
Abstract
Background
Prenatal depression, anxiety, and stress (prenatal psychosocial distress) are common, and several environmental risk factors have been implicated in their development. Variation in genes, specifically single nucleotide polymorphisms (SNPs), may explain why some women develop maternal mental health concerns while others do not.
Purpose
The purpose of this pilot study was to determine the feasibility of completing SNP analyses using whole blood collected prenatally between 2008 and 2011. We examined the association between SNPs in two genes (FKBP5 and OXTR) among women with low and high prenatal psychosocial distress.
Methods
A subset (N = 50, 25 high and 25 low prenatal psychosocial distress) of participants was selected from the All Our Families pregnancy cohort. DNA was extracted from maternal blood and used for selected SNP analysis. Participants’ scores on the Edinburgh Prenatal Depression Scale, Spielberger State Anxiety Inventory, and Perceived Stress Scale were used along with demographic variables.
Results
Genotype distribution was not significantly different between the low and high prenatal psychosocial distress groups for either the FKBP5 or the OXTR SNP (p = .699 and p = .125). After controlling for maternal age and income, women with the GG genotype at the OXTR SNP (rs237885) were statistically less likely to be in the high prenatal psychosocial distress group (p = .037).
Conclusion
OXTR SNP rs237885, maternal age, and lower income were associated with prenatal psychosocial distress. This pilot study demonstrated the feasibility of continuing to a larger study that incorporates additional environmental and genetic information.
Introduction
Prenatal depression, anxiety, and stress are common and can impact the physical and emotional health of the mother and child during pregnancy, birth, and postpartum (Dunkel Schetter & Tanner, 2012). During pregnancy, depression and anxiety may lead to a wide array of emotional and physical symptoms, including more nausea and vomiting, as well as extra days off work and increased visits to the obstetrician due to fear of childbirth (Andersson, Sundström-Poromaa, Wulff, Åström, & Bixo, 2004). Poor birth outcomes associated with depression and anxiety include preterm birth and low birth weight (Ding et al., 2014; Raisanen et al., 2014). In the first year postpartum, mothers who experienced prenatal depression or anxiety may develop postpartum depression or anxiety, and there is evidence that both prenatal and postpartum depression can negatively influence infant development (Biaggi, Conroy, Pawlby, & Pariante, 2016; Kingston, Tough, & Whitfield, 2012). In the All Our Families (AOF) community-based, longitudinal pregnancy cohort, from which participants were selected for this pilot study, the prevalence of prenatal depression (Edinburgh Postnatal Depression Scale [EPDS] ≥ 13), prenatal anxiety (Spielberger State Anxiety Inventory [SSAI] ≥ 40), and prenatal stress (Perceived Stress Scale [PSS] ≥ 20) was 8.1%, 16.9%, and 18.1%, respectively (Tough et al., 2017). As prenatal depression and anxiety are often comorbid and high prenatal stress is predictive of prenatal anxiety and depression, this study examines prenatal depression, anxiety, and stress together (hereafter referred to as prenatal psychosocial distress; Bayrampour, Tomfohr, & Tough, 2016; Biaggi et al., 2016; Falah-Hassani, Shiri, & Dennis, 2017).
Prenatal psychosocial distress has a multifactorial etiology, as evidenced by multiple environmental risk factors that may be associated with the development of symptoms. Risk factors for the development of prenatal psychosocial distress include poor social support, dissatisfied relationship with partner, young age, and lower education (Biaggi et al., 2016; Leigh & Milgrom, 2008). However, these risk factors are experienced by many new mothers, and risk factors alone do not fully explain why one woman will experience prenatal psychosocial distress and another will not (Corwin, Kohen, Jarrett, & Stafford, 2010). Reviews of recent research highlight the potential importance of individual genetic susceptibility to the development of prenatal mental health conditions (Figueiredo, Parada, de Araujo, Silva, & Del-Ben, 2015; Serati, Redaelli, Buoli, & Altamura, 2016).
Single nucleotide polymorphisms (SNPs) provide a source of genetic variation in the human genome. Although most SNPs have not been functionally characterized, some have been linked to complex health issues, including mental health conditions. FK506 binding protein (FKBP5) is involved in regulation of the glucocorticoid receptor (GR) complex and has an epigenetic mechanism mediating gene by environment interactions (Klengel et al., 2013). Genetic variations in FKBP5 have been associated with several mental health issues, including depression, posttraumatic stress disorder, and attempting suicide (Binder et al., 2008; Roy, Gorodetsky, Yuan, Goldman, & Enoch, 2010; Zimmermann et al., 2011). The FKBP5 SNP rs1360780 is a functional polymorphism, and the risk allele (T-allele) causes increased mRNA expression following GR activation leading to GR resistance and an extended cortisol response following exposure to stress (Klengel et al., 2013). The hormone oxytocin has been implicated to play a role in complex human social interaction, including maternal–infant relationships (Galbally, Lewis, Ijzendoorn, & Permezel, 2011). Oxytocin acts via interaction with the oxytocin receptor (OXTR), and variations in the OXTR gene have been associated with depression (Mileva-Seitz et al., 2013; Saphire-Bernstein, Way, Kim, Sherman, & Taylor, 2011). Specifically, the OXTR receptor SNP rs237885 was previously associated with prenatal depression (Mileva-Seitz et al., 2013). For this pilot study, our aim was to determine the feasibility of conducting selected SNP analysis with maternal blood samples (taken at 17–23 weeks of gestation) of the AOF cohort collected between 2008 and 2011. We selected two of the many SNPs previously associated with mental health conditions and examined the relationship between self-report of prenatal psychosocial distress and genotype at these two SNPs. The specific FKBP5 SNP was chosen due to multiple associations with mental health conditions and known functional effect of the SNP. The specific OXTR SNP was chosen based on evidence of association with complex human social interaction and a previous report of an association with prenatal depression.
Materials and Methods
Participants
This study included women (N = 50) selected from the AOF prospective community-based birth cohort in Calgary, Alberta, comprising 3,387 pregnant women at initial enrollment (Tough et al., 2017). For the current study, participants were included if they completed a detailed questionnaire at intake (<25 weeks of gestation) and provided a whole blood sample taken at 17 to 23 weeks of gestation (N = 1,867). The questionnaire completion and blood collection occurred at different times due to strategic study design to enhance convenience for community participants and pragmatic issues arising from collecting data from a large number of participants (Gracie et al., 2010; McDonald et al., 2013; Tough et al., 2017). Participants were excluded if they delivered preterm and/or had preeclampsia as there is evidence of association between prenatal depression and both preterm birth and preeclampsia and possible susceptibility to preterm birth related to genetic variation in the oxytocin pathway (Kim et al., 2013; Li, Liu, & Odouli, 2009; Qiu, Williams, Calderon-Margalit, Cripe, & Sorensen, 2009). To maximize variation between the low and high prenatal psychosocial distress groups, participants were selected by calculating percentiles based on scores on the EPDS, SSAI, and PSS. Participants who scored in the 90th percentile of the scores on all three scales (suggesting high depression [score of ≥10 on the EPDS], high anxiety [score of ≥40 on the SSAI], and high stress [score of ≥20 on the PSS]) formed one group of 25. Participants who scored in the bottom 10th percentile on all three scales (indicating low depression, low anxiety, and low stress) formed another group of 25. The sample size of 50 was chosen due to the primary aim of determining the feasibility of conducting the SNP analysis using blood samples collected between 2008 and 2011.
The AOF study was approved by the Conjoint Health Research Ethics Board at the University of Calgary (REB ID 15-0248). Participants provided informed consent at the time of recruitment and were provided copies of the consent form for their records. This secondary analysis was also approved (REB ID 16-0971).
Study Variables
Information on demographics and maternal psychosocial distress variables was obtained from self-report questionnaires completed at < 25 weeks of gestation. All study variables for the AOF cohort were collected at < 25 weeks to capture the lower bounds of viability concomitant with preterm birth. Demographic variables included age at the administration of questionnaire, income, level of education, presence of partner, ethnicity, parity, and gravidity.
Maternal psychosocial distress variables included self-reported symptoms of depression, anxiety, and stress assessed at intake. The EPDS is a 10-item self-report scale with robust validity and reliability (Cox, Holden, & Sagovsky, 1987). The EPDS has been validated for use in pregnancy (Murray & Cox, 1990). A score of 10 or higher on the EPDS is used by primary care providers to indicate possible depression and the requirement for additional assessment (Cox et al., 1987). The SSAI is a subscale of the State-Trait Anxiety Inventory and is a 20-item scale used to assess an individual’s current state of anxiety (Spielberger & Gorsuch, 1970). The PSS is a 14-item self-report instrument used to assess self-appraisal of stress due to life events in the past month (Cohen, Kamarck, & Mermelstein, 1983). The psychometric properties of the SSAI and PSS in a pregnant population were tested using AOF data and were found to be strong (Benediktsson, McDonald, & Tough, 2017).
DNA Extraction and Genotyping
Maternal whole blood samples were collected in EDTA tubes at 17 to 23 weeks of gestation and stored at −80℃ (Tough et al., 2017). Maternal genomic DNA was extracted from whole blood samples using the Qiagen QIAamp DNA Blood Midi Kit. Genotype information was obtained for FKBP5 (rs1360780) using polymerase chain reaction (PCR) and sequencing. In brief, the region of genomic DNA containing the polymorphism was amplified using primers previously used for this purpose (Ventura-Junca et al., 2014). Amplified PCR product was purified using the QIAGEN PCR purification kit, separated by agarose gel electrophoresis to confirm a single product, and sequence verified (University Core DNA Services, University of Calgary). Chromatograms were analyzed to obtain SNP genotype. Genotype information was obtained for OXTR (rs237885) with the TaqMan SNP Genotyping assay (C___3290319_1_) method using the StepOnePlus Real-Time PCR system (ThermoFisher Scientific, Waltham, MA). Samples were run in duplicate along with negative and internal controls. Genotype results were read independently by two blinded individuals. Hardy–Weinberg equilibrium was evaluated for each SNP.
Statistical Analyses
All statistical analyses were performed using IBM Statistical Package for the Social Sciences (SPSS, version 24). We assessed univariate outliers using frequency tables of z scores and multivariate outliers by checking that no cases had a Cook’s value greater than one (Stevens, 1984). Although there were very few missing data points, a sensitivity analysis was carried out using multiple imputation, and the results corresponded to the complete case analysis. Therefore, missing values are not sensitive to the results, and complete case analysis was carried out. Normality for continuous variables was evaluated by the Shapiro–Wilk test and examination of frequency histograms and normal probability plots. Skewness and kurtosis were evaluated for continuous variables by ensuring that scores for skewness or kurtosis divided by their standard errors were less than or equal to ± 3.29 (Kim, 2013). Multicollinearity was assessed by ensuring no Conditioning Index values greater than 30 for any dimension along with no variance proportions greater than .50 for two or more different variables (Dormann et al., 2013).
To compare categorical demographic variables and distribution of genotypes between the high and low psychosocial distress groups, either Chi-square or Fisher’s exact tests were performed where appropriate. As maternal age was available as a continuous variable, a t test was performed to compare maternal age between the two groups. One-way analysis of variance (ANOVA) tests were conducted to evaluate the relationship between SNP genotype and score on the EPDS, SSAI, and PSS for both SNPs. Binary logistic regression was conducted using the demographic variables that were statistically significant (p ≤ .05) and the genotype variables.
Results
Demographic Characteristics of the High Prenatal Psychosocial Distress and Low Prenatal Psychosocial Distress Groups.

Note. N = 50; an = 49 due to missing data; bn = 48 due to missing data.
Analysis using continuous variable.
*Significant at p < .05.
Comparison of Range, Mean, and Standard Deviations of Scores on the EPDS, SSAI, and PSS between the Low and High Psychosocial Distress Groups.

Note. EPDS = Edinburgh Postnatal Depression Scale; SSAI = Spielberger State Anxiety Inventory; PSS = Perceived Stress Scale; SD = standard deviation. n = 25 low distress and n = 25 high distress. EPDS scores range from 0 to 30. SSAI scores range from 20 to 80. PSS scores range from 0 to 40. For all scales, higher scores indicate more distress.
Genotype Frequency and HWE.

Note: MAF = minor-allele frequency; HWE = Hardy–Weinberg equilibrium; SNP = single nucleotide polymorphism. FKBP5 = FK506 binding protein; OXTR = oxytocin receptor. n = 25 low distress and n = 25 high distress. HWE also not violated for high distress group or two groups analyzed together.
Descriptive Statistics and One-Way Analysis of Variance Scores Examining the Relationship between OXTR Genotype and Score on the EPDS, SSAI, and PSS.

Note. OXTR = oxytocin receptor; EPDS = Edinburgh Postnatal Depression Scale; SSAI = Spielberger State Anxiety Inventory; PSS = Perceived Stress Scale; SD = standard deviation. n = 12 (TT), n = 11 (GG), n = 27 (GT).
A binary logistic regression was performed to investigate differentiating participants with high and low prenatal psychosocial distress. Predictors included statistically significant demographic variables (income and maternal age) and information on genotype at the two SNPs. OXTR SNP (rs237885) was dummy coded with “TT” being the reference group. FKBP5 SNP (rs1360780) was dummy coded with “CC” being the reference group. Entry of the variables into the equation was simultaneous, controlling for income and maternal age. After deletion of two cases with missing values, data from 48 participants were available for analysis: 25 with high prenatal psychosocial distress and 23 with low prenatal psychosocial distress.
Binary Logistic Regression Model with Maternal Demographic Variables and SNP Genotype.
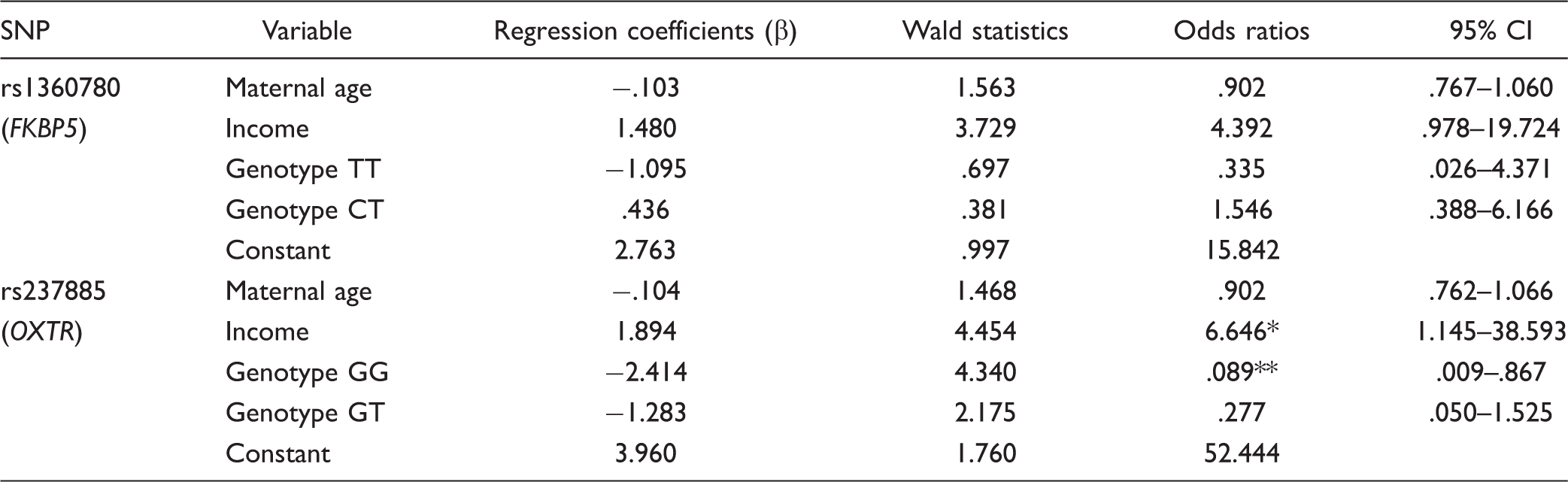
Note. CI = confidence interval; SNP = single nucleotide polymorphism; FKBP5 = FK506 binding protein; OXTR = oxytocin receptor.
p = .035. **p = .037.
For the OXTR SNP, a test of the full model with all three predictors against a constant-only model was statistically significant, χ2(4, N = 48) = 14.878, p = .005, indicating the three predictors, as a set, reliably distinguished between high and low prenatal psychosocial distress. The variance accounted for was 35.6% (Nagelkerke R2 = 35.6%). Overall prediction success was 68.8%, with 73.9% of participants with low and 64.0% of participants with high prenatal psychosocial distress correctly classified. Maximal discrimination between the groups occurred with a constant and only two predictor variables: income and OXTR SNP (see Table 5). In general, the odds of inclusion in the high psychosocial distress group are higher with self-report of lower income (p = .035) and lower with a “GG” genotype at the OXTR SNP rs237885 (p = .037).
Discussion
This proof of concept study offers pilot evidence for an association between a SNP in the oxytocin receptor and prenatal psychosocial distress. In addition, the results of this study provide further evidence for environmental factors previously linked to prenatal psychosocial distress.
In the current study, high prenatal psychosocial distress was associated with lower income and younger maternal age. A systematic review examining risk factors associated with antenatal depression and anxiety identified 15 other studies that found an association between low income and antenatal depression and anxiety versus three that did not (Biaggi et al., 2016). Maternal age is less consistently linked with maternal anxiety and depression, with almost equal numbers of studies identifying young age as a risk factor, old age as a risk factor, or finding no association with age (13 studies vs. 10 studies vs. 10 studies, respectively; Biaggi et al., 2016). Income is an important social determinant of health and even when income is sufficient for material necessities relevant to health, socioeconomic gradients can impact social factors related to health outcomes (Marmot, 2002). Current evidence, including the results of our study, point to the significance of relative socioeconomic circumstances as a contributing factor to maternal psychosocial distress.
No association was found between the FKBP5 SNP rs1360780 and prenatal psychosocial distress, which corresponds with the results of a FKBP5 SNP haplotype analysis conducted by Schneider et al. (2014). Nevertheless, as only one SNP was examined in this study, FKBP5 cannot be conclusively ruled out as being implicated in prenatal psychosocial distress. The results of this study reveal a statistically significant relationship between the “GG” genotype at the OXTR SNP rs237885 and self-report of low prenatal psychosocial distress. Prenatal depression was previously found to be associated with the OXTR SNP rs237885; however, the association was reverse to what was found in this study, with the “GG” genotype associated with high prenatal depression (Mileva-Seitz et al., 2013). The difference in the direction of association could be due to our study looking at the three different conditions as one phenotype versus depression alone, small sample size, or chance.
Plasma oxytocin levels are known to vary between individuals, and it has been suggested that high plasma oxytocin levels may serve as a buffer against the development of depressive symptoms in the face of high levels of psychosocial stress (Levine, Zagoory-Sharon, Feldman, & Weller, 2007; Zelkowitz et al., 2014). The function of OXTR SNP rs237885 is unknown, and it is possible that it is not functionally relevant, but rather in linkage disequilibrium with a functional SNP. There is evidence that OXTR SNP rs237885 is in linkage disequilibrium with OXTR SNP rs237887, located in an intron containing an active enhancer, and hypothesized to alter transcription-factor binding and cause altered gene expression (Skuse et al., 2014). Further research is needed to clarify whether genetic variations in the oxytocin system contribute to the development of prenatal mental health issues.
Limitations
This study was a proof of concept pilot project with small sample size and analysis of only two selected SNPs. As the sample used for this study was not limited to one self-reported ethnicity and allele frequencies can vary between ethnic groups, results should be strengthened and validated using a larger, homogeneous sample. Results of this study will inform a larger study incorporating more environmental variables and additional (pathway/oxytocin/OXTR) relevant SNPs that could lead to more information about the genetic contribution to prenatal psychosocial distress. Increasing the scope of investigation will enable separate analysis of depression, anxiety, and stress and perhaps identify distinct roles for each.
Conclusion
Despite these limitations, we demonstrated the feasibility of the project and found a statistically significant relationship with prenatal psychosocial distress for maternal age, income, and the OXTR SNP rs237885. Further study is needed with a larger sample to clarify the potential role of oxytocin receptor SNPs and other candidate genes in the etiology of prenatal psychosocial distress. Establishing genetic and gene by environment links to prenatal psychosocial distress will enable the expansion of explanatory models and lead to the development of more precise interventions and improved treatment for an area of health care that has been neglected (Glover, 2014). Understanding the complex interactions and mechanisms that explain outcomes allows nurses to have a more complete foundation when advocating for support and services for families (Letourneau, Giesbrecht, Bernier, & Joschko, 2014).
Footnotes
Acknowledgments
The authors thank Indiana Best for her help in the laboratory. The authors would also like to thank and acknowledge the All Our Families Study participant families and research team members, especially Mary Canning, Nikki Stephenson, and Muci Wu. The authors are extremely grateful to the All Our Families investigators, coordinators, research assistants, graduate and undergraduate students, volunteers, clerical staff, and managers.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All Our Babies funded through Alberta Innovates Health Solutions Interdisciplinary Team Grant #200700595. Pilot project funded by internal grant from the Faculty of Nursing, University of Calgary.