
Abstract
Abstract Background
Although a majority of nurses understand that delirium is a major issue in perioperative care, professional barriers to routine monitoring using delirium assessment tools exist. The aim of this study was to assess the effectiveness of continual monitoring of postoperative delirium in patients that have undergone esophagectomy using the Neelon and Champagne (NEECHAM) Confusion Scale (NCS).
Methods
Demographic data and case histories were obtained from medical records. We conducted NCS scoring for 1 week after surgery and verified the daily changes in scores. Patients were classified into normal, neurocognitive-change, and complication groups for the analysis of the influence of preoperative neurocognitive changes and postoperative complications.
Results
Data from 19 patients were analyzed. NCS scores decreased sharply on the first day and then significantly recovered each day. The normal group exhibited a steady recovery process, but the other groups deviated from this progression. The incidence of delirium was highest on the first day. The incidence in the normal group decreased each day, but other groups developed delirium for an extended time. In the NCS subscale score analyses, the information processing score was low in the neurocognitive-change group. The complication group exhibited delayed recovery of the physiologic control score.
Conclusions
We observed the recovery process of mental function after esophagectomy as well as the impact of preoperative neurocognitive changes and postoperative complications. Continual monitoring of postoperative mental function may predict postoperative delirium. For early detection and prevention of delirium, nurses should monitor postoperative mental function via daily observation.
Introduction
Surgical resection is the primary treatment option for esophageal cancer (Ng & Vezeridis, 2010); however, it is a highly invasive procedure associated with high morbidity and mortality. The reported postoperative morbidity rates range from 45% to 80%, even in high-volume centers (McCulloch, Ward, & Tekkis, 2003; Putnam et al., 1994; Yoshida et al., 2014). Postoperative delirium developed in 153 (50.0%) of 306 patients who underwent esophagectomy in a study conducted in Japan (Takeuchi et al., 2012). Moreover, delirium is associated with poor outcomes and high costs (Lee and Kim, 2014; Markar, Smith, Karthikesalingam, & Low, 2013; O’Mahony, Murthy, Akunne, & Young, 2011).
Postoperative delirium is an acute brain dysfunction that occurs because of surgical stress. It is a transient disturbance of consciousness accompanied by inattention, disorganized thinking, and an altered level of consciousness (Ely et al., 2004; Van Rompaey et al., 2009). Generally, the cause of delirium is multifactorial (Inouye & Charpentier, 1996). Among various factors, cognitive impairment is the leading risk factor for delirium (Dasgupta & Dumbrell, 2006; Inouye, 2006). In addition, the occurrence of postoperative complications is associated with postoperative delirium (Greene et al., 2009; Markar et al., 2013; Takeuchi et al., 2012).
Delirium can be classified as hyperactive, hypoactive, or mixed type; 50% of postoperative delirium consists of the hypoactive type (Whitlock, Vannucci, & Avidan, 2011). The hyperactive type is readily recognized during the course of routine care, but hypoactive delirium is more likely to remain undiagnosed because of its calm clinical manifestation (Guenther et al., 2012; Peterson et al., 2006).
To detect postoperative delirium, the Society of Critical Care Medicine recommends routine monitoring of adult intensive care unit (ICU) patients in their guidelines (Barr et al., 2013). The following six tools have been identified to evaluate delirium in the ICU (Devlin, Fong, Fraser, & Riker, 2007):
Cognitive Test for Delirium (CTD) The abbreviated version of the CTD Confusion Assessment Method-ICU (CAM-ICU) Intensive Care Delirium Screening Checklist (ICDSC) Neelon and Champagne (NEECHAM) Confusion Scale (NCS) and Delirium Detection Score
Among these, the guideline reported that the CAM-ICU and ICDSC are the most valid and reliable tools. However, nurses are unfamiliar with performing a semidiagnostic assessment, such as the CAM-ICU; in addition, they may be concerned that the questioning procedure could potentially distress the patients (Oxenboll-Collet, Egerod, Christensen, Jensen, & Thomsen, 2016). Although early detection of postoperative delirium is considered the critical concern, the clinical efficacy of routine monitoring of delirium has not yet been established (Bigatello et al., 2013). Therefore, some medical professionals feel that delirium guidelines are inconvenient to implement in daily practice (Andrews, Silva, Kaplan, & Zimbro, 2015; Trogrlic et al., 2016).
The NCS was developed for rapid and unobtrusive assessment of acute confusion. This scale is designed for frequent retesting and uses only observational information. Compared with the other five tools, the NCS is best suited to assess the risk of developing delirium. The NCS can show daily changes in risk and it is helpful for monitoring developing or worsening acute confusion (Neelon, Champagne, Carlson, & Funk, 1996). In addition, this scale can screen patient status with little stress on either seriously ill patients or busy nurses (Immers, Schuurmans, & Van de Bijl, 2005). The Japanese version of the NCS has been confirmed to have high reliability (Watanuki et al., 2001).
The aim of this study was to determine the efficacy of daily monitoring of the risk of developing delirium in patients after esophagectomy using the NCS.
Methods
Subjects
Adult patients who underwent esophagectomy with two- or three-field lymph node dissection at one university hospital from January to September 2013 were included. We selected patients who were sufficiently capable of linguistic communication and able to provide written informed consent for study entry.
Data Collection
We collected the following data from the medical records:
Patient age Patient sex History of neurocognitive disorders, Preoperative blood test data Operative method Operative time Intraoperative blood loss Occurrence of postoperative complications and Occurrence of postoperative delirium
Postoperative complications were classified according to the Clavien–Dindo Classification (Clavien, Sanabria, & Strasberg, 1992). Postoperative delirium was diagnosed based on the Diagnostic and Statistical Manual of Mental Disorders-IV-TR (DSM-IV-TR) criteria.
NCS Scoring
Each Component and Score Allotment of the NEECHAM Confusion Scale.
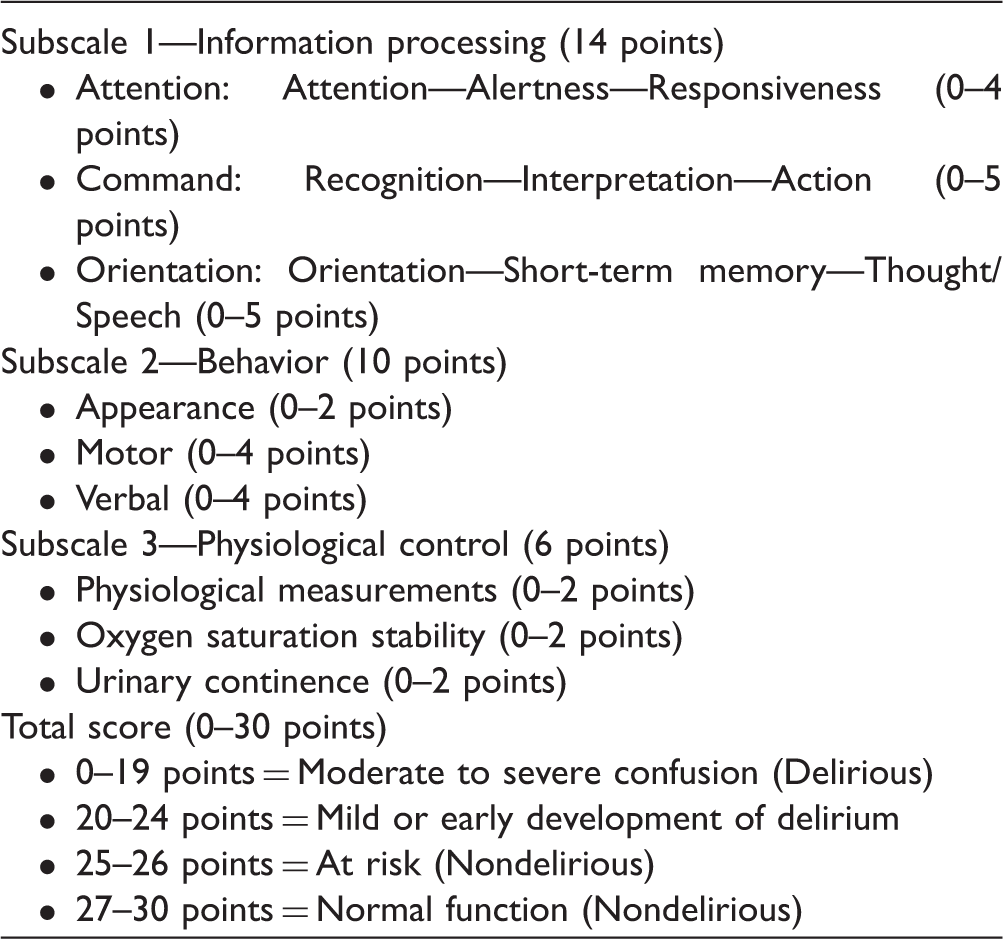
We used the NCS score as an indicator of mental function in postoperative patients. Because the NCS cannot be applied to intubated patients, the investigation was performed for 1 week after extubation. A trained nurse researcher rated the NCS once to obtain the baseline value before surgery. After the operation, the NCS was scored during the daytime for 7 days after extubation.
Classification of the Patients
We divided patients into three groups to assess the impact of preoperative neurocognitive changes and postoperative complications on mental function. Patients who had a history of neurocognitive disorders were categorized into the neurocognitive-change group. Patients who developed postoperative complications corresponding to Clavien Grades II to V were categorized into the complication group. Patients who had neither of these were categorized into the normal group.
Data Analysis
We performed the statistical analyses using IBM SPSS Statistics 20. We used the Wilcoxon signed-rank test to evaluate the changes in the NCS score on each day. We also used Mann–Whitney U test and analysis of variance with the Scheffe post hoc test to analyze the differences in the NCS score in each group.
Ethical Consideration
This study was implemented with the approval of the ethics committee of Osaka university hospital.
Results
Demographic Data.
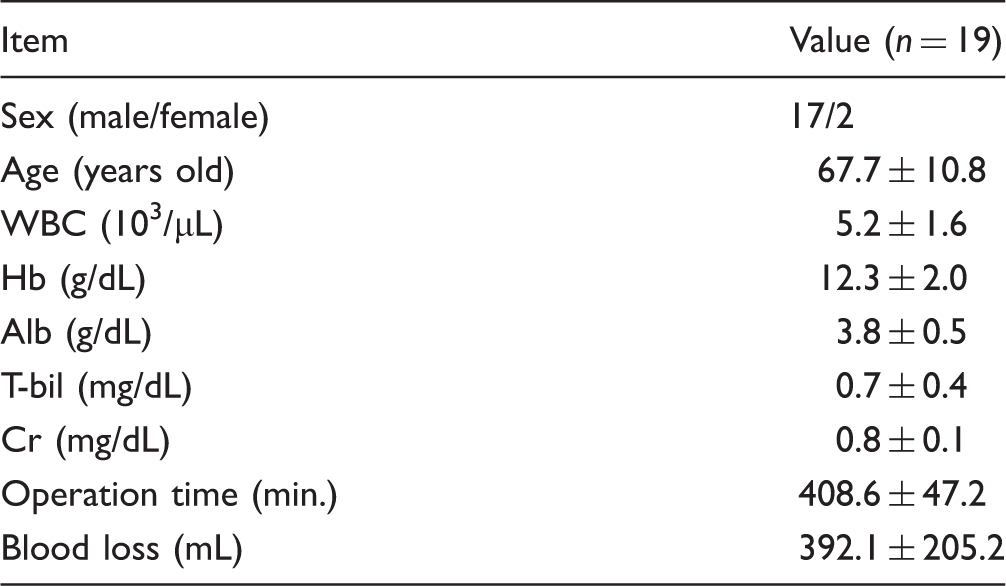
Note. Continuous variables are expressed as means ± SD.
One patient was preoperatively diagnosed with mild cognitive impairment, and normal pressure hydrocephalus was suspected. Two additional patients had a history of cerebral infarction but did not manifest any cognitive problems. These three patients had no problems with activities of daily living and were categorized into the neurocognitive-change group. Postoperatively, one patient developed a catheter-associated bloodstream infection on Day 2, and another patient developed postoperative pneumonia on Day 4. These two patients were assigned to the complication group. The remaining 14 patients comprised the normal group.
Incidence of Delirium
Incidence Rate of Postoperative Delirium.
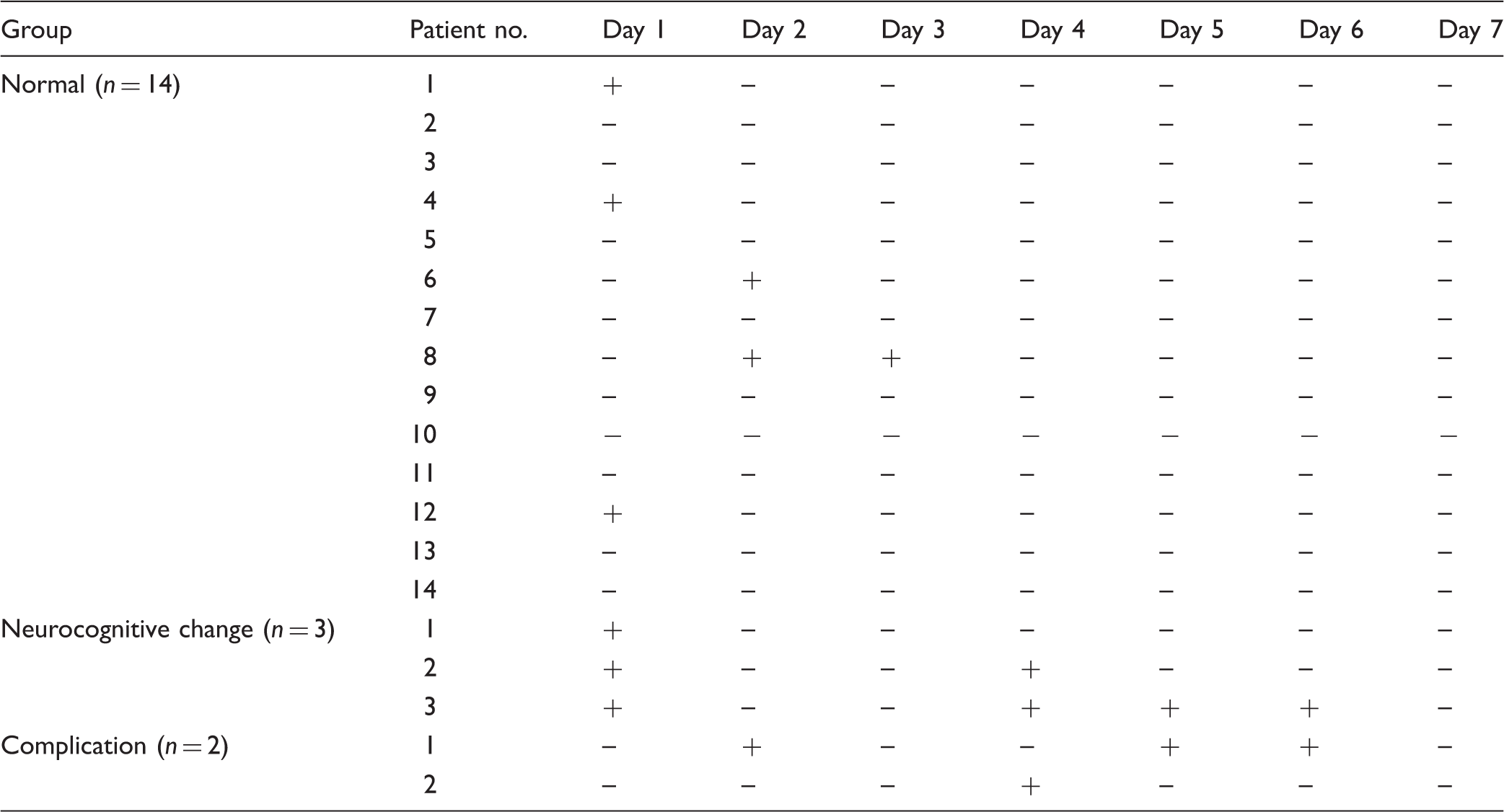
Note. + = Diagnosis of postoperative delirium by the doctor in charge; − = No diagnosis of postoperative delirium by the doctor in charge.
NCS Score
On the preoperative NCS assessment, all 19 patients scored 30 points (full score), including the patients with mild cognitive impairment. The NCS score of all patients decreased to less than 24 points, which indicates mild confusion, on Day 1. Then, the NCS scores significantly recovered from Day 1 to Day 7 (Figure 1a). The NCS score of patients developing delirium was significantly lower compared with that of nondelirium patients throughout the study period (Figure 1b).
Changes in the NCS score. The Wilcoxon signed-rank test was used to analyze the daily changes in NCS scores in all patients (a). Mann–Whitney U test was used to analyze the difference in NCS scores between delirium patients and nondelirium patients (b). *p < .05, **p < .01. NCS = Neelon and Champagne (NEECHAM) Confusion Scale.
In intergroup comparison, the total score of the normal group decreased to 20.9 points on Day 1 and then increased to more than 25 points, which indicates nonconfusion, on Day 3. The normal group score steadily recovered to the preoperative level. The score in the neurocognitive-change group decreased to less than 19 points, which indicates moderate to severe confusion, on Day 1, and the score recovery was significantly delayed. The average score of the neurocognitive-change group did not rise above 25 points on Day 7. In the complication group, NCS score recovery was similar to that of the normal group within the first three days but then the recovery slowed (Figure 2).
Changes in the NCS score in each group. Analysis of variance was used to analyze the difference in NCS scores in each group. Significant differences were found on Day 3 to Day 5 and Day 7 between the normal group and the neurocognitive-change group and on Day 6 to Day 7 between the normal group and the complication group using the Scheffe post hoc test. *p < .05, **p < .01. NCS = Neelon and Champagne (NEECHAM) Confusion Scale.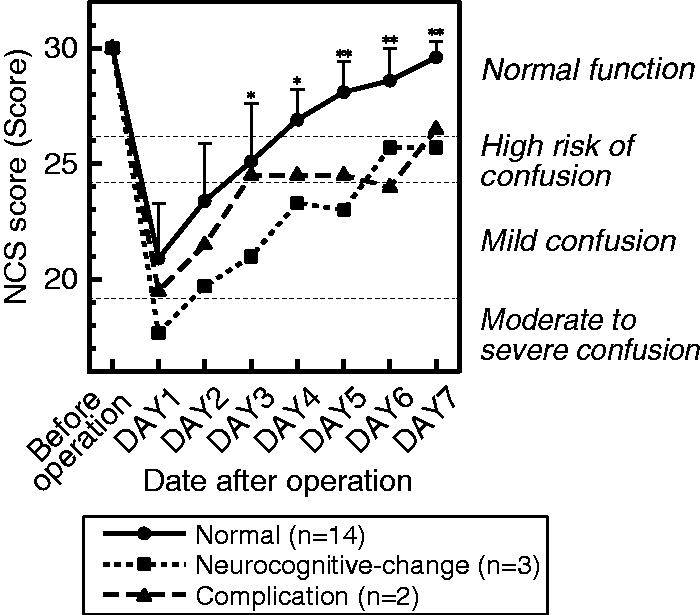
In the analysis of each NCS subscale score, the recovery of information processing scores was delayed in the neurocognitive-change group (Figure 3a). Although all the patients in the normal group scored 14 points (full score) after Day 5, two of the three patients in the neurocognitive-change group scored 11 to 12 points, even on Day 7. In contrast, the recovery of the physiologic control score was delayed in the complication group (Figure 3b). The behavior index score showed a pattern similar to that of the total NCS score.
Changes in the subscale scores of the NCS in each group. Analysis of variance was used to analyze the differences in the NCS subscale scores in each group. For the information processing score, significant differences were found on Day 3 to Day 7 between the normal group and the neurocognitive group using the Scheffe post hoc test (a). For the physiologic control score, significant differences were found on Day 7 between the normal group and the complication group using the Scheffe post hoc test (b). *p < .05, **p < 0.01. NCS = Neelon and Champagne (NEECHAM) Confusion Scale.
Discussion
In all patients, the NCS score decreased to 24 points or less on Day 1, which suggested confusion. Furthermore, the average NCS score of patients developing delirium decreased to 18.8 points, which indicates delirium on Day 1. This reduction in score indicates that patients who undergo highly invasive surgery such as esophagectomy may develop postoperative delirium. Moreover, 6 of 19 patients developed delirium based on the DSM-IV-TR on Day 1. This was the highest incidence rate of delirium during the 7 days assessed. After extubation, inadequate emergence often occurs because of influence by the sedation during ventilation (Hove, 2010). The delirium developed in this period is called emergence delirium. Emergence delirium is a known complication in pediatric anesthesia, but emergence delirium in adult patients is less known (Radtke et al., 2010). This phenomenon suggests that delirium occurs most often on the day of extubation among esophageal cancer patients. Therefore, delirium should be carefully monitored with frequent NCS retesting on the extubation day.
In the normal group, the NCS score gradually returned to the preoperative level 1 week after the decrease observed on Day 1. The incidence rate of delirium also decreased according to NCS score recovery. In other groups, the changes in the NCS score were different from the recovery process of the normal group, and patients developed delirium. These results suggest that monitoring the changes in postoperative mental function may predict the risk of developing delirium.
In the neurocognitive-change group, the total NCS score was significantly decreased compared with the normal group on Day 1. In addition, a score below 25 points persisted longer in this group than in the normal group. All three patients developed delirium on Day 1, and two of the three patients in this group developed delirium again after Day 4. We found that the information processing score played a major role in this result. It is thought that preexisting cognitive impairment status makes patients more vulnerable to developing postoperative delirium (Robinson & Eiseman, 2008; Van Rompaey et al., 2009). Although two of the three patients in the neurocognitive-change group did not exhibit any cognitive problems preoperatively, all patients developed delirium on Day 1. Beason-Held noted that patients with cognitive impairment show organic brain changes that occur years before the onset of cognitive symptoms (Beason-Held et al., 2013). Root suggests that preoperative white matter pathology in the brain predisposes patients to a greater risk of postoperative delirium (Root et al., 2013). Even if a patient does not show clear signs of cognitive impairment preoperatively, a suspected neurocognitive change, such as a history of cerebral infarction, is thought to increase the risk of postoperative delirium.
The NCS score of the complication group recovered in a manner similar to the normal group during the first three days, but the recovery deviated thereafter. Neither of the two patients exhibited delirium symptoms on Day 1, but they developed delirium following fever because of postoperative infection. In contrast to the neurocognitive-change group, the physiologic control score, rather than the information processing score, was low in this group. If a patient is recovering well from the initial surgery, secondary damage because of postoperative complications may cause postoperative delirium. Postoperative complications predispose patients to an additional risk for postoperative delirium.
Although the recognition of delirium is a critical issue, delirium is often undiagnosed (Robinson & Eiseman, 2008). The American Association of Critical-Care Nurses (AACN) recommends implementation of the Awakening and Breathing Coordination, Delirium Monitoring and Management, and Early Mobility bundle for delirium management in the ICU (Balas et al., 2012). In relation to delirium monitoring, AACN ensures once-per-shift delirium assessment using a validated tool like CAM-ICU or ICDSC (AACN, 2012). Nurses play an important role in predicting delirium (Inouye, Foreman, Mion, Katz, & Cooney, 2001). A nurse’s role in delirium monitoring is to monitor and determine the “possibility” of delirium occurring during the recovery process of mental function. If nurses are alert to the early signs of developing delirium, preventive care can be provided. Even if delirium is only suspected, the physician may make a definitive diagnosis of delirium and treat it early based on the information provided by observant nurses. While the CAM-ICU is a good tool for the diagnosis of delirium (Gusmao-Flores, Salluh, Chalhub, & Quarantini, 2012), it is difficult to monitor condition changes in mental function. Compared with the CAM-ICU, the NCS has good retest utility (Neelon et al., 1996) and can assess the risk of developing delirium. This strong point is valuable for the early detection of delirium in nonintubated patients (Van Rompaey et al., 2008).
Our study has several limitations. First, this is small sample study in a single medical institution, and our results, especially comparisons among three groups, are therefore not generalizable. Second, the NCS was developed in general hospital population (Neelon et al., 1996). While this scale has been validated for use in ICU patients (Csokasy, 1999), it cannot be used in intubated patients. To solve this problem, we are currently developing a new tool for postoperative mental function monitoring by continuous nursing observation.
In conclusion, we presented the typical recovery process of mental function after esophagectomy. The continuous monitoring using NCS could identify the high risk of developing delirium. If we assess the change of mental function continuously, we may provide care that enables patients to trace a smooth recovery process and patients’ outcomes such as length of stay will improve. The impact of preoperative neurocognitive change and postoperative complications would become an indication of deviation from the recovery process. To prevent postoperative delirium, it is important that nurses perform continual monitoring with bedside observation to assess the change of postoperative mental function.
Footnotes
Acknowledgments
We are grateful for the support provided by all medical staff in the intensive care unit and surgical ward of Osaka University Hospital. We also express our appreciation to the patients in the study and their families.
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a JSPS Grant-in-Aid for Scientific Research (Grant Number 26861902).