic to children with POP and only 36.3% also admitted they gave opioids on regular basis. Aziato and Adejumo (2014) found that personal factors such as lack of commitment, fear of administering opioids, and fear of addiction to opioid analgesics may contribute to its low usage by nurses. It is important to note that sociocultural factors could also account for the reason why nurses may not administer pharmacologic interventions (Jones, 2012). In Ghana, some cultural norms do not support outward demonstration of pain especially in men (Aziato & Adejumo, 2015). Dissimilar results have, however, been documented in literature. Nurses preferred pharmacological interventions which they find simple as opposed to employing basic nursing interventions to improve comfort and reduce POP (Mackintosh, 2007; Rafati et al., 2016).
The results of this study provided valuable information and avenues for the development of future studies. Studies in other districts and regions in Ghana are necessary to allow for generalization. Interventional or experimental studies as pertained in other countries can be replicated to assess the impact of a structured educational program on pain management and documentation for nurses in Ghana. Studies to develop cultural and language relevant pain assessment tools in our local dialects to enhance pain assessment are recommended. Subsequent studies involving the patient will be necessary. This can involve patients who have lived experiences with POP in the district hospital setting.
Conclusion
Nurses in this study self-reported inadequate nursing intervention and assessment skills in the management of POP. This is a result of inadequate knowledge as well as limited range of practices utilized by nurses to offset the deleterious effects of POP as the study identified. However, Ghanaian nurses have good attitudes which can be harnessed to translate into evidence-based practices in POP management. There must be a paradigm shift in POP management by Ghanaian nurses. Nurses must be empowered through continuous development programs to keep abreast with changing trends pertaining to pain management postoperatively. This would ensure quality of care, improve nursing care, patient satisfaction, and ultimately improve patient outcomes in Ghana.
Implication of Study
Curricula revisions in colleges of nursing in Ghana are necessary for effective education of nursing students in POP management. Nurse leaders could also advocate for more degree nursing institutions rather than diploma nursing education as currently exist in Ghana. This is important since evidence shows that degree nurses are better managers of pain. Of equal importance is the need to review and update the pharmacology content in the various nursing programs in Ghana to encompass new trends in assessments, documentation, and management of POP. Interventional or experimental studies in the area of POP management should be encouraged in Ghana in order to help address the challenges that confront nurses in effective management of POP.
Limitation of Study
This study was carried out in only Ashanti region, which is one out of 10 regions in Ghana. Although sample size calculation formula was used in identifying a sample size for this study, there is need to include more regions and more hospitals in Ghana in order to better generalize the findings to Ghana. The study considered only district hospitals which are smaller hospitals in comparison to regional and teaching hospitals in Ghana. It will be necessary to assess knowledge, attitudes, and practices of nurses within regional and teaching hospitals in order to have a holistic understanding of nurses' knowledge, attitudes, and practices in hospitals in Ghana.
Footnotes
Acknowledgments
The authors would like to express their profound gratitude to the nurses who took time off their busy schedules to fill out the questionnaire.
Authors' Contributions
A. M., I. G., S. A. A., and D. F. A. conceptualized the study. A. M. collected the data. A. M., I. G., and S. A. A. analyzed the data. I. G., C. A., and A. M. drafted the manuscript and all the others edited and approved the content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.