
Abstract
Background
Shared decision-making (SDM) is supposed to position patient and expert knowledge more equal, in which will have an impact on how mental health-care professionals relate to their patients. As SDM has not yet been widely adopted in therapeutic milieus, a deeper understanding of its use and more knowledge of interventions to foster its implementation in clinical practice are required.
Aim
To explore how mental health-care professionals describe SDM in a therapeutic milieu as expressed through clinical supervision. The research question was “What are prerequisites for mental health-care professionals to practice SDM in a therapeutic milieu?”
Methods
A qualitative content analysis of data from focus groups dialogues in 10 clinical supervision sessions where eight mental health-care professionals participated was performed.
Findings
The theme, practicing SDM when balancing between power and responsibility to form safe care, was based on three categories: internalizing the mental health-care professionals’ attributes, facilitating patient participation, and creating a culture of trust.
Conclusion
SDM is a complex and arduous process requiring appropriate interventions. Clinical supervision is necessary for reflection on SDM and for improving practice in a therapeutic milieu.
Keywords
Introduction
High-quality care should be a common goal for all mental health-care professionals, and patient participation is argued to be an important element in high-quality services (Rise, Westerlund, Bjorgen, & Steinsbekk, 2014). A recommendation in Norwegian White Papers (Norwegian Ministry of Health & Care Services, 2008–2009; Norwegian Ministry of Health & Care Services, 2012–2013) is that the patient perspective should be taken into account in the planning and implementation of treatment. The therapeutic milieu in mental health wards is based on relational treatment, the main focus of which is the use of relationships to alleviate relational harm. Daily life and activities are lived in a healing culture, rich in therapeutic interpersonal relationships and cooperative attentiveness to patients (Long, Knight, Bradley, & Thomas, 2012; Mahoney, Palyo, Napier, & Giordano, 2009).
Shared decision-making (SDM) is a care model facilitating patient involvement (Dierckx, Deveugele, Roosen, & Devisch, 2013) by adjusting the asymmetrical power balance between patients and mental health-care professionals. As SDM has not yet been widely adopted in therapeutic milieus, a deeper understanding of its use and more knowledge of interventions to foster its implementation in clinical practice are required (Gravel, Légaré, & Graham, 2006; Perestelo-Perez, Gonzalez-Lorenzo, Perez-Ramos, Rivero-Santana, & Serrano-Aguilar, 2011). A prerequisite for implementing SDM in care settings is that mental health-care professionals have the ability and are willing to include the patient in decisions (Grim, Rosenberg, Svedberg, & Schön, 2016).
This quality improvement study contributes to new knowledge of prerequisites for mental health-care professionals to practice SDM in a therapeutic milieu as expressed through clinical supervision. Clinical supervision is a way of creating a culture where a process of sharing, learning about, and reflecting on clinical experiences of patient–mental health-care professionals interaction enhances the professional development of mental health-care professionals (Berggren & Severinsson, 2011). The purpose of clinical supervision is to improve practice (Brunero & Stein-Parbury, 2008) by means of a forum where questions about how to perform high-quality work are raised and safe work practices studied in order to learn from everyday situations (Brunero & Lamont, 2012). Mental health-care professionals attending clinical supervision are supposed to improve SDM (Berggren & Severinsson, 2011; Brunero & Stein-Parbury, 2008). Clinical supervision outcomes are shown to include “changing organization of care, confirmation of nursing interventions, problem solving, and improving and confirming practice” (Brunero & Stein-Parbury, 2008, p. 93), in which the approach of clinical supervision turns to be a suitable tool for strengthening SDM in a therapeutic milieu.
Review of Literature
In Norway, the health and care service legislation strongly supports patient participation (Norwegian Ministry of Health & Care Services, 2012–2013) which means to acknowledge the patients’ experience and knowledge of their right to participate in their health, and to position patient and expert knowledge more equal (Solbjør, Rise, Westerlund, & Steinsbekk, 2011). However, the power balance between patients and mental health-care professionals needs to be adjusted, which will have an impact on how mental health-care professionals relate to their patients. SDM consists of five elements: active participation between patients and mental health-care professionals, information sharing, problem definition, deliberation about treatment options, and finally, a decision or deferment (Charles, Gafni, & Whelan, 1997). The interaction between the patient and mental health-care professionals should be characterized by an equal division of power between the parties, a negotiated agenda, and exploration of the patient’s values, with mental health-care professionals playing an advisory role regarding the patient’s goals and decisions (Elwyn et al., 2009). Practices with standardized procedures and guidelines are dominated by the expert power, and become challenged by this equal power relationship on which SDM builds on (Grim et al., 2016).
In mental health-care, some patients are considered incapable to act in their best interest. Both health-care professionals and patients have characterized SDM as challenging during episodes of mental illness, as the patients may have phases with lack of insight, difficulties in communication and cooperating disabilities. Solbjør et al. (2011) reports that this requires mental health-care professionals having the sensitivity and the insight to facilitate SDM in ways that safeguard patients in all phases of illness. Despite the fact that there has been a great deal of focus on SDM in mental health care, many patients continue to express a desire for more active involvement in their treatment (Angell, Matthews, Stanhope, & Rowe, 2015). This means that mental health-care professionals need to improve their work of facilitating SDM, in which involves an ongoing reflection on and assessment of the patient’s resources, limitations, and need for assistance (Kontio et al., 2010).
The aim of this study was to explore how mental health-care professionals describe SDM in at therapeutic milieu as expressed through clinical supervision.
Methods
Study Context
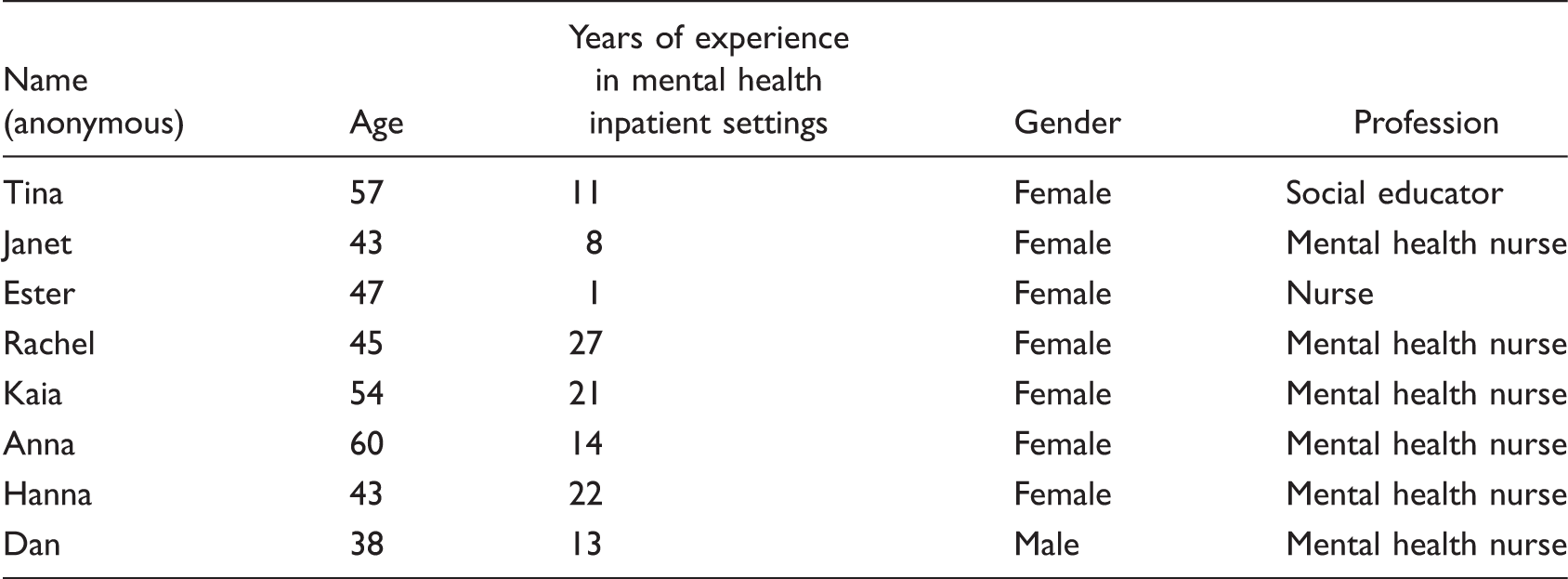
The context of this study was the therapeutic milieu in three different wards in a community mental health center in Norway, possessing a total of 30 beds. This is an autonomous professional unit responsible for general mental health services in a distinct geographic region. Mental health-care professionals working in the therapeutic milieu possess various professions, mostly bachelor degree in nursing or as a social educator, some with a specialized education in mental health care. Because of lack of mental health-care professionals, unskilled assistants are working in this clinical context. A total of 105 employees are connected to the 30 inpatients in the three wards in permanent positions or as stand-in, covering 24 hours a day, 7 days a week. The patients have various mental health problems, suffering from different mental illnesses which makes them in need of being inpatient in a period of time, short or long term.
Study Design and Supervision Program
A qualitative study with an explorative and descriptive design was chosen (Polit & Beck, 2010) in order to gain a deeper understanding of SDM as described by mental health-care professionals working in therapeutic milieu. The researchers designed a 10-session supervision program based on knowledge of core phenomena in clinical supervision (Holm Wiebe, Lindquist, & Severinsson, 2011). This formed the basis for the data collection by facilitating in-depth dialogues that addressed the research question. The principles of a supportive and nurturing relationship (confirmation, understanding, empathy, presence, creating trust, and security) presented by Holm Wiebe et al. (2011) formed the basis of the 10 sessions, and their principles related to the supervision space (storytelling, sharing and reflection, acting, and challenges) were adhered to at all times. These elements were equally important for collecting in-depth data by means of dialogues (Polit & Beck, 2010). The main topics addressed in the clinical supervision were the mental health-care professionals–patient relationship and SDM in the therapeutic milieu. The mental health-care professionals reflected on what SDM means in various situations, using examples from their everyday practice. Knowledge development took place when mental health-care professionals who were attending clinical supervision shared their experiences and viewpoints, in addition to being open to the various perspectives of their fellow supervisees.
The research question was: “What are prerequisites for mental health-care professionals to practice SDM in a therapeutic milieu?”
Participants
Description of Participants.
Data Collection
Focus group discussion in clinical supervision was employed to collect the qualitative data (Colucci, 2007; D. L. Morgan, 1996). The topics were determined by the researchers ahead of the sessions. This technique used the group interaction on the specified topic focusing on the research interest (D. L. Morgan, 1996). In this way, we formed the focus group in a way that adhered to the aim of the study. According to D. L. Morgan (1996), more creative uses and formats for focus groups remain to be discovered.
D. L. Morgan (1996) argues that focus groups as a data-collection tool are influenced by participants’ reliance on the researcher and the interaction, and that this has a direct impact on the project’s strength or weakness. In the current study, the participants and researchers became familiar with each other as a consequence of several meetings. No conflicts between the participants and the researchers were determined, and the dialogues that took place in the sessions were characterized by an open, engaged, and curious atmosphere. This attitude seemed to enhance the participants’ will to share experiences from their clinical field (cf. D. L. Morgan, 1996).
The first (LB) and last author (KR) acted as moderators. We always started the sessions with some evaluation from last time, an introduction of todays’ topic, and thereafter the reflection in the group. The sessions always ended with an evaluation of today’s session. By holding this routine, the form of the sessions became predictable and was a way for the moderators to find an appropriate way of approaching the participants. We tried to use the activity-oriented questions to encourage the discussion; “Activity-oriented questions can also be appropriate to talk about sensitive topics, which may look less threatening when discussed through practical and enjoyable tasks” (Colucci, 2007, p. 319).
The sessions, each of which lasted for 1.5 hr, were performed every second week between February and June 2016. All sessions were audio-taped and transcribed verbatim, and the dialogues were used as data for the study. Two of the four authors were involved in the clinical supervision group, which provided proximity to real-life situations. By having proximity to real-life situations, the researchers can understand the participants’ views and become involved with them, thus creating a trusting relationship that enables the participants to feel safe enough to share their experiences and provide a rich data set (M. S. Morgan, 2015). To ensure that the data were as genuine and trustworthy as possible, the researchers were aware of and reflected on their own preunderstandings and how they could affect the participants, while at the same time remaining open to other possibilities of understanding (Graneheim, Lindgren, & Lundman, 2017).
Qualitative Content Analysis
The qualitative content analysis was performed at a descriptive manifest level (Graneheim et al., 2017). An inductive approach, with a search for patterns in the text, was employed in order to illuminate the mental health-care professionals’ views as a whole (Graneheim et al., 2017; Lincoln & Guba, 1985). The authors searched for variations in the data material by identifying similarities and differences in the text, which were presented in the form of theme, categories, and subcategories on various levels of abstraction and interpretation. The analysis was conducted in three steps after the conclusion of the 10 supervision sessions: In Step 1, the transcribed text was read and listened to several times in order to gain a sense of the whole, after which the content was divided into meaning units that were then condensed and labeled with a code. In Step 2, the various codes were compared and sorted into categories, which constituted the manifest content. In Step 3, the codes and categories were compared and organized into three categories, each of which was based on two subcategories. The categories were abstractions of the linked subcategories. The data became clearer and a new understanding emerged as a result of the process of temporal distance, when feelings and experiences from the data collection grew more distant. The categories were validated and the abstractions of the data were reflected on and discussed by the four authors with focus on how to discover and understand their meaning. As a final point, the content in the three categories were interpreted and integrated in one theme (Graneheim et al., 2017).
The authors’ preunderstandings were related to their experience as clinical nurses, clinical supervisors, and researchers, while three of the authors (LB, KR, and ES) are registered mental health nurses and have several years of clinical experience caring for mentally ill people.
Ethical Considerations
This study was carried out in accordance with the Declaration of Helsinki (World Medical Association, 2013) and has been approved by the Regional Ethics Committee of Western Norway (2015/1721). A guarantee of anonymity and confidentiality was given to all participants and their written consent was obtained. The participants’ role as clinical supervisees exposed them in the sense that they became emotionally involved by sharing personal experiences in the group. All data were treated confidentially, kept securely locked away, and only used for research purposes.
In addition, the participants were informed about the aim of the study and that they could withdraw their consent at any time without any negative consequences. The researcher did not ask for sensitive information during the interviews (International Committee of Medical Journal Editors, 2017; World Medical Association, 2013). The mental health-care professionals were closely monitored in the supervision group by being asked how they experienced participating in the clinical supervision sessions.
Findings
Theme, Categories, Subcategories, and Condensed Meaning Units.

Practicing SDM When Balancing Between Power and Responsibility to Form Safe Care
The theme reflected the participants’ experiences of being in a dynamic process together with their patients. Mental health-care professionals should safeguard patients’ participation and sense of control at the same time as they ensure good recovery conditions. Both mental health-care professionals and patients have power and responsibility for SDM, where the power and responsibility should be balanced in a way that forms patient recovery and safety. The participants experienced that SDM was a dynamic process where they continuously should assess the patient’s insight and ability to take responsibility for own choices, securing that the patient was of no danger for oneself or others. In such phases, the participants saw it as their mission to compensate for the power and responsibility the patient is unable to maintain. The participants took charge by providing information, encouraging their patients, and reducing choices, as they safeguarded the patient by showing dignity and respect. Some of the participants described that when the patient recovers and is no longer in danger for oneself or others, the power and responsibility is given back to the patient. They stated that the balance between power and responsibility should be perceived to be the patient’s best interest at all times. Practicing SDM when balancing between power and responsibility to form safe care seemed to be a red thread throughout the data and the subcategories represent different aspects of the prerequisites for SDM in a therapeutic milieu.
Internalizing the Mental Health-Care Professionals’ Attributes
The first category describes the importance of mental health-care professionals possessing a high level of professional skills and being attentive to patients in order to achieve a balance between power and responsibility in SDM, thus forming safe care.
The participants reflected on how making use of professional skills implied professional knowledge on the part of mental health-care professionals: “If we haven’t enough knowledge about the problems the patient is struggling with he will not get the help he needs and it could threaten patient participation” (Anna, Session 5).
Mental health-care professionals’ attitudes, values, and way of being influenced the patients. The interpersonal competence is an important part of the professional skills and was experienced as challenging to improve because it is mostly grounded in automated and unconscious features.
By being attentive to the patient, the mental health-care professionals experienced that they should invite the patients to participate in a dialogue in order to become more aware of what is beneficial for them, in which implied that mental health-care professionals understand the patients and can intervene in accordance with their understanding: I didn’t know the patient well and a violent situation occurred. In retrospect we can understand what led to the patient’s violent reactions. When we have built a relationship we notice signs of violent reactions earlier and can intervene to avoid them (Rachel, Session 2).
Facilitating Patient Participation
The participants reflected on a variety of experiences when facilitating patient participation. They described how some patients want mental health-care professionals to know what is best for them and make them healthy without becoming involved themselves. The participants described that they found this problematic because they could not find themselves able to know what was the best for each patient without getting the patient’s point of view. They considered it their responsibility to take the initiative to facilitate patient participation, however, they found it challenging to assess how much and in what way each patient is capable to participate in different situations and with differing levels of engagement. Facilitating patient participation comprises stimulating patient involvement and acknowledging the patients’ process of participation.
The theme stimulating patient involvement concerned being trustworthy, honest, and always showing respect for the patient’s feelings. Maintain a trusting relationship with the patient through challenging situations requires mental health-care professionals being aware of their own emotions and thoughts and processing these so that they are able to balance between supporting the patients and encouraging them to cope with challenges in a way that facilitate patient participation. The participants stated that in their experience, confirming patients is very important for stimulating involvement in their own treatment. One participant commented: “Acknowledging patients’ knowledge of their own lives helps to create a good relationship. You show that you care about what they need for recovery” (Ester, Session 2).
Predictability was highlighted as important for stimulating patient involvement. Unexpected interventions without their involvement can make patients lose faith in SDM. How predictability is ensured was described as follows: The patient is involved in making a plan for how to deal with similar crises at a later stage. In that way, she knows what will happen next. The plan will be evaluated together with the patient on a regular basis, which means that the patient has ownership of her treatment plan (Janet, Session 3). “Sometimes we must help and protect patients against their will. In retrospect, they feel ashamed and thank us for taking over” (Dan, Session 5).
The participants described that patient involvement can vary over time; sometimes the patients have the strength to participate, while on other occasions they need the mental health-care professionals to take over. Acknowledging this process was considered important for balancing between power and responsibility.
Mental health-care professionals being able to encounter the patients where they stand was experienced as crucial when facilitating patient participation, and this insight needs high expertise to convey.
Creating a Culture of Trust
When reflecting on the fact that many mental health-care professionals work in the therapeutic milieu at different times with the same patients, the participants reported that creating a culture of trust is essential in order to maintain the balance between power and responsibility to form safe care. According to the participants, the prerequisites for creating a culture of trust are applying guidelines in a person-centered way and standing together as a team.
Applying guidelines in a person-centered way was reported as challenging. The participants experienced that SDM is hindered by the procedures and structure of the ward. If mental health-care professionals adhere to checklists and procedures for their own sake without taking account of the patients’ recovery process, the participants believed that a culture of trust would fail to emerge. Checklists do not help when mental health-care professionals know that something is not right. In such situations, they have to act on their intuition in a way that enhances patient well-being. One participant shared the following experience: The doctor said the patient was fine, but we were very familiar with the patient and knew that he was not well. To protect the patient, we acted against the doctor’s orders and ran to the patient to secure him. It led to a long hospitalization but prevented the patient from taking his own life (Janet, Session 9).
The participants discussed their concern about situations in which there is a failure to create a culture of trust and where the conditions for SDM are difficult. They experienced that colleagues’ expectations of mental health-care professionals professionalism can hinder patient participation: “Therapists may be hesitant to let patients find the solution themselves because it can challenge the professionalism expected of a good therapist” (Kaia, Session 1).
Having a dialogue with the colleagues about expectations was experienced to promote a culture of trust, which was seen as prerequisites for SDM.
Sometimes, mental health-care professionals are forced to employ coercion as a part of the treatment. The participants expressed that the way they employ coercion is crucial for balancing power and responsibility when facilitating SDM to form safe care: The decisions are beyond the power of both the patient and myself. I must do my job while showing respect for her as a human being … We made it (administering medication by coercion) by taking time, and she decided who was to give her the medicine and how she should lie. I offered to hold her hand. She refused to talk to me. When it was over, I offered her a slice of bread with honey and a cup of tea, and she smiled at me (Kaia, Session 8).
Standing together as a team was deemed necessary to make it possible for the therapeutic milieu as a whole to balance power and responsibility to form safe care. The participants described that standing together as a team entails good teamwork, shared knowledge, familiarity with, and a supportive attitude toward the patient. They experienced that good teamwork implies that colleagues know and trust each other, feel safe when working together, cooperate and are honest with each other, are not afraid to express disagreement, and stand together on the decisions made. They described good teamwork as shaping the atmosphere in the therapeutic milieu and having an impact on patients’ impression of receiving safe care: If the team members are uncertain about each other, there is a lot of anxiety on the ward, but when they are well coordinated, it becomes calm (Janet, Session 4).
The participants experienced that a supportive attitude toward the patient is important for creating a culture of trust. In the words of one participant, 11 persons stood in the staff room and expected that the next shift would be difficult because of one patient, but I considered it differently and had to tell them because I didn’t think it was right. It took courage for me to say that we must encounter the patient with a better attitude (Janet, Session 5).
Discussion
SDM is supposed to facilitate patients achieving real involvement in a therapeutic milieu (Dierckx et al., 2013). This study reveals that practicing SDM when balancing between power and responsibility to form safe care is a continuous, dynamic, and arduous process that requires each mental health-care professionals to internalize their attributes, facilitate patient participation, and create a culture of trust in the therapeutic milieu. According to the literature, such balance requires ongoing reflection on and assessment of the patient’s resources, limitations, and need for assistance in order to give them the power and responsibility they are capable of managing during various phases of illness with various needs (Kontio et al., 2010). The patient’s functioning can change over time, thus to ensure safe care mental health-care professionals should always compensate for the power and responsibility that the patient is unable to maintain (Rise et al., 2014). Kontio et al. (2010) describe that achieving this balance is a challenge for mental health-care professionals in the therapeutic milieu, as it sometimes creates difficulty because of the question “who knows what is best for the patient?” In a literature review by Sutton, Eborall, and Martin (2015), it is reported that patients can become specialists in their own conditions and that they want to ensure the best outcome. This is an important basis for SDM. However, mental health-care professionals experience that patients are often unable to maintain good recovery conditions for themselves (Kontio et al., 2010; Solbjør et al., 2011). For instance, when a patient is determined to take their own life, mental health-care professionals are obliged to assume responsibility and use the necessary power to intervene and prevent them from committing suicide. When mental health-care professionals use power against the patient’s will, they must simultaneously bear professional responsibility for protecting them. As the patient recovers and is no longer in danger, the power and responsibility should be gradually transferred back to them (Rise et al., 2014).
Prerequisites for practicing SDM include mental health-care professionals who are able to recognize that different clinical situations require differing approaches, as well as acceptance of SDM as a core element of good practice (Elwyn & Fisher, 2014; Grim et al., 2016). The process of reflection in clinical supervision improves mental health-care professionals’ understanding of their relationship with their patients (Holm Wiebe et al., 2011), which is essential for achieving a balance between power and responsibility to form safe care.
Participation in a clinical supervision program focusing on SDM, as in this study, is a way to develop knowledge of practice and make implicit knowledge explicit (Neher, 2016). In line with Neher (2016), this study promotes learning by allowing the members of the group receiving clinical supervision to critically reflect on implicit assumptions about themselves, the patient and others, as well as thoughts, motives, and behavior patterns associated with their experiences of SDM. Automatic and habitual actions can be transformed into more conscious and targeted ones (Neher, 2016). In this way, clinical supervision can help mental health-care professionals to make use of their professional skills and be attentive to the patient.
As described in this study, mental health-care professionals experience that facilitating patient participation is important as many patients either do not want or are unable to participate in their recovery process. Rise et al. (2014) state that patients need flexible services in order to regulate to their changing needs. When the patients have strong symptoms, they have a need to be taken care of and less responsibility, and when they have less symptoms, the need for empowerment, active participation, and more responsibility in decision-making is increased. Making it possible for patients to be listened to and have their views considered meaningful and acted upon in differing phases of illness requires active intervention (Sutton et al., 2015). By participating in clinical supervision, mental health-care professionals will gain a space where they can reflect on their practice, their experiences, and how they can develop better interactions with patients in different situations and with differing levels of engagement (Brunero & Lamont, 2012). The awareness and knowledge gained by reflection should enable mental health-care professionals to increase their capacity to apply the principles of SDM (Charles et al., 1997). By acknowledging the patients’ process of participation, mental health-care professionals show that they care about what is needed to help and that patient participation is important throughout the recovery process. Confirming that patients are important in their own recovery process should provide them with an impression of being autonomous and equal, conveying respect and dignity, which is essential in the balance between power and responsibility (Florin, 2007; Solbjør et al., 2011). When mental health-care professionals are aware of stimulating their patients’ involvement and acknowledging their patients’ process of participation, they are more likely to involve their patients in care by asking for feedback on treatment, encouraging them to speak up about risks, and plan for new interventions (Sutton et al., 2015).
Creating a culture of trust as outlined in this study is necessary in order to enable the therapeutic milieu as a whole to balance between power and responsibility to form safe care. “The way we do things here” is based on the mental health-care professionals’ norms, attitudes, beliefs, and values. As the culture is local, the work of creating a culture of trust should occur at unit level (Pronovost et al., 2009). Gathering mental health-care professionals who work together in the therapeutic milieu for clinical supervision provides them with a forum where they can share individual knowledge related to experiences of patient dialogue. A creative dialogue within the team enables mental health-care professionals to actively reflect on their experiences, attitudes, and alternatives for action. This learning process may promote collective SDM practice in the therapeutic milieu (Swart & Pye, 2002), and is also important for applying guidelines in a person-centered way (Elwyn & Fisher, 2014). The learning process may promote collective understanding and shared attitudes, which are important for standing together as a team.
Limitations
A limitation of this study is that the data were collected from dialogues in only one clinical supervision group. However, a strength is that the group took part in 10 meetings over a period of 4 months, thus providing insight into various aspects of the participants’ experiences (Polit & Beck, 2010). As the analysis and data interpretation process were influenced by the authors’ preunderstandings, the findings are therefore not objective facts but a reconstruction of the participants’ experiences, perceptions of reality, and understandings (Polit & Beck, 2010).
Implications for Practice
Ensuring SDM in a therapeutic milieu concerns balancing between power and responsibility. This is a complex and arduous process that does not take place by itself. Clinical supervision is necessary for enabling reflection on and promoting the practice of SDM in a therapeutic milieu. There is need for more research focusing on the patient perspective related to patients’ role in SDM.
Summary
SDM in a therapeutic milieu is supposed to facilitate patients achieving real involvement in a therapeutic milieu, in which concerns mental health-care professionals balancing between power and responsibility to form safe care. The clinical supervision program presented here is considered a useful tool in the effort to implement SDM practice in a therapeutic milieu. The findings revealed that clinical supervision facilitates the mental health-care professionals in the process of internalizing their attributes, stimulates them to promote patient participation, and serves as a forum for creating a culture of trust, which may enhance patient safety in the therapeutic milieu (Brunero & Stein-Parbury, 2008).
Footnotes
Acknowledgments
The authors wish to thank the participants for sharing their experiences and providing material for this study as well as the reference group (a former patient, a Head Nurse, and a psychotherapist) for contributing feedback on the study thus ensuring high quality.
Author Contributions
The study and the clinical supervision program were designed by L. B., K. R., and E. S. L. B. coordinated the research. L. B. and K. R. participated in the data collection: K. R. as clinical supervisor and LB as facilitator and moderator. L. B. analyzed the first two steps of the data interpretation, while L. B., K. R., E. S., and B. S. H. participated in the third step. The report was written by L. B. with supervision from K. R., E. S., and B. S. H. All authors provided feedback on the draft manuscript and approved the final version. They all adhered to the criteria pertaining to roles and responsibilities in the research process recommended by the ICMJE (![]() ).
).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is financed by Stavanger University Hospital. The review of the English language by Monique Federsel was funded by the Centre for Women’s, Family, & Child Health at the University College of Southeast Norway.