
Abstract
Recruiting and retaining nurses in mental health practice settings have long been problematic: A situation which is not helped by student nurses being exposed to negative attitudes about mental health nursing or poor clinical experiences. A pilot program in which student nurses were mentored on the mental health clinical placement was initiated at an Australian School of Nursing. A qualitative study was undertaken to explore the value of this program for the student mentee and the registered nurse mentor. A questionnaire containing six questions was distributed to all participants before and after the clinical experience. The questions were open format seeking data on (a) the perceived advantages or disadvantages of mentoring, (b) perceptions of whether mentoring contributes to professional development, and (c) whether mentoring contributes personally to the participant. The data were subjected to inductive thematic analysis. The registered nurse mentors found that time diverted from clients was a barrier to mentoring students; however, they experienced reciprocity through nurturance of self, students, and the profession. The student mentees found that they experienced a richer and deeper learning environment. Mentoring provides a satisfying learning environment for both parties if carefully implemented and supported.
Introduction
The acute shortage of mental health nurses in Australia has been described as a crisis (Harrison, Hauck, & Hoffman, 2014): one which is likely to worsen with the ageing of the mental health workforce (Australian Institute of Health and Welfare, 2013; Health Workforce Australia, 2012; Nadler-Moodie & Loucks, 2011; Stevens, Browne, & Graham, 2013). According to the Australian Institute of Health Welfare (AIHW) (2013), 88.3% of the mental health nursing workforce are more than the age of 45 years. Therefore, it is likely a large proportion of this workforce will retire within the next 10 to 15 years. Recruiting and retaining nurses in this specialty are clearly key to ameliorating any potential workforce shortages. However, this has been described as problematic (Happell, 2008; Hungerford & Hodgson, 2013; McCloughen & O’Brien, 2005), with evidence that nursing students are less likely to choose mental health nursing as a career option after graduation (Happell & Gaskin, 2012; Happell & Gough, 2009; Nadler-Moodie & Loucks, 2011; Stevens et al., 2013).
A vital component of preparing students for the role of a registered nurse (RN) is experience in real-world practice settings (Henderson, Cooke, Creedy, & Walker, 2012; Jonsén, Melender, & Hilli, 2013). It has been reported that how the student is received by the other staff in the practice setting strongly influences their learning (Levett-Jones, Lathlean, Higgins, & McMillan, 2009). Yet, numerous authors have described both the negative reception many students receive from the nursing staff during their clinical placements, and the poor quality of the clinical experience (e.g., Cambers, 2010; Jonsén et al., 2013; Tee, Özçetin, & Russell-Westhead, 2016). There is “no single, best way” to undertake student education in clinical practice (Maplethorpe, Dixon, & Rush, 2014, p. 183). However, a model which has received increased focus in the nursing literature is that of mentoring. It has been suggested that this can be a valuable recruitment and retention strategy in mental health nursing (Hazelton, Rossiter, Sinclair & Morrall, 2011; McCloughen & O’Brien, 2005). For students on clinical placement, a mentor can also be an important influence on their experience (McInnes, Peters, Hardy, & Halcomb, 2015) and may positively influence their choice of mental health nursing following graduation.
A pilot student mentorship project in the mental setting was initiated by the School of Nursing at one Australian university to investigate whether this enhanced the student experience and views of mental health nursing as a career option. The article which follows describes the experiences of both the students (mentees) and RNs (mentors) who participated.
Background
It is arguable that mental health is the most challenging area with respect to the recruitment and retention of nurses. Factors commonly cited to explain the loss of mental health nurses are as follows: workloads, workplace violence and aggression, stress, burnout, and reduced ability to cope with work-related stressors (Happell, 2008; McCloughen & O’Brien, 2005). In addition, Hungerford and Hodgson (2013) note the impact of a lack of role clarity, limited professional development, and more germane to this study, undergraduate students having poor experiences while on clinical placement—including a lack of mentoring.
These workplace issues are compounded by the deep seated and pervasive stigma attached to both having mental ill health and to being a mental health nurse. There is little written about the stigma associated with being a mental health nurse; however, a term that has been presented in the literature is courtesy stigma. This is also known as “stigma by association”; public disapproval evoked as a consequence of associating with a stigmatized individual or group (Halter, 2002, 2008; Larson & Lane, 2006; Verhaeghe & Bracke, 2012). Redknap, Twigg, Rock, and Towell (2015) term this as “secondary stigma” and suggest this is a disadvantage in the competition for nursing workforce (p. 273). In addition, nursing students are often encouraged to choose medical-surgical nursing rather than mental health nursing following graduation premised on the belief that this will consolidate their practice (Nadler-Moodie & Loucks, 2011). As Stevens et al. (2013) note “the care of people with mental illness is considered routine and mundane in comparison with the excitement involved in the manipulation of technology in surgical and critical areas of practice” (p. 213). Anecdotally, the authors have heard comments by other nonmental health nurses and nurse educators such as “you are not a real nurse” or “you will lose your skills working in mental health.” Students considering mental health as a career report that they often hear such comments.
Supportive relationships are the key to establishing supportive working environments where people want to stay (Mills, Francis, & Bonner 2005). As already noted, mentoring has been identified as potentially a valuable recruitment and retention strategy in mental health nursing (Grindel & Hagerstrom, 2009; Hazelton et al., 2011; McCloughen & O’Brien, 2005). A mentoring model of practice education can create a positive learning environment, and according to Siu and Sivan (2011), this has benefits for both mentor and mentee. These benefits include personal and professional learning, skill development, confidence, enhanced self-esteem, attainment of professional goals, and preparation for leadership roles. For students on clinical placement being supported through inclusion in the nursing team and being valued as a person impact on the ability to learn (Bradbury-Jones, Sambrook, & Irvine, 2011). When students feel supported and welcomed as team members, they focus on the learning: the development of knowledge, skills, competence, and confidence—rather than being preoccupied with interpersonal relationships (Bradbury-Jones et al., 2011; Levett-Jones et al., 2009). Thus, the student is less focused on endeavoring to understand and fit into the culture of the clinical placement and be accepted by the nursing staff. In addition, in the mental health placement, this interpersonal focus can include dealing with “the misconceptions and stereotypes they frequently hold towards people with mental illness” (Happell, 2015, p. 214).
An Australian study conducted by O’Brien, Buxton, and Gillies (2008) investigated mentoring of student nurses in the mental health setting. In this project, RNs worked with students in their area of specialty. This provided the students with increased familiarity with all aspects of the work environment, and subsequently there was an increase in applications for employment in those facilities involved in the study.
Roles of Clinical Mentor and Academic Mentor.

RN = registered nurse.
As shown in Table 1, the mentor and mentee were provided with preclinical placement education on the mentoring process and their respective roles by the academic mentor, and during the clinical placement, each student had 1 h of individual time each week with the academic mentor to guide the connecting of the theoretical teaching with the clinical learning. The students were able to discuss the new learning and to debrief the less straightforward and difficult learning experiences. What makes this model different from the usual model of student placement used by the university is the intensive input from the experienced clinical mentor as well as the academic mentor.
Methods
Research Design
The study was undertaken in a large, specialist mental health drug and alcohol community center which provides both inpatient and outpatient mental health services to a section of the population in a large Australian city. The chosen study design was qualitative descriptive. It is a research approach which Sandelowski (2000) describes as particularly suited to obtaining “answers to questions of special relevance to practitioners and policy makers” (p. 337) as can provide access to people’s thoughts, feelings, and attitudes to a situation in a manner which is relatively free from theorizing. In this study, the participants were asked to complete in writing a questionnaire containing six open format questions which was distributed before and after the clinical experience.
Research Questions
Research Questions.
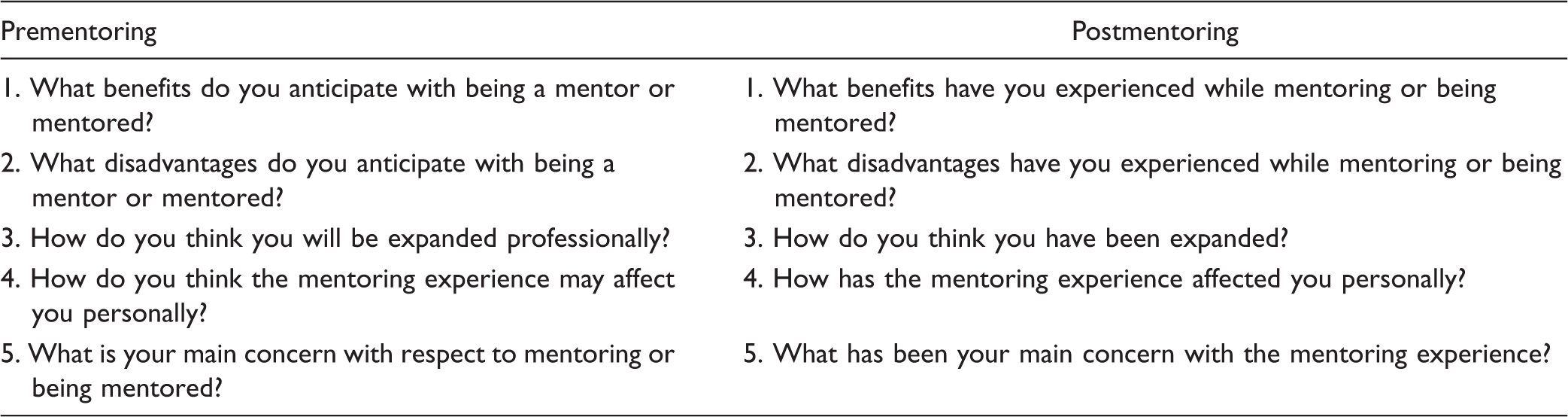
Space was provided for the participants to write their responses, and in addition to the five questions, there was a space for the participants to write further comment as they thought appropriate to the experience.
Participants
RN Mentors.

As shown in Table 3, the majority of the mentors had considerable nursing experience postregistration. All had previously worked as clinical buddies with students on clinical placements. There is an expectation during rotations that all RNs undertake a buddy where they provide clinical support and teaching to the student. However, this is an ad hoc process, and depends on the willingness of the rostered staff to accept the assignment, which is only for that particular clinical shift. Therefore, students may be assigned to a number of different buddies depending on who is available (and willing) on any particular day. The mentor, on the other hand, works alongside the student in a sustained manner for the duration of the placement. The mentor role is a deeper relationship as it also includes a focus on the student’s short- and long-term professional goals. It is entirely voluntary and there is no expectation, at this point, that this is a requirement of the RN’s professional role. Four of the RN mentors chose not to participate in the study. Although they had been assured that only the administrator would have knowledge of identities, it is possible that they were concerned with respect to issues of anonymity and confidentiality; however, several told the administrator that it was because they chose not to use their personal time in responding to the questionnaires.
Ethics
The study was approved by the hospital’s Human Research Ethics Committee and the University Human Research Ethics Committee. An information sheet and consent form was sent to all the potential participants via e-mail. The participants were assured that their confidentiality would be protected and no information linked to a particular person would be included in any subsequent publication or presentation. The participants were also informed that they had the right to withdraw up until the time of completed data analysis and that nonparticipation would have no impact on either their course of study, employment or relationship with the university, and any of its representatives.
Analysis
The hand-written comments were transcribed into electronic format by one of the researchers. Inductive content analysis was then applied to extract categories and themes to describe the phenomenon. The data were first analyzed by one of the researchers and subsequently subject to a further cycle of analysis and verification with the other author. This iterative process continued until consensus was reached. The initial phase was the close reading and rereading of the transcripts, and those parts of the transcripts that provided understanding of the participants experiences were highlighted and noted as self-explanatory descriptive codes (King & Horrocks, 2010). The descriptive codes that shared some common meaning were then grouped for interpretive analysis of meaning. Finally, the overarching themes were elicited.
Findings
The analysis of both datasets—the pre- and postclinical questionnaires of both the mentors and the mentees’ responses—revealed two overarching themes and associated subthemes. These were as follows: (a) barriers with the subthemes of time constraints and relational concerns and (b) nurturance with its subtheme of deeper and richer learning.
Barriers
Both pre- and postmentoring experience the factor that was most frequently identified as presenting a barrier to engagement in mentoring or being mentored was that of lack of time.
Time constraints
Before commencing the mentoring relationship, several of the RNs expressed concern that it would be time consuming; a concern echoed by a number of the students. Whereas the students were concerned about whether they would have enough time with their mentors, the RNs were concerned about the time the mentoring might divert from their clients. One expressed disquiet about “attention being diverted to students,” and this time issue was evidently associated with a perceived tension between meeting both client and mentee needs. In addition, given the nature of the clientele, it was perceived that there might be “difficulty establishing a trusting environment with patients when being accompanied by a student.”
These concerns were found to be valid as evidenced by the comments provided postmentoring experience. One RN noted that “allocating time to the student meant less time for my work … unable to see more difficult, inappropriate clients.” For some—both mentor and mentee—the issue was not about being diverted from the clients’ needs per se but about the time requirements on top of the current workload allocation. For one RN when “very busy on intake, I would have liked to have been able to spend more time going through the processes.” For some students, there was both the time constraints and the needs of other students who were not part of the pilot mentoring program: Having a mentor who has many students to attend to aside from myself, meant I didn’t always get to communicate with my mentor as frequently as I would have like because their time is being taken up by other students.
Relational concerns
This theme was more frequently identified in the prementoring responses; however, it was identified by several of the participants in the postmentoring questionnaire as well.
Prior to the mentoring experience, several of the RNs were concerned that either the student would not engage as they would expect, there might be personality conflict or else of “not meeting all the student’s expectations.” Similarly, the students were concerned about not meeting the RN’s expectations, having a mentor with whom they clashed or who provided a poor role model. For example, one student commented, “my only concerns are picking up bad habits from my mentor, and letting my mentor down if I do not perform so well.” Another expressed concern, also, about poor role modeling if “the mentor had other motives such as self-importance or control issues.”
Nurturance
The pre- and postmentoring responses reveal that the majority of RN mentors and student mentees were anticipating a rewarding experience that can be conceptualized as nurturance. The responses postmentoring provide evidence that this anticipation was experienced as feeling of nurturing and being nurtured.
From the students’ perspective, it was a relatively simple expectation of, and resultant experience of, being nurtured through the provision of support, reassurance, knowledge giving, and guidance. As noted in one student’s response prementoring, “a mentor provides support and reassurance when adapting to new situations.” While postmentoring, according to one, such reassurance was provided: “A lot of anxiety about my clinical placement this semester was a fear of the unknown, and the mentor was able to ally most these fears because they were there to help when needed.”
While the support in orienting to a new environment was clearly highly valued, so too was the opportunity for increasing their knowledge and clinical skills. For example: I think a mentor will be of a great help when opportunities arise because they may be able to provide extra information about such an opportunity through their own experience. They may be able to guide you through the pros and cons of a situation, so that you are able to make an informed decision. One-on-one individual time with the mentor has meant better quality training and practice of skills, and individual assessment of my skills and areas for improvement. There is also the added benefit of time with the mentor to ask questions and gain more information from an experienced person.
Deeper and richer learning
A salient theme in the student responses following their clinical placement and working with a mentor was that this was a “deeper and richer” learning experience. I loved being mentored in community mental health – the staff were fantastic in teaching and setting up opportunities for me within their unit and so I could gain a good understanding of their individual roles and the role of the community mental health team. Having a mentor gave an infinite number of greater opportunities. As students there are so many skills/opportunities that we are not even aware exist. It is not until someone else points it out that we realise we didn’t know anything about it. Having a mentor to point out these things greatly helped me in being able to find learning opportunities and use them to their full advantage. I found myself being challenged to think critically in many situations, particularly on my assessment of a client and they might be acting the way they were, e.g., because of drugs, alcohol or an illness such as schizophrenia.
Discussion
The major limitation in this study is the small number of participants. Most of the student mentees who were part of this clinical experience participated; however, only 7 of the 11 RN mentors were willing to undertake the questionnaire, citing time pressures as a reason for not participating. It was shown in Table 3 that two of the mentors had Master’s degrees, and that six had more than 8 years clinical experience. However, the study did not investigate the extent to which academic preparation or length of experience contributed to the mentoring experience. Although this study is limited in scope, it contributes to the emerging body of knowledge in revealing that a mentoring relationship can provide a reciprocal relationship between students and RNs, which creates a deeper and richer learning environment.
Beyond the creation of a more potent learning environment, the findings reveal that the experience also allayed perceived barriers such as anxiety and fear about undertaking the mental health clinical placement. A fear that is often founded in the many misconceptions about mental illness, and mental health nursing; negative attitudes toward people with mental ill-health are found among nurses, and other health-care personnel that are not dissimilar to those of the general population (Dearing & Steadman, 2008). The experience of working with people who were struggling with their mental well-being was not only contextualized in relation to classroom teaching but also facilitated personal understanding; during debriefing sessions comments such as “they are real people” and “they are just like us” were commonly heard.
It was noted in the findings that there was an increase in reflection and critical thinking. The students were able to recognize the importance of the use of self in the therapeutic relationship. Rather than seeing mental health as an area in which they will lose their skills they were able to perceive it as one in which a different skill set is utilized. One student participant noted that “nurses in the general setting use a lot of technology to help perform their jobs, mental health nurses use themselves as a tool. It’s the way they interact with the patient that measures and heals.”
The increased time spent on reflection with both their academic and clinical mentors enabled deeper and richer learning through discussion about clinical work, themselves, their colleagues, and the influence of their own personal value judgments. The reciprocity between student mentee and RN mentor identified in this study has been found elsewhere; for example, Penman, Papoulis, and Cronin (2013) found that a partnership approach between student and mental health clinicians is “mutually beneficial.” Thus, it is important that the clinical learning environment is one in which both parties gain satisfaction from the learning relationship.
Implications for Nursing Education and Practice
This study highlights the value of the mentoring experience for both the student and the RN. Rather than the students being perceived as an additional workload burden, the RNs enjoyed sharing their knowledge at a deeper level, and perhaps more importantly valued being able to promote mental health nursing. The students experienced a richer learning environment where they were enabled to reflect more positively on mental health nursing as a potential career choice. While this is only a small study at one site, the findings suggest that such a model could provide a useful strategy to address both recruitment and retention. An environment can be created that welcomes and supports the needs of the student learner, and facilitates deeper engagement while simultaneously enhancing the satisfaction of the RN with their role.
While this is one potentially useful strategy to a multifaceted problem, it needs careful implementation, and adequate resourcing, to ensure that the RN mentors are not compromised by the needs of the students versus those of their clients.
As noted earlier, O’Brien et al. (2008) found that improving the undergraduate mental health clinical placement experience resulted in increased applications for new graduate positions in the participating facilities. Therefore, it is possible that the mentoring of nursing students during their mental health clinical placements might have a similar result and be helpful as part of a bundle of strategies aimed at addressing recruitment issues. However, any such intervention might well prove futile if ongoing issues in mental health clinical practice environments have not been addressed. The participants in a mentorship program for new graduates working an Australian public mental health service characterize the environment as tough with a focus on security rather than therapy, staffed by veteran colleagues, of whom many were dismissive of them, and provided poor role models both therapeutically and collegially (Hazelton et al., 2011). Equally, as an undergraduate mentoring program requires thoughtful planning and resourcing so to this needs to be built upon when the new graduates enter the mental health workforce. As noted by Hazelton et al. (2011): … new graduate nurses potentially represent a powerful force with which to oppose the regressive mindsets and practices of many veteran staff in mental health services. It is critical that they are provided with the support necessary to consolidate the lessons from university once they join the work force, including strategies for modelling the work of progressive colleagues and managing exposure to recalcitrant staff. (p. 183)
Summary
Mental health nursing is facing a staffing crisis in terms of retention and recruitment of nurses. New strategies are required to ensure that the practice environment is one that welcomes students and opens them to the rich possibilities of a career in mental health. Simultaneously, any strategy for supporting student nurses on their mental health clinical experience needs to be rewarding for the RNs involved so that working alongside a student is professionally and personally satisfying rather than an additional and unwelcome burden. The findings from this study demonstrate the value of mentoring as a clinical learning model for both parties. It creates a mutually rewarding richer and deeper learning environment and has potential to be a successful strategy in the growth of the mental health nursing workforce.
Footnotes
Acknowledgments
The authors would like to thank Mrs. Gail Burgess for her administrative support and are also grateful to the students and registered nurses who agreed to participate, and to all those without whom this pilot mentoring project would not have been possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.