
Abstract
The purpose of this study was to assess the impact of a mentored guideline implementation (Registered Nurses’ Association of Ontario Prevention of Falls and Falls Injuries in the Older Adult Best Practice Guideline) focused on enhancing sustainability in reducing fall rates and number of serious falls and the experience of staff in three acute care hospitals. The National Health Service (NHS) Sustainability Model was used to guide the study. Interviews and focus groups were held with 82 point-of-care professional staff, support staff, volunteers, project leaders, clinical leaders, and senior leaders. Study results supported the importance of the factors in the NHS model for sustainability of the guideline in these practice settings. There were no statistically significant decreases in the overall fall rate and number of serious falls. The results supported strategies of participating hospitals to become senior friendly organizations and provided opportunities to enhance staff collaboration with patients and families.
Keywords
Introduction
Injurious falls in acute care hospitals are a common, costly, and health-limiting problem (Zecevic et al., 2012). Up to 84% of adverse events in acute care hospitals are related to falls (Aranda-Gallardo et al., 2013). Consequences of in-hospital falls are significant including fractures, pain, increased length of hospital stay, increased patient discharges to long-term care facilities, and economic burden to the health-care system (Miake-Lye, Hempel, Ganz, & Shekelle, 2013; Spoelstra, Given, & Given, 2012; Zecevic et al., 2012). Falls also have an emotional impact on patients and their caregivers, such as fear of falling, reduced physical activity, anxiety, and depression (Miake-Lye et al., 2013; Spoelstra et al., 2012). In addition, falls affect nursing and interdisciplinary staff, causing feelings of guilt and distress (Oliver et al., 2008).
Multifactoral interventions (including exercise, setting medication targets, and assistive preventive technology) in acute care hospitals have resulted in significant reductions in risk of falling and rates of falls (Cameron et al., 2012; Tricco et al., 2017). Implementation of best practice guidelines for fall prevention in both acute care and community settings can result in improved practice and patient outcomes (Davies, Edwards, Ploeg & Virani, 2008). Yet, guideline implementation initiatives have been reported to result in sustainability failure rates as high as 41% to 70% 2 years after completion of the implementation (Davies & Higuchi, 2013).
Mentoring, a knowledge translation intervention, has the potential to influence sustained guideline implementation (Abdullah et al., 2014; Maher, Gustafson, & Evans, 2007; Marchionni & Ritchie, 2007). Mentoring is defined by three critical characteristics: (a) mentors are more experienced than mentees in guideline implementation; (b) mentors provide individualized support based on mentees’ learning needs related to the implementation; and (c) mentoring occurs in the context of a beneficial and committed interpersonal relationship (Abdullah et al., 2014). However, it is not known how mentoring improves sustainability of guideline implementation or what the components of such a mentored approach should include (Miake-Lye et al., 2013). Thus, the purpose of this study was to assess the impact of a mentored guideline implementation focused on enhancing sustainability in reducing fall rates and numbers of serious falls in three acute care hospitals.
Review of the Literature
Falls Prevention in Acute Care Hospitals
A fall is defined as “an event in which a person’s unintentional and unexpected loss of balance was followed by his or her landing on a lower level” (Zecevic et al., 2012, p. 141). Reported fall rates vary greatly in the literature (e.g., from 3 to 13 falls per 1,000 patient days) depending on setting, population, and definition of falls (Oliver et al., 2007). A fall can also be categorized by severity, with a severe fall causing: “extreme discomfort, serious harmful effects, major intervention required, major potential to increase length of stay and potential for future intervention” (Zecevic et al., 2012, p. 141).
In-hospital falls are caused by a complex constellation of factors (Cameron et al., 2012). Factors in the hospital environment found to influence falls include: polypharmacy and the use of sedative and hypnotic medications; patient unassisted attempts to use the washroom; lack of transfer equipment in bathrooms; poor condition of floors; poor lighting; inappropriate footwear; use of bedrails as restraints; and lack of available and appropriate transfer equipment (such as a mechanical lift; Choi, Lawler, Boenecke, Ponatoski, & Zimring, 2011; Zecevic et al., 2012).
Due to the multiplicity of such factors, fall prevention in acute care hospitals requires a comprehensive approach (Stern & Jayasekara, 2009; Tricco et al., 2017). A number of systematic reviews have been conducted to determine the implementation strategies, components, and effectiveness of acute care hospital fall prevention programs for older adults (Avanecean, Calliste, Contreras, Lim, & Fitzpatrick, 2017; Cameron et al., 2012; Hempel et al., 2013; Miake-Lye et al., 2013; Stern & Jayasekara, 2009; Tricco et al., 2017). These reviews found that the following interventions may be effective in reducing the number of falls in older adults: (a) a multidisciplinary, multifactorial intervention program (falls risk identification, supervised exercise program, education program, vision assessment, and treatment); (b) one-on-one patient education and goal-setting (patient-centered intervention); and (c) targeted risk factor reduction intervention (fall risk factor screen and recommended evidence-based interventions; Avanecean et al., 2017; Cameron et al., 2012; Hempel et al., 2013; Miake-Lye et al., 2013; Stern & Jayasekara, 2009; Tricco et al., 2017). Other factors associated with successful implementation of falls prevention programs included leadership support, engagement of front-line staff, guidance provided for a prevention program by a multidisciplinary committee, pilot-testing interventions, use of information systems to provide data about falls, integration of components with electronic health records, education of staff, and development of a culture of safety (Miake-Lye et al., 2013; Spoelstra et al., 2012).
Despite the variety of fall prevention strategies reported in the literature, there is a gap in understanding how to best implement and sustain fall prevention programs (Avanecean et al., 2017; Cameron et al., 2012; DiBardino, Cohen, & Didwania, 2012). Implementation strategies were not well described in the studies included in the systematic reviews and actual adherence to the guideline recommendations in these studies was not clearly stated (Hempel et al., 2013). A systems approach to fall prevention is articulated in the recently published Registered Nurses’ Association of Ontario (RNAO) Best Practice Guideline for Prevention of Falls and Fall Injuries in the Older Adult (RNAO, 2017). The 2011 version of the guideline was in place during the current study reported here and its recommendations for practice were integrated into the mentoring intervention. The guideline includes practice, education, organizational, and policy recommendations (RNAO, 2011).
Sustainability of Guideline Implementation
Sustainability is comprehensively defined as involving five constructs: “(1) after a defined period of time, (2) the program, clinical intervention, and/or implementation strategies continue to be delivered and/or (3) individual behavior change (i.e., clinician, patient) is maintained; (4) the program and individual behavior change may evolve or adapt while (5) continuing to produce benefits for individuals/systems” (Moore, Mascarenthas, Bain, & Straus, 2017, p. 6). Despite international interest in guidelines to improve patient care, significant challenges exist for health-care providers and decision-makers when determining which and how many guideline implementation strategies to select and how to tailor activities to address identified barriers (Davies & Edwards, 2013).
Guideline implementation has been evaluated to identify facilitators and barriers at the individual, organizational, and environmental level (Ploeg et al., 2007; Stenberg & Wann-Hansson, 2012). At the individual level, a common barrier was negative staff attitudes and beliefs, while an important facilitator was learning about the guideline through small group interaction. At the organizational level, facilitators included leadership support, champions, teamwork, and collaboration (Ploeg et al., 2007; Stenberg & Wann-Hansson, 2012). Barriers included limited integration of the recommendations in policy and documentation, time and resource constraints, organizational change, and return to old routines after periods of champion absence, such as vacation (Ploeg et al., 2007; Stenberg & Wann-Hansson, 2012). Virani, Lemieux-Charles, Davis, and Berta (2009) identified the need for proactive attention to sustainability of clinical practice change by leaders and staff when implementing new guidelines. However, Graham and Tetroe (2007) identified that sustainability is typically only considered at the end of an implementation cycle, after evaluation of outcomes has taken place.
Conceptual model
The National Health Service (NHS) developed a model for sustainability of health-care innovations to support health-care leaders in the introduction of sustainable initiatives to improve quality of care and the patient service experience (Maher et al., 2007). This model, unlike other models of knowledge translation, has specific guidance for users and focuses on early sustainability planning (Maher et al., 2007).
The NHS model is a diagnostic tool that helps users to identify the strengths and weaknesses in a best practice implementation plan and assess the likelihood of sustainability (Maher et al., 2007). A Sustainability Model Package was created by the developers of the NHS model to facilitate use of the model and includes tools to conduct an in-depth examination of the experiences of point-of-care staff and senior and clinical leaders involved with health-care organizational change. The model includes 10 key factors related to process, staff, and organization (see Figure 1).
NHS Sustainability Model. Note. Figure adopted from Maher et al. (2007) Sustainability model and guide (p. 5) and reprinted with permission from Sustainable Improvement, NHS England.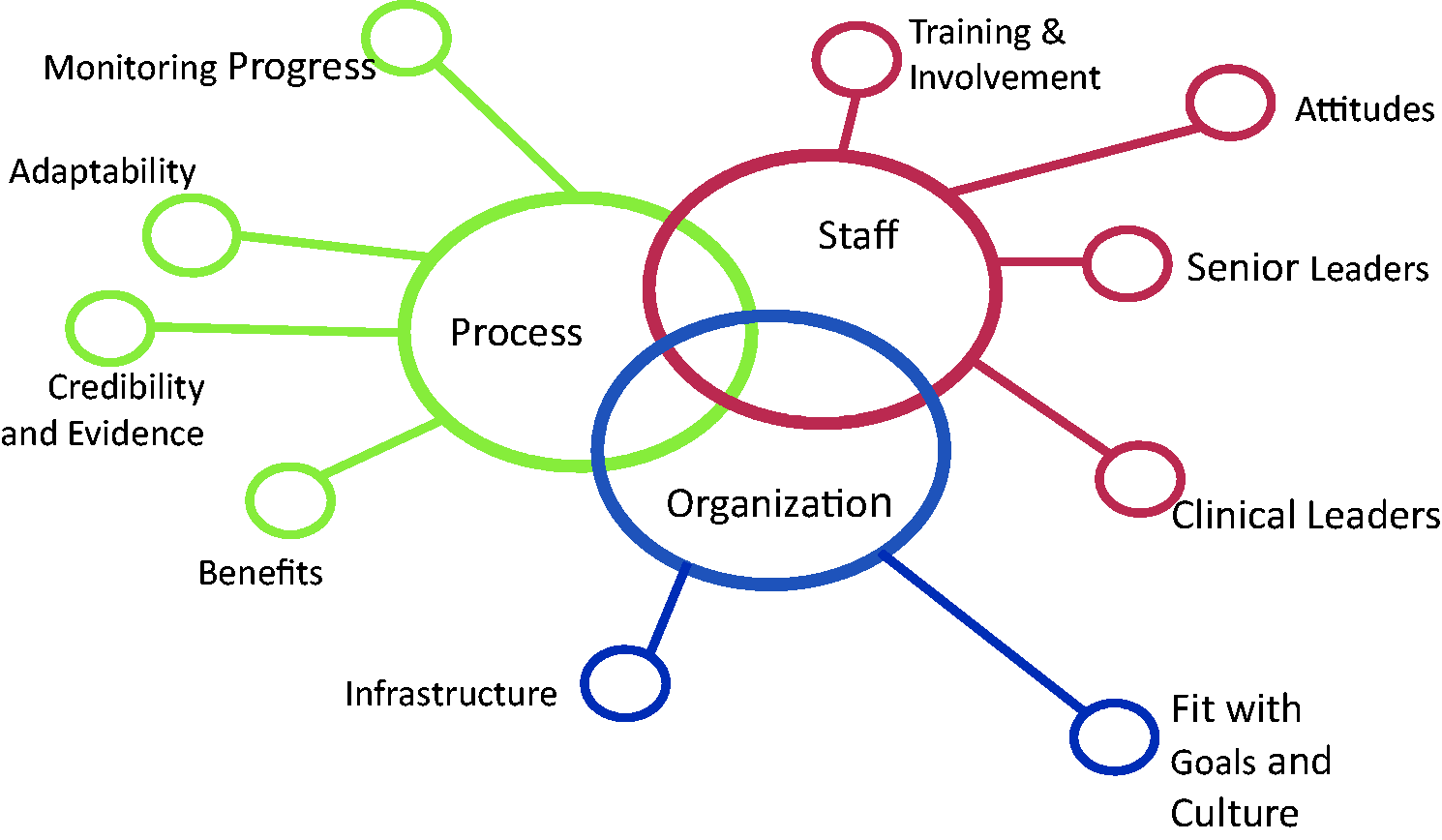
The NHS model can be used to self-assess against key criteria for each of the 10 factors (Figure 1). Self-assessment is recommended at several points when implementing a guideline (Maher et al., 2007). During planning, self-assessment is used to identify areas that require initial enhancement; at the pilot testing stage, results indicate which factors require strengthening in the implementation plan; and finally, the assessment is repeated during guideline implementation to ensure conditions are optimal for sustainability. A “master score system” allows users to calculate and determine an overall sustainability score (Maher et al., 2007, p. 21). A score of 55% or greater indicates that conditions are optimal for sustainability (Maher et al., 2007). Key factors with the greatest potential for improvement are identified through this process, and implementation activities can be designed and directed to address these factors.
Some empirical evidence supports the use of the NHS model in sustaining organization change. In a retrospective analysis of documents related to use of the NHS framework to implement multiple clinical practice guidelines at seven institutions, the use of the framework provided useful direction for leaders in the successful implementation of guidelines (Higuchi, Downey, Davies, Bajnok, & Waggott, 2012). The NHS framework also has demonstrated relevance in a Canadian setting (Higuchi et al., 2017). A formal evaluation of the NHS model by Doyle et al. (2013) revealed that facilitation is likely necessary for health-care teams to effectively use the model.
Based on the evidence, it was concluded that research in the area of fall prevention guideline implementation and evaluation required a comprehensive theoretical and methodological approach to take into account the complexity of different acute care hospital settings and the need for mentoring and support of study participants. The NHS model (Maher et al., 2007) provided such a framework.
Study Purpose
The purpose of this study was to assess the impact of a mentored falls prevention guideline implementation focused on enhancing sustainability in reducing fall rates and numbers of serious falls and the experience of participating staff in three acute care hospitals.
Methods
Design
A prospective, longitudinal intervention study with repeated measures over 2 years was conducted. Both qualitative and quantitative data were collected to understand the sustainability of the guideline implementation. The NHS Sustainability model (Maher et al., 2007) was used to guide the study intervention as well as data collection and analysis.
Research Questions
What are the experiences of point-of-care professional and support staff and senior and clinical leaders in acute care community hospitals related to implementing and sustaining a falls prevention guideline? What are the barriers and supports encountered when implementing and sustaining the falls prevention guideline? What are the patient fall rates and total number of serious inpatient falls at three acute care community hospitals before, during, and after a mentored implementation of the falls prevention guideline?
Setting and Sample
The study setting included three community hospitals in Ontario: two medium-sized hospitals and one small (based on number of beds and admissions; Canadian Institute for Health Information, 2016). For the qualitative component, purposive sampling, in particular maximum variation sampling, was used to sample a broad range of participants at multiple levels in each organization who had been involved in implementation and sustainability activities (Creswell, 2013). Study participants included the following groups: (a) Registered Nurses, Registered Practical Nurses, Occupational Therapists, Physical Therapists, environmental services staff, and volunteers for focus groups; and (b) Chief Nurse Executives, clinical managers, clinical educators, and project leaders for one-on-one interviews.
Ethical Considerations
The study received ethics approval from the Hamilton Integrated Research Ethics Board, Project #10-312. The three participating hospitals also conducted site-specific ethics reviews prior to the study commencement. Written, informed consent was obtained from all study participants.
Intervention
The mentored guideline implementation intervention process included multiple components that were based on elements of the NHS Sustainability Model (Maher et al., 2007). The purpose of the mentored intervention was to reduce fall rates and numbers of serious falls through: (a) enhancing sustainability action planning; (b) providing on-going feedback to implementation teams about patient outcomes through collection and analysis of quantitative data; (c) identifying barriers and supports that occurred in the implementation of the guideline through collection and analysis of qualitative data; and (d) providing education and networking opportunities for project leaders at the three participating hospital sites (see Figure 2 for an illustration of the mentored intervention).
Framework for mentored guideline implementation.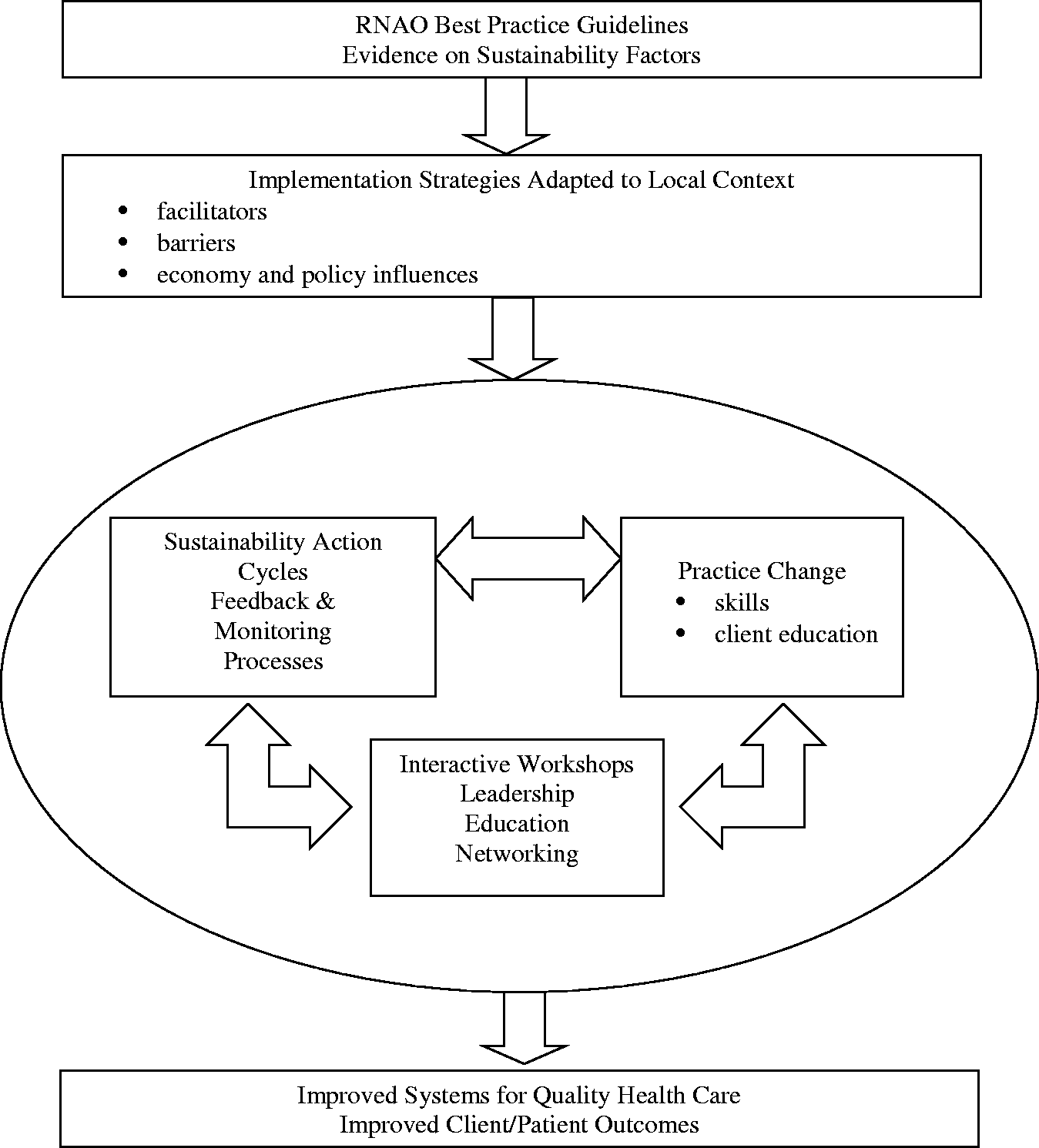
The principal investigators (JP and SI) and a coinvestigator (KC) provided the mentoring interventions in their roles as the research team mentors. (JP), a senior nursing researcher, had considerable experience collaborating on evaluation studies of guideline implementation and knowledge translation research. (SI), a senior nursing leader had extensive experience in the implementation and evaluation of guidelines in acute care settings. (KC), professional practice and education specialist, had extensive clinical management experience in implementing practice changes at the point-of-care. The intervention included three interactive workshops and two sustainability action cycles (Maher et al., 2007).
Interactive workshops
Clinical leaders from each of the participating community hospitals attended an initial sustainability action planning workshop at the beginning of the project. This workshop provided leaders with an introduction to the key elements of the NHS Sustainability Model (Maher et al., 2007). Participants also had an opportunity to apply their learning to their respective sites by planning for: (a) implementation of the guideline; and (b) generation, dissemination, and application of fall rates and number of serious falls results from the hospitals’ common electronic fall occurrence reporting system. The initiation of the mentorship relationship between the research team mentors and the clinical leader mentees began at this event and developed at two subsequent education and networking sessions held prior to implementation of the fall prevention guideline.
Sustainability action cycles
During the implementation period, seven site visits to the three participating hospitals were conducted by the research team mentors. Two visits per hospital were planned but inclement weather resulted in one visit being canceled. Site visits were focused on mentorship and training in the areas of evaluation and monitoring of patient fall-related outcomes and conducting problem-solving sessions on issues related to the Sustainability Action Planning processes in progress. Planned agenda items were developed collaboratively with each site in advance of the meetings.
Historical organizational fall data were reviewed with the site teams to develop an understanding of the contextual issues at each site. On-going barriers, facilitators, and stakeholder influences were also discussed. The research team mentors took an appreciative inquiry approach in these discussions with mentees to focus on positive accomplishments and celebrate achievements (Akrich, Collon, & Latour, 2002). Given that three hospital sites were involved in the project, sharing of materials that were being developed for falls prevention was done at these visits.
The scores achieved on each factor included in the Sustainability Model self-assessments were reviewed with the implementation teams and the project progress was discussed using the NHS Sustainability Model as a guide (Maher et al., 2007). Each of the sites had access to the NHS model and associated tools electronically and the sites made these available to all staff on their intranets.
Data Collection
Qualitative data collection
Qualitative data were collected at the end of the intervention period, when project leaders at each site identified and recruited participants for the focus groups and interviews. A trained research coordinator conducted the interviews and focus groups at all sites. Focus group and interview questions were based on the sustainability factors identified in the NHS Sustainability Model (Maher et al., 2007). Additional questions were informed by previous guideline implementation research regarding barriers, facilitators, and implementation strategies (Davies et al., 2006; Davies et al., 2008; Ploeg et al., 2007). Questions about the perceived impact of the mentoring intervention were also included (see Appendix). Documents such as site logs and meeting minutes provided additional information about fall prevention and mentoring activities.
Quantitative data collection
The falls data available for this study were reported on a quarterly basis and represented total falls and falls resulting in serious injury over a 3-month period. Falls data were available for three quarters for the preintervention period, four quarters for the intervention period and five quarters for the postintervention period. Retrospective and prospective data identifying quarterly number of falls, fall rates, and numbers of serious falls were provided by the risk management and patient safety departments at each study site. Monitoring of outcomes was facilitated by the standardized reporting of fall occurrences using rL Solutions occurrence reporting software (Risk Monitor Pro Software, 2012) and hospital patient day data. Fall data from all inpatients admitted to the three community hospitals during the study timeframe (33 months) were included.
Serious falls were defined as a category of equal to or greater than five in the data received from rL Solutions database. To be ascribed a score of ≥5 in the rL Solutions database, the person who has fallen has experienced severe harm that would: (a) require life-saving intervention or major surgical or medical intervention, (b) shorten life expectancy or cause major long-term harm and loss of function, or (c) cause death. The NHS Sustainability Model self-assessment was conducted at the beginning and end of the intervention period (Maher et al., 2007).
Analysis
Qualitative analysis
Focus groups and interviews were tape-recorded and transcribed verbatim. The data were entered into NVivo qualitative data analysis software program, version 10. Analysis involved the use of a template analysis style (Crabtree & Miller, 1999). This involved focusing on particular aspects of the transcript based on a predetermined template or model (Crabtree & Miller, 1999). The NHS Sustainability Model was used as the organizing framework. The research team mentors and a research coordinator conducted the analysis. These four individuals independently coded some of the transcripts based on the factors in the NHS Model and met to agree on a coding scheme for the remaining transcripts. The coding scheme was used by the research coordinator to code the remaining transcripts. Qualitative rigor was enhanced through a number of strategies. Participants at multiple levels of the organizations were included resulting in diverse perspectives on the topic and improved generalizability of results. Coding and data analysis was conducted by four individuals with expertise in qualitative research, contributing to investigator triangulation of results. Finally, a report of the results for each site was shared with and presented to leads and champions at each site and opportunities were provided to discuss the findings.
Quantitative analysis
A p value <.05 was considered statistically significant (
Patient outcomes at the hospital level of fall rates/1,000 patient days and numbers of serious falls were determined through descriptive statistical analysis. Fall rate/1,000 patient days was used for comparing falls within and between acute care hospitals as it accounts for hospital occupancy levels during the study time frame (Agency for Healthcare Research and Quality, 2013). For example, if the hospital had a period of time with numerous empty beds, there would likely be fewer falls, regardless of the fall prevention program. The falls rate per quarter was calculated by dividing the number of falls per quarter by the number of occupied bed days for that quarter and multiplying the result by 1,000. Fall rates per quarter were calculated for each study site and overall (three sites combined), and average falls rates were calculated for the three study periods (preintervention, intervention, and postintervention). An analysis of variance (ANOVA) test of the overall differences in falls rates and serious falls for the three periods in the study were also conducted.
Total number of inpatient falls resulting in a serious injury were used to calculate mean serious falls for each quarter. This mean was calculated for the three sites, in each study period, by adding the number of serious falls at all three sites and dividing by the number of quarters in the study period (preimplementation [three quarters], intervention [four quarters], and postintervention [four quarters]).
Results
Sample Characteristics
Demographic Description of the Study Participants (n = 82).

Best Practice Guideline Fall Prevention Activities
Examples of Fall Prevention Activities by National Health Service Sustainably Model Factor.

Experiences of Professional and Nonprofessional Staff and Administrators
The following analysis of qualitative interview and focus group data is presented under the NHS (Maher et al., 2007) categories of staff, process, and organization and the associated sustainability factors. Also included is a category describing patient and family based on a consensus decision made by participants and researchers.
Staff
Senior leadership engagement and support
Senior leaders reported closely monitoring occurrence reporting summaries. This information generated questions about factors contributing to falls and actions required and informed dialog with clinical leaders and members of hospital boards. Open forums and patient safety walkabouts provided leaders with opportunities to interact with staff and identify needed resources. Leaders advocated for the fall prevention needs of staff to be identified as a hospital priority in planning and resource allocation but reported the challenges they faced. Like we are working on it … if you really need it, then you should get it because that is the right thing to do and everyone knows it, but we’re always … managing resources against a million other priorities. (Interview, senior leader)
Clinical leadership engagement and support
Clinical leaders described how in their management roles they: interpreted results of occurrence data based on a synthesis of staff discussion about serious falls and their knowledge of the workings of the unit to identify resources, efficiencies or realignment of work that may address gaps … advocating with directors and other senior leaders for funding. (Interview, clinical leader)
Staff involvement and training to sustain the process
Participants described how various point-of-care professional and support staff were involved in planning, implementing and sustaining the fall prevention program. A variety of formal and informal educational strategies were used to engage staff in developing a fall prevention program that would ensure that patients were consistently assessed for fall risk. At the organizational level, fall prevention committees were identified as important to implementation and sustainability. We have a dedicated working group from the different areas in the hospital who are committed, see this as a big issue, and want action. So, you have people who are very strong. They have leadership within their program, and they are able to make change happen. (Interview, clinical leader)
Staff behaviors toward sustaining the change
Staff members described a variety of strategies that facilitated sharing of ideas and provided opportunities for them to provide either formal or informal leadership in fall prevention. Both leaders and point-of-care professional staff assumed formal (e.g., champion or clinical expert), informal, and sometimes rotating leadership roles (e.g., charge nurse, experienced nurse). The need to take a “step by step” approach, consistent with a quality improvement methodology, was identified by both leadership and point-of-care staff. I think providing the forum for these discussions to happen and to … provide some kind of consistent forum so that they know they can bring those issues to us and that we do look at, together, problem-solving and then looking at tweaking things … the PDSA [plan, do, study, act] cycle. (Interview, leader)
Process
Adaptability of improved process
Participants reported that the implementation and sustainability of the fall prevention program was facilitated by a number of organizational changes and priorities. The alignment of fall prevention with Canadian hospital accreditation standards was a key driver. Fall prevention programs were a natural fit with other organizational quality priorities required to meet these standards: quality councils, patient safety, seniors’ health, interprofessional care, medication reconciliation, electronic documentation implementation, and communicating best practices to the community. I think there will be a focus so it does keep on going because we all know that that’s the biggest issue besides medication in a safety environment for patients … because it is part of the quality improvement plan [this year] … it’ll roll over into the next QIP [quality improvement plan]. (Interview, leader) You know in the system there’s some gaps. They [patients] have been to a doctor that has given them some medications and another doctor and they’re giving them something different or something else … then the physician looks at it and says, “Wow! How come you are on all these things?” (Interview, clinical leader)
Effectiveness of the system to monitor progress
The electronic occurrence reporting system common to the three participating hospitals was reported as a fall monitoring facilitator and a critical element in sustaining practice change. Senior leaders used the system to review serious incidents for contributing factors at both the staff and system levels and inform board reports and website postings.
Managers described a variety of approaches taken to communicate fall results to point-of-care staff. They also identified the lack of resources at the unit level as a barrier to monitoring staff performance in risk assessment. All of the statistics are posted after the monthly quality risk meeting … so that anyone who wants to know how many falls there were can get that information if they know where to get it and it’s also on our website. (Interview, senior leader) I think it would be a benefit for us to be made more aware of … the statistics, how well we are doing, where there’s room for improvement, where the falls are taking place, if there’s particular times of the night they are happening. If it’s at shift change or any of those [other] statistics that would show that type of information. (Focus group, point-of-care staff)
Benefits beyond helping patients
Implementation of the best practice guideline was recognized by participants as providing a wide range of benefits beyond helping patients. Benefits described included an increased awareness of patient safety issues, an opportunity to integrate evidence into practice and participate in research, and improved interprofessional teamwork, sharing of resources, and partnerships: “You know, just that whole team approach, that they’re actually working together to help reduce falls … the injuries of falls” (Interview, clinical leader). Some participants identified potential for reduction in staff injuries, patient length of stay, inconsistencies in practice, and utilization of health-care resources. Others identified how the implementation of the falls prevention guideline had improved their hospital’s reputation.
Credibility of the benefits
Participants articulated the importance of communicating the benefits of the fall prevention program to staff, including the impact on patients, organization, and the system. While some had a sense that fall rates were improving, others did not know what the fall rates were or how they compared with previous rates. The credibility of the fall risk assessment tool’s ability to accurately inform interventions for specific patient populations was questioned by many point-of-care staff, thus posing a threat to sustainability. Staff members were aware of the importance of communicating the economic benefits of reducing patient falls. “And you know, what it means for their length of stay, what it means for how much it costs per day … I think that hits home sometimes … when the team hears that” (Focus group, point-of-care staff).
Organization
Fit with organizational aims and culture
Leaders and point-of-care staff participants all agreed that the fall prevention program was consistent with their organizational strategic aims for quality improvement: patient safety, patient-centered care, creating a seniors’ friendly environment, and an evidence-based culture. It is part of our quality improvement plan and so we recognize the importance of it. Even though we started this initial participation under the RNAO best practice, but it has been recognized by both the hospital and more importantly by the board that this is something that is very important. It ties in completely with being a senior friendly organization. (Interview, senior leader)
Infrastructure
The investment of the hospital in the infrastructure to support and sustain fall prevention was evident: “Equipment is the key … crash mats, the high/low beds, the bed alarms are good. Just because when you do have minimal staffing, especially at night, you hear that alarm, you know you better be running” (Focus group, point-of-care staff).
Some point-of-care staff expressed concerns regarding the impact of staffing and equipment shortages on patient falls. Falls prevention is a wonderful thing but it’s going to get worse instead of better unless they [staff] have the ability to keep on top of their patients that need to get to the washroom on time, or, improve monitoring because … they don’t have time to do that. (Focus group, point-of-care staff)
Patient and family
While not a factor in the NHS model, participants reported that the fall prevention program had provided an opportunity to partner with patients and families in prevention of falls and readmissions related to falls. Patient and family educational materials provided staff with an opportunity for health teaching. I think at the same time for patients and families, it’s a greater awareness of the role they have to play in this because it is not all about us. It’s all about them understanding why we do some of the things we do and the importance of doing these things. And trying to work with the patient and family to achieve what’s best for the patient. (Interview, clinical leader) I think the patient and family are aware [of] how serious the situation is. Many times I have read them the booklet and they say, “Oh, my, I didn’t know that the death rate was so high with people who fall and end up in the hospital.” So, the awareness. And that’s helping quite a bit. (Focus group, point-of-care staff)
NHS Sustainability Model Self-Assessment Results
Three Study Site Composite NHS Sustainability Model Self-Assessment Results.

Note. NHS = National Health Service; T1 = Time 1 (intervention period), T2 = Time 2 (postintervention period), p level = significance level. Bold value signify that p values for the staff total, process total and organization total categories has been provided.
In particular, the effectiveness of the system to monitor progress showed high and steady sustainability scores from the preintervention to intervention period. Monitoring of fall rates was a key focus of the mentored intervention, thus demonstrating success in this area.
With respect to staff and their confidence in their involvement and training to sustain the process of implementation of the fall prevention guideline, while the scores started very high (92.46%), they did decline (70.58%), although not statistically significantly. Organizationally, participant scores on the investments in infrastructure made by all three of the hospital sites increased, although not statistically significant, from 68.02% in the intervention period to 79.53% in the postintervention period.
Fall Rates and Serious Falls
Three Study Site Composite Mean Quarterly Fall Rate/1,000 Patient Days and Total and Mean Quarterly Serious Falls by Study Period.

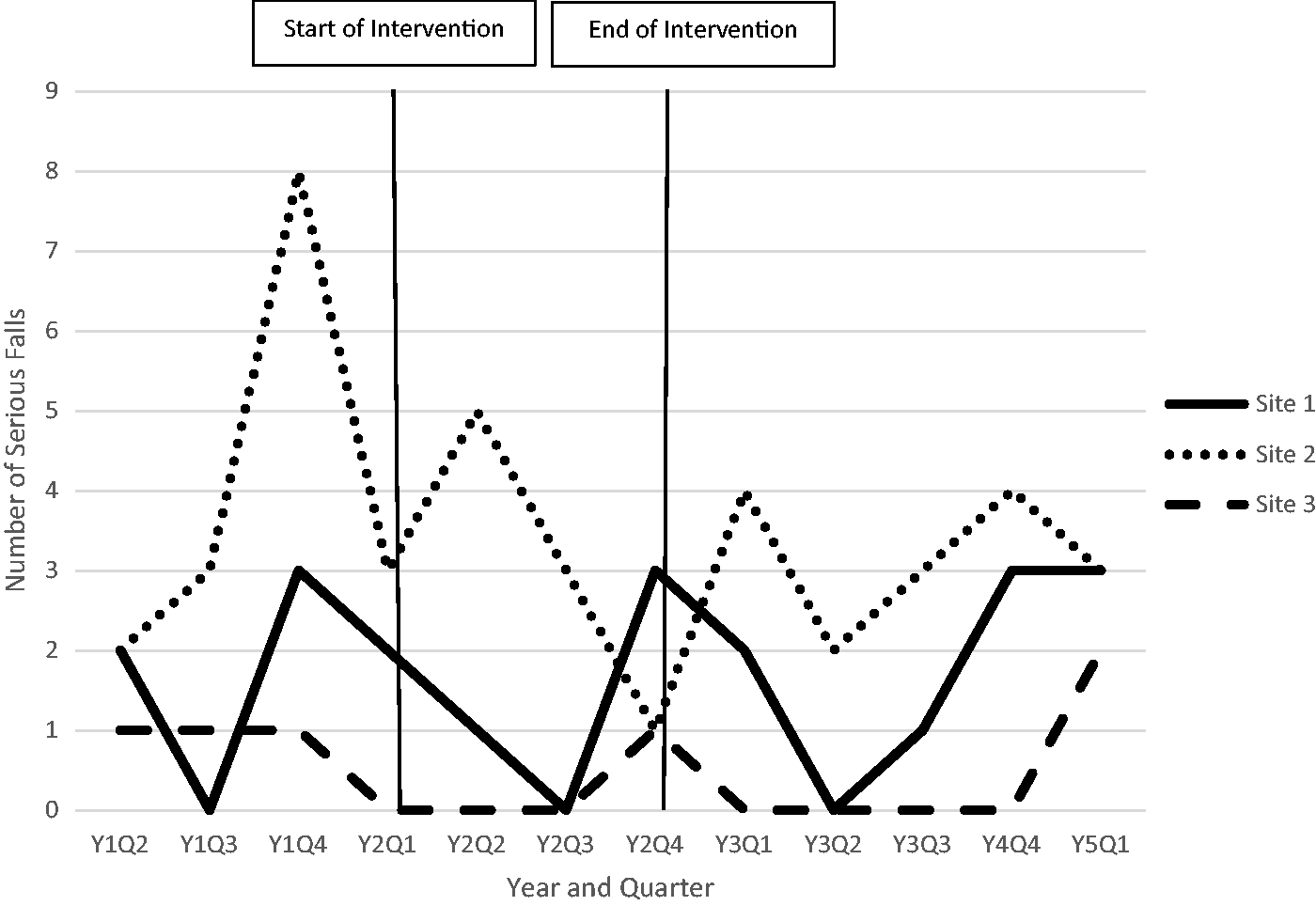
The ANOVA procedure was used to compare fall rates across the three study periods. A Welch-adjusted ANOVA was used to adjust for the heterogeneity of variances across the study periods (SAS version 9.4). The Welch-adjusted ANOVA indicated that the reported differences in fall rates were not statistically significant (F = 2.71, p = .10), likely due in part to the small number of falls. The mean fall rate primarily declined over the study period at two of the three study sites (Sites 2 and 3), whereas, the mean fall rate at the third site (Site 1) increased until the first quarter of the postintervention period (see Figure 3). No clear pattern emerged in mean number of quarterly serious falls (see Figure 4).
Fall rate/1,000 patient days over time by study site. Number of serious falls over time by study site.
Discussion
This article makes important new contributions to understanding the process of sustaining practice change in acute care hospitals related to fall prevention. Enhanced knowledge was gained regarding how activities directed by the NHS Sustainability Model can support sustainability efforts. As well, this article provides insights into the impact of mentoring support for sustainability on tackling common barriers to successful guideline implementation. Finally, the results highlight the challenges of assessing outcomes for fall prevention in large, complex organizations.
The NHS Sustainability Model self-assessment was useful in grounding the mentoring sessions and transferring knowledge at the three hospital sites. The results of the sustainability model self-assessment identified areas of strength in promoting sustainability at the study sites as well as areas requiring attention. Data on the model were collected from multiple sources from both leadership and point-of-care staff.
The development of the focus group and interview formats and the analysis of the qualitative data were enhanced by the use of the NHS Sustainability Model. For the most part, the sustainability factors provided a good fit with the data collected from point-of-care and leadership staff who participated in the focus groups or interviews. Barriers and facilitators to guideline sustainability within the factor data were readily identified.
Staff described the importance of engaging patients and families in fall prevention through the continuum of care. This finding identified a gap in the NHS model that necessitated the addition of “patient and family” as a factor. The emergence of patient and family as a factor is a novel finding related to factors influencing sustainability.
Additionally, during the mentoring visits with the site teams, it was apparent that there was wide variability in the status of the implementation of fall prevention best practices at the three study sites prior to their engagement in the research study. Engagement ranged from not having a strategy in place to the implementation of multiple strategies, which may explain the relatively static overall fall rate results reported. One site did experience an increase in falls from preintervention to postintervention periods. A new leadership team and an electronic reporting system were introduced concurrently with the research project, which challenged implementation of the falls prevention protocol. This is consistent with the findings of Doyle et al. (2013) in their formative evaluation of the application of the NHS model in the UK. At the time of their evaluation, UK was in the midst of a large-scale reorganization of service delivery to contain costs and this affected both senior leaders’ time and staff commitment to sustaining change as they were concerned about the future of their employment (Doyle et al., 2013).
Mentoring as a strategy for sustainability was a vital component of implementing the fall prevention guideline. The research team mentors influenced the implementation of the guideline by strategically and specifically targeting the typical barriers that can derail guideline implementation. Mentorship is different than other sustainability strategies, in that it focuses on the needs of the mentees (Abdullah et al., 2014). Mentorship requires expertise in the mentor and individualized support in the context of an engaged interpersonal relationship (Abdullah et al., 2014). For example, one of the project leaders identified challenges in communicating with point-of-care staff the baseline fall rate in relation to setting future targets. The research team mentor focused on support regarding strategies to improve the effectiveness of the system to monitor progress. Also, one of the mentors was well-known and respected among the senior leaders and this trust in the context of a previous relationship facilitated the mentoring related to the role of senior leaders in sustaining change. Finally, there was little change in the mean quarterly fall rates and the number of serious falls at the three hospitals over the study period.
Study Strengths and Limitations
A study strength was that it was undertaken in a “real world” setting. Furthermore, the utilization of the NHS Sustainability Model provided evidence-based structure and strategies to address the challenges of sustainability. The mentorship intervention involved a unique research partnership between nurse academics, nurse leaders, and point-of-care professional staff to explore sustainability of a falls prevention guideline. Another study strength is that the participants in the focus groups and interviews came from a wide range of clinical settings (e.g., general medicine to maternal-child) and positions (e.g., volunteer and Chief Nursing Officer).
There are study limitations to consider. First, there was a small number of overall and serious falls across the sites, which limited the statistical power for the quantitative analysis. Second, the three hospitals are all from the same geographic area of Southern Ontario, and perhaps reflect unique jurisdictional and practice characteristics. Third, in order to protect the anonymity of the participating sites, the results are presented as aggregate data which may obscure the individual challenges, context, and culture of each setting. As well, the study sites did not keep detailed records of the implementation changes so the full breadth of the practice changes could not be described. Finally, a small number of participants completed the NHS Sustainability model self-assessment and it was only done at two points in time, rather than three as recommended by the model’s authors (Maher et al., 2007).
Implications
Study findings support the inclusion of mentoring as part of sustaining fall prevention guideline implementation. Mentorship could be accomplished by forging creative partnerships with universities or with staff and leaders from other organizations. As was done in this project, effective fall prevention strategies can be discussed among neighboring hospitals and this was particularly helpful where one organization had more experience with multifaceted fall prevention program implementation. The impact of mentoring as part of guideline implementation requires further research to better understand and measure the effect (Abdullah et al., 2014).
Study findings support senior leaders taking a highly visible and active role in keeping fall prevention an organizational priority and recognizing the accomplishments of staff in fall prevention. The findings revealed that staff members are quite sensitive to feeling supported by senior management when making practice changes opportunities for staff and leaders to dialog are necessary. The importance of increasing the attendance of staff at senior leader forums and staff meetings and formally engaging point-of-care staff as champions was stressed by participants. This sharing of ideas and discussion routinely during change cycles is needed to facilitate staff perseverance and sustain the gains.
As the findings demonstrate, fall prevention is dependent on point-of-care professional and support staff knowledge, engagement, and time. It is important that clinical leaders have resources to sustain fall prevention awareness for all staff, including the need to provide relief hours for ongoing education, feedback, and audit activities. Consistent with research on sustaining guideline implementation, providing on-going staff education is challenging and creative alternatives to the traditional in-service, such as e-learning or brief huddles, require exploration and evaluation (Ploeg et al., 2007). Best practice fall prevention interventions are time-intensive, especially when staff members are on a learning curve, which has implications for workload measurement tools. These tools must be able to accurately measure the time required to provide patient and family education, particularly on units where the prevalence of fall risk, cognitive impairment, and delirium are high. In turn, this workload measurement must be translated into flexible, proactive staffing models that can adjust staffing based on shift challenges and changing patient needs.
Findings from qualitative data suggest that staff input is vital to determining what kind of feedback related to falls is most meaningful and that the type of feedback may need to change over the course of sustaining the practice changes. Equally important is that feedback is provided to all staff related to falls at the unit and operational levels as well as to other stakeholders, such as the public and community providers. The findings support that the format for sharing feedback should be varied, timely, and user-friendly.
The novel finding of the important role of patients and families suggest that the engagement of patients and families should be increased in fall prevention programs, including representation on fall prevention committees. Future research is needed to develop and test models or strategies designed to provide clinical staff with consistent and meaningful feedback about patient fall and other patient safety outcomes. Patient and family involvement in the context of sustainability also requires further research.
Conclusion
This study contributes important understandings about the impact of using the NHS Sustainability Model to facilitate a mentored implementation of a fall prevention guideline at three acute care sites. Study findings revealed that sustaining change does not end at the implementation period. As noted in the qualitative findings, the interventions required adaptation and refinement over time, for example, in relation to feedback on fall rates and tailoring fall risk assessment to different patient groups. This is the “paradox” of sustainability: The acute care context is continually changing and by extension so must clinical practice (Chambers, Glasgow, & Stange, 2013). As such, mentoring can be particularly relevant and useful. Future work and research with the NHS model should include consideration of external health-care system factors that contribute to the dynamic nature of health-care systems and care delivery processes (Doyle et al., 2013).
Footnotes
Appendix. Focus Group and Individual Interview Guide.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.