
Abstract
Systems navigation services provided by a designated provider or team have the potential to address health and social disparities. We conducted an environmental scan of navigation activities in a large urban Canadian community to identify and describe: service providers who engage in systems navigation; the clients who require systems navigation support and the issues they face; activities involved; and barriers and facilitators in providing systems navigation support to clients. Using an online survey and convenience sampling, we recruited individuals who self-identified as community navigators or practiced systems navigation activities as part of their role. The majority of respondents (n = 145) were social workers, social services workers, or nurses. Clients of navigators struggled with mental health or addictions issues, disabilities, chronic diseases, and history of trauma or abuse. The most frequently reported activities of navigators were building professional relationships, managing paperwork, and communicating with relevant agencies or organizations. Barriers to navigation were time available in the work day, difficulty partnering due to bureaucratic structures, differing philosophies and ways of working, and a lack of central information repository in the community. Facilitators were a client-centered organization, the availability of multiple community resources in the region, and organizational support. Participants struggled with client waitlists, system issues such as lack of resources and interagency collaboration, and role clarity.
Keywords
Introduction
In Canada, it is estimated that over 15% of the population lives with multiple chronic diseases (Chronic disease and injury indicator framework, 2015). Clients and families with complex and chronic conditions struggle to navigate health and social systems, and providers are expected to support their clients in this struggle. Fragmentation of the health care system has been recognized as problematic within Canada, with an influential national report suggesting that individuals are left on their own to negotiate networks of programs and providers to get the information and full range of services needed (Romanow, 2002). A more recent report noted that patients and their family caregivers need greater integration among different health care providers and settings (Expert Group on Home and Community Care, 2015).
Systems navigation, through the use of a designated professional navigator or a team providing navigation services, has emerged as a potential intervention to address health and social disparities resulting from fragmentation and inequitable access to services (Natale-Pereira, Enard, Nevarez, & Jones, 2011). Broadly, navigation is a person-centered approach to empower individuals and families to identify needs or concerns and establish a connection with appropriate services (Freeman & Rodriguez, 2011). Navigators address health, and often social systems, to coordinate care and facilitate access along the continuum of care (CARNA, 2008; Doll et al., 2003; Freeman & Rodriguez, 2011; Manderson, McMurray, Piraino, & Stolee, 2012).
Social determinants of health are key determinants of health equity. The conditions within which people live their everyday lives are influenced by structural drivers such as gender, race, class, economics, power relations, and government policies (Marmot, Allen, Bell, Bloomer, & Goldblatt, 2012). Those who are disadvantaged by these factors also often have difficulty accessing material resources to maintain and improve their health status. In addition, the concept of social capital is recognized as a significant determinant of health (Macinko & Starfield, 2001). Bourdieu's dimensions of capital or “habitus” include economic, cultural, and social capital. He defines social capital as “the aggregate of the actual or potential resources which are linked to possession of a durable network of more or less institutionalized relationships of mutual acquaintance or recognition” (Bourdieu, 1985, p. 248). Bourdieu refers not only to the social relationship itself that allows people to get resources possessed by his or her associates but also to the quality of these resources (Lesser, 2000). Bourdieu (1986) also refers to “doxa” (a set of unquestioned rules, discourses or common assumptions and understandings) that exist within a “field” (an area or structured social patterned activity or practice with internal protocols and assumptions, e.g., the healthcare field or social care field). With respect to systems navigation, the navigator must help their client understand these “fields,” each with its own “doxa,” in order to enable their clients to access and benefit from these services. As such navigators have an important linking role to play.
Putnam (2000) expands on Bourdieu by distinguishing between “bonding” capital (the strongest ties between members of an exclusive, homogenous group) and “linking” social capital (making connections between institutions and individuals with power to leverage resources; Woolcock, 2001). Systems navigation can be understood as an intervention to increase social capital for both individuals and communities. Navigators are a form of “bridging” social capital (vs. “bonding” or “linking” social capital), and this form of social capital has been related to health (Ehsan & De Silva, 2015; Habibov & Weaver, 2014; Szreter & Woolcock, 2003). “Bridging” refers to weaker ties that are made across diverse social circles to help members link to external resources (Putnam, 2000). Systems navigators establish relationships of trust with others, to facilitate access to services and resources for those who need them, and as such act as bridges across social networks, and to access resources (bridging). They may also contribute to “linking” social capital as they work at the broader community level with other institutions. Navigators work through institutions and their attendant social and power relations to link individuals to health and social services.
In primary and community care, navigation services are delivered by health care professionals or lay providers. Navigators assist with fragmentation of health and social health care system through various methods, including communication with multiple agencies (Bishop, Edwards, & Nadkarni, 2009; Clark et al., 2009; Gimpel et al., 2010; Hendren et al., 2011), facilitating access to care (Bishop et al., 2009; Brown et al., 2011; Clark et al., 2009), navigating the system and services (Bradford, Coleman, & Cunningham, 2007; Brown et al., 2011; Palinkas, Ell, Hansen, Cabassa, & Wells, 2011), or assisting individuals with health insurance. Often navigators work with specific populations. For example, McCloskey (2009) describes the role of promotoras. These are community members who act as navigators to reduce health disparities among Hispanics in a diabetes intervention program in New Mexico (McCloskey, 2009). The work of promotoras include enrolling patients in diabetes and exercise programs, meeting with them individually for support, educating clients about smoking cessation, and leading grocery store tours.
Navigators address both health and social issues. For instance, there are many nurse-led navigation models developed for patient populations with complex needs such as patients with multiple chronic conditions (Boult & Wieland, 2010; Boyd et al., 2007; Foret Giddens, Tanner, Frey, Reider, & Boult, 2009; Maeng, Davis, Tomcavage, Graf, & Procopio, 2013; Williams, Smith, Chapman, & Oliver, 2011; Wolff et al., 2009), immunodeficiency diseases (Burton, Murphy, & Riley, 2010; Pfeffer & Schnack, 1995) or young adults with schizophrenia (McCann & Clark, 2005). The Guided Care Model is a nurse-led interdisciplinary model of primary care designed to improve the quality of life and resource use for medically complex older patients (Boult & Wieland, 2010; Boyd et al., 2007; Foret Giddens et al., 2009; Wolff et al., 2009). The care delivered by these navigators in the Guided Care Model includes: home assessment of the client and caregiver, encouraging self-management, coordinating providers of care, smoothing patient transitions by communication with hospitals and emergency departments, and educating and supporting caregivers (Foret Giddens et al., 2009). Navigators also address social issues including housing concerns (Clark et al., 2009; McCloskey, 2009; Retkin, Antoniadis, Pepitone, & Duval, 2013), food insecurity (Boyd et al., 2007; Clark et al., 2009; Kramer, Nosbusch, & Rice, 2012), legal issues (Kramer et al., 2012; Retkin et al., 2013), employment issues (Linkins et al., 2011; Retkin et al., 2013), financial difficulties (Hendren et al., 2011; Kramer et al., 2012), racism (Kramer et al., 2012), and lack of social support (Hendren et al., 2011).
Effective navigation services can lead to improved health outcomes for patients including better overall health and wellness (Bohman et al., 2011; Bradford et al., 2007; Esperat et al., 2012; Kramer et al., 2012; Linkins et al., 2011; McCloskey, 2009; Natale-Pereira et al., 2011; Retkin et al., 2013; Spiro, Oo, Marable, & Collins, 2012); reported self-efficacy, self-management, and empowerment (Burton et al., 2010; Esperat et al., 2012; Foret Giddens et al., 2009; Gimpel et al., 2010; McCann & Clark, 2005; McCloskey, 2009; Natale-Pereira et al., 2011); better access to care (Bohman et al., 2011; Ferrante, Cohen, & Crosson, 2010; Layne, Rose, Longnecker, & Holmes, 2012; Natale-Pereira et al., 2011; Tataw, Bazargan-Hejazi, & James, 2011); and better follow-up to care (Batra et al., 2009; Layne et al., 2012). Navigation services have also resulted in less use of acute care services for care that could be provided in the primary care setting (Esperat et al., 2012; Layne et al., 2012; Maeng et al., 2012; Mayhew, 2009).
Navigation is a patient-specific health care delivery model intended to reduce barriers and facilitate access to care by providing professional or lay support through the continuum of care (Thoms & Moore, 2012). To enhance navigation services in communities, there is a need to understand who is providing navigation support, what providers are doing to reduce barriers to access to health and social services, and challenges they face working with multiple patient populations. In 2014, as part of a community-research collaboration, the local public health department in Hamilton Wentworth funded a pilot project to organize a “community of practice” for health and social services navigators, and conduct an environmental scan of navigation activities in the community. The objectives of this descriptive study were to (a) identify and describe the providers of systems navigation within community settings; (b) describe the clients who require systems navigation support and the issues they face; (c) identify activities involved in providing systems navigation support; and (d) identify barriers and facilitators to providing systems navigation to clients. With the rapid emergence of new navigation roles and programs in primary and community care, the results of this study can inform the development and maintenance of navigation roles and services in a community.
Methods
For this descriptive study, we developed and administered an online questionnaire to understand health and social system navigation in the community by exploring the topics identified in the aforementioned objectives. The study was approved by the Hamilton Integrated Research Ethics Board.
Survey Instrument and Administration
The initial content for the questionnaire was informed by results of a scoping review of literature on systems navigation and navigator roles in primary health care conducted by the research team. The questionnaire was pretested for face and content validity with approximately 10 individuals who attended a local Navigation Community of Practice (N-COP) meeting. Providers from health and social services organizations were represented since the scoping review which was focused on primary care activities that might not capture activities conducted in other sectors or organizations. We integrated feedback regarding clarity of language used and comprehensiveness of survey items. The revised questionnaire was subsequently pretested with a community nurse navigator and a primary care navigator with a social work background to further establish validity. Content validity was assessed in the following ways: (a) use of data from a scoping review of the literature on navigation, (b) review of drafts by researchers with content expertise and N-COP participants, and (c) comments about comprehensiveness from two providers who pretested the questionnaire. Feedback from these activities was incorporated into the final version of the instrument. The instrument was then converted into electronic format using LimeSurvey.
The final questionnaire incorporated a definition of systems navigation which was as follows: assisting individuals and families to navigate through complex systems and access appropriate health, specialty and social services can work to ensure the most effective use of health and community services with the intention to enhance one's well-being or support care delivery. Navigation is a client-centered approach to empower individuals and families to identify needs or concerns and establish a connection with appropriate services.
The survey contained 5 open-ended and 12 forced-choice items. Open-ended questions were related to work title, length of time doing systems navigation, the biggest challenges in providing navigation, and strategies to improve navigation in Hamilton. Forced choice questions were related to participant demographics, navigation-related work activities and roles, client descriptors and issues, and barriers and facilitators to providing navigation. The questionnaire took approximately 10 to 15 minutes to complete.
Sample
We used convenience sampling to recruit individuals who self-identified as community navigators or practiced systems navigation activities as part of their role. This broad criterion facilitated the identification of as many navigators or service providers providing systems navigation as possible given the variation in job titles and roles in the community. Members of the N-COP (n = 41) were the first group invited to participate in the study through an e-mail invitation. Subsequently, we applied a snowball technique to recruit others. An electronic link to the online questionnaire was included in N-COP meeting minutes with instruction to distribute the link freely. A description of the survey and invitation to participate was also sent to primary care community organizations including primary care practices and community health centers. All surveys were anonymous and participant consent was implied through completion of the survey. The LimeSurvey database, account, and results were maintained by a research coordinator and principal investigator.
Analysis
Data were analyzed using descriptive statistics. Means and frequencies were calculated to summarize demographic data and responses to questions. Chi-square tests were used to compare differences between participants. For the qualitative data from open-ended questions, we used NVivo 10 software to organize and categorize responses.
The open-ended questions created a large volume of short statements. To analyze data, we utilized directed content analysis, where an existing theory or framework is used to identify initial coding categories (Hsieh & Shannon, 2005). We chose an ecological framework for health promotion (McLeroy, Bibeau, Steckler, & Glanz, 1988). In this model, behavior is viewed as being determined by the following: (a) intrapersonal factors; (b) interpersonal process and primary groups; (c) institutional factors; (d), community factors; and (e) public policy. A socioecological model is appropriate because “it moves beyond the cognitive determinants of individual actions to encompass the larger social, cultural, and economic contexts that influence health-related behaviour” (Ingram et al., 2016, p. 169). This framework has been utilized frequently to assist with qualitative data analysis in published studies in primary and community care. For instance, recently it was used to explore the barriers that primary care providers face with clients to maintain a healthy weight (Woodruff, Schauer, Addison, Gehlot, & Kegler, 2016). In another study, the framework was used to identify themes from interviews exploring sexual and reproductive health needs and priorities with Latinas who participated in a community-based participatory research (Mann et al., 2016). In our study, the framework was used to create categories for the data (for example, intrapersonal, interpersonal, institutional, or community factors) and deductively code into these categories. Within categories, we found common themes through inductive coding. The data analysis was conducted by the primary author and checked by members of the research team (RV and JF).
Results
Participant Characteristics
Description of Participants (N = 145).

Characteristics of Clients Receiving Navigation Services
Types of Clients Receiving Navigation Services.

Barriers that clients face to access health and social services
Client Barriers to Accessing Health and Social Services.

Providing Navigation Services to Clients
To establish a more comprehensive understanding of how respondents provided navigation support, we questioned the activities involved in navigation support, barriers, and facilitators of providing systems navigation, challenges they faced, and recommendations to improve systems navigation in their community.
Activities involved in navigation support
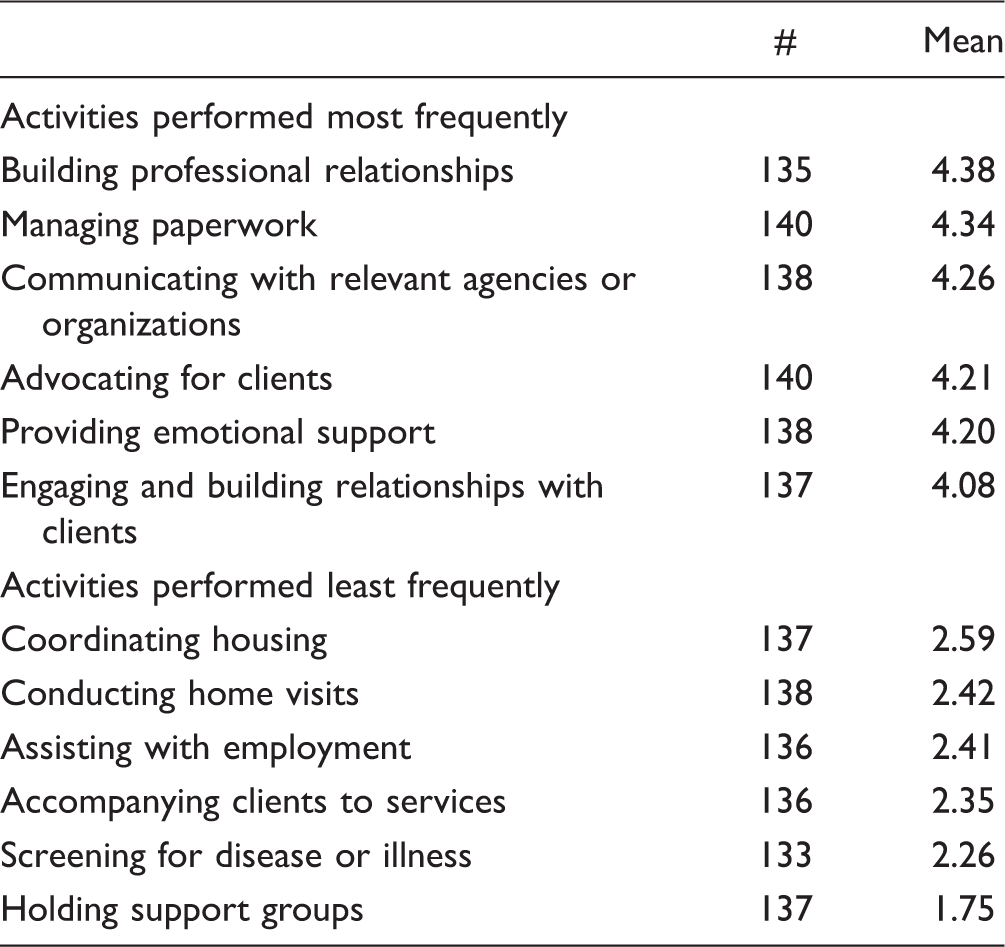
Most and Least Frequent Navigation Activities Performed by Respondents (N = 145).
Barrier and facilitators to providing navigation support
The barriers and facilitators reported were further categorized into intrapersonal factors (characteristics of the individual such as knowledge), interpersonal processes (formal and informal work and social support systems), institutional factors (social organizations with rule and regulations), community factors (relationships among organizations and institutions with defined boundaries), and public policy (local, provincial, or national policies) according to the ecological framework by McLeroy et al. (1988). Respondents responded to questions to providing navigation support to clients on an ordinal 4-point scale (including: 0 = not at all; 1 = minimally; 2 = somewhat; 3 = a great deal). The most frequently reported barriers include: time available in the work day (intrapersonal; µ = 2.98); difficulty partnering due to bureaucratic structures (institutional and community; µ = 2.96); differing philosophies and ways of working (institutional and community; µ = 2.87); a lack of central information repository or database for health services in the community (policy at local level; µ = 2.73); and policies that make it difficult to provide services or care (policies at the provincial system; µ = 2.73).
Respondents were also asked to select from a number of items to understand what facilitated their ability to provide navigation support. The most commonly reported responses were institutional factors including a client-centered organization (71.7% of respondents) and organizational support (56.6%) and a community factor—the availability of multiple resources in the region (69%).
Challenges to providing navigation services to clients
In an open-ended question, participants were asked to list three challenges in providing navigation support to their clients. The most commonly reported challenges were institutional and community factors (waitlists, systems issues, and lack of resources), interpersonal processes (role clarity issues), and intrapersonal issues (client resource issues).
Waitlists
Participants most frequently reported the challenges of lengthy waitlists for community agencies and programming, housing, residential or long-term care placements, and access to outpatient services, mental health programs, and specialized services such as psychiatry. One participant described the “wait times and administrative nightmares in gaining access to services.” Waitlists were challenging for both providers and clients. One respondent described the frustration resulting from a prolonged wait for service this way, “When the patient finally gets the service, it often doesn't offer them what they need.”
Community and public policy systems issues
The second most commonly reported challenges were systems issues. Many respondents highlighted the constant changes, including changes to government funding systems. A number of them described the problems of communication and one described the issue of “silos at provincial level, ministries, sectors, and within organizations.” Another respondent articulated the difficulty in working with providers from different services and said, “Our programming is outreach-based, focusing on hard-to-service clients. The biggest challenge is to engage other services (medical for instance) to meet clients where they are at in the community. Many policy and bureaucratic differences impact service.” Strict policies and regulations were seen as a challenge by many as this respondent said, “Program eligibility criteria and mandates are a barrier. For example, individuals in need of mental health support are often unable to access services until they have a formal diagnosis.” Another respondent described the problems clients can face once they enter the system through different points: “Supports and services are often tied to ‘systems’ and not individuals. Individuals therefore risk losing vital services and supports when they move from one program to another (for example when moving from employment service programs to disability support programs).” Additional system challenges to providing navigation included lack of collaboration between agencies and issues in sharing client information.
Resource issues
Resource challenges included lack of funding for services, programs, and provider positions to support navigation work as well as services for these populations in general. Respondents highlighted resource challenges for specific populations, such as the limited funding for mental health, or “limited and dwindling resources for population 16 – 59 years old (singles/couples without children).” A number of respondents reported that there were not enough systems navigators in their community and they could not keep up with the demand for service. In contrast, one respondent described the problem of too many navigators and how it was related to wait lists in this way, Currently there are so many people navigating, but there are issues with too many people referring to agencies for service, and those agencies not having the capacity to act due to lack of funding. Consequently wait lists for service increase and clients become distrustful and discouraged with lack of service.
Role clarity issues
With the rapid emergence of navigators and navigation services in the community, respondents reported the challenges associated with duplication of services related to role clarity. One participant described the consequences of unclear roles, I found the vast increase in system navigators when working in case management was quite ridiculous. There were no clear descriptions of what each navigator was capable of, and since every organization feels the need to have one and they don't coordinate between each other, it adds another layer of useless bureaucracy that wastes time and money that would be better diverted to health promotion initiatives so people could stay out of the healthcare system rather than need to be haphazardly guided through it. Role clarity is an issue. Public health nurses (PHN) used to perform the navigation role as part of their job description. That changed with funding model changes. However, many PHN's are still providing navigation services in their current role (e.g. school nurses, mental health nurses, chronic disease nurses) but it is not officially recognized because the public health mandate is population health.
Client resource issues
Providing navigation support was challenging because clients had resource issues such as low income, lack of adequate social assistance, medication coverage, and food security issues. Financial constraints prevented clients from accessing services. Specific examples of this included lack of funds for transportation or childcare, or loss of contact due to clients' inability to manage funds to keep phone service. One respondent described the resources implications of clients accessing care, “Clients are often left with a disjointed system that asks them to take time out of work, school or family life (which can be a substantial cost) while they navigate large systems that can feel very dehumanizing and degrading.” Another respondent said, “There are many services for the destitute, but not many available to prevent people from becoming destitute.”
Suggestions for Improving Navigation Services
Suggestions for improving navigation from open-ended questions were categorized and presented according to frequency of mention. They include: (a) strengthening interagency collaboration and partnership (e.g., communication and coordination), (b) enhancing support for navigators (e.g., information and education), (c) applying a client-based approach to navigation (e.g., client centeredness), and (d) a focus on needs-based supports for clients (e.g., better education for newcomers, services specific to ageing). Detailed descriptions of responses are provided later.
Interagency collaboration and partnership
A large proportion of the suggestions were related to work between agencies, including the need for improved collaboration, centralization and integration of services in the region, better communication, and more sharing of information. One respondent reported on the lack of trust and the need for shared vision between agencies, The most notable challenge is the lack of trust and communication between agencies. This often feels like it stems from differences of philosophy between agencies and the need to protect funding. We all need to have the trust and understanding that agencies and people are trying to serve their clients the best they can, and that collectively we are working together to serve people.
Support for navigators
Many respondents suggested resources were needed for more navigators and also for new roles in different areas of the system. One respondent said, “Develop roles in areas that follow patients in their journey in and out of hospital and that have the ability to deal with clients from diagnosis to cure or death.” Other suggestions for support included the creation of a community of practice, a database and flowchart of navigators and services, and training and mentoring that included best practices and care pathways. One respondent said this about the training needs of navigators, “Ensure those in navigation positions are trained to assess the client experience and have knowledge of the system and its limits. It is not simply a referral-based role.”
A client-centered approach to navigation
A number of respondents suggested an approach to navigation that is client-centered as this participant said, “We have bureaucratic filled social services that people are forced to access, yet are difficult to access and lack flexibility and adaptability, which is needed because we are working with people who are all a bit different.” Another respondent described the need to remain focused on clients this way, “I find myself curbing my inclination to fit clients into programs and services versus finding programs and services that are a good fit for clients.”
Needs-based supports for clients
A number of participants suggested programs specific to certain population groups. One participant said, “There are inadequate supports for the aging population. Programs, supports and institutions which address senior-related issues are not funded well.” A number of suggestions were related to clients who were newcomers to Canada and this person said, We need better education for newcomers when they arrive—knowledge about signing leases, where to go for their ethnic food, child care information i.e., don't let your child play outside unattended, how to look for a job. There are not enough system navigators who can speak other languages.
Discussion
Bryant, Raphael, Schrecker, and Labonte (2011) establish that there has been a weakening of Canada's capacity to address health inequalities over the last 25 years (Bryant et al., 2011). Reductions in public spending on families, old age, minimum wage, social assistance rates, and changes to tax structures means that Canada's public social expenditures are low compared with other Organisation for Economic Cooperation and Development countries. Bryant notes the significant shift in the mid-1990s where Canada's provinces transferred resources to health care and education from social services, with very little spending in the latter category. The result is increasing income inequality and poverty, and less than adequate public policies to address the social determinants of health across the population.
Canada is not alone in its concerns about rising income inequality and the recognition that this is directly related to population health, both nationally and internationally (Macinko & Starfield, 2001). It is also clear that the widening gap of income inequality within societies creates a “social gradient” that is deleterious to human health (Marmot et al., 2012; Wilkinson & Marmot, 2003). All of these factors create worsening conditions for vulnerable populations who are living with chronic illness. This presents challenges for those working in health care who care for individuals with health and complex social needs.
We report on the first Canadian study to explore multiple components of and influences on systems navigation including demographics of providers and clients, navigation activities, and barriers and facilitators to providing navigation support that links individuals to health and social services to meet their needs. The purpose of our descriptive study was not only to begin to understand systems navigation from the provider perspective but also to learn more about how services could be improved to meet the needs of clients in the community.
The survey respondents came from a variety of fields and were employed in health sectors, social services, police, emergency services, faith-based organizations, and education. The differences in the background of our respondents and the organizations in which they work are reflected in the navigation activities they performed most frequently: building professional relationships, managing paper work, and communicating with other agencies. It appears that this type of work is done just as frequently as the work they do with clients, such as relationship building and providing emotional support. The breadth and complexity of the employing organizations may account for the large number of comments we received about barriers, such as: sharing of information, bureaucratic structures, and differing philosophies. As well, there were frequent suggestions to improve interagency collaboration and partnership and to promote a client-based approach to navigation.
Lack of time available in the work day was the most frequently reported barrier for respondents. Just over half of our respondents reported that systems navigation was a secondary function of their role and our data suggest that there is a need for more resources or professional education to support respondents in this type of work. Despite such a breadth of providers and agencies involved in providing navigation support, new navigation roles have been introduced into the community. Our respondents reported role confusion and role overlap due to a lack of careful planning and a lack of shared vision. These results closely align with factors influencing collaboration between primary care and public health which showed that role clarity and having a shared vision and clear mandates between organizations are imperative for collaborative work (Martin-Misener R et al., 2012; Valaitis et al., 2012). Work in primary care and public health collaboration suggest that some of the strongest collaborations can occur when increasing access to care through outreach and care to vulnerable or marginalized populations (Valaitis et al., 2015). The need for careful planning of new health provider roles based on client needs is a recommended strategy to prevent role confusion and more successful implementation (Bryant-Lukosius & DiCenso, 2004). However, other recent literature in mental health, child health, aging, and community heath supports a paradigm shift in the use of strength-based versus needs-based approaches to support health and well-being and therefore should be considered (Feeley & Gottlieb, 2000; Saleebey, 1996; Waters, 2015). Further, there is the potential for “role creep” which has been reported by social workers and is defined as the blurring of boundaries between provider roles in health care (Craig, Betancourt, & Muskat, 2015). Role creep has also been reported as a job stressor when workers have not been prepared for new roles that they are expected to take on (Denny, Wells, & Cunningham, 2011). Existing disciplines such as nursing and social work can review their own competencies to understand where they relate to navigation roles and justify working in these areas. Managers thus need to take into consideration professional development of service providers for new roles that they may be expected to take on.
New or improved navigation roles are only relevant when there are services to which clients can be directed: “navigation to nowhere” has been identified as a challenge by Anderson and Larke (2009a, 2009b) who were working in a rural community in British Columbia to support mental health and addictions. Our respondents reported a significant challenge providing navigation support where there were long waitlists for programs, placements, and services. Moreover, clients faced multiple obstacles accessing services when they become available. Participants described frustration with limited resources, low income, transportation issues, or inadequate funds for child care that prevented clients from getting the services arranged for them. The challenges of providing navigation are complex.
The descriptions our participants provided of their clients were typical of marginalized groups or those suffering health inequities: presence of mental health, addictions, disabilities and chronic diseases, histories of trauma or abuse, and facing obstacles such as low income, unemployment, low education, lack of social supports, transportation, and housing issues (Health Equity Impact Assessment (HEIA) Workbook, 2012). It is not surprising that these clients require navigation support, as differential access to key social determinants of health is the underlying foundation of health disparities (Gardner, 2008). Issues of employment and housing were high on the list of obstacles for clients, but were also among the activities performed the least frequently by our participants. There appears to be a need for client specific priority planning to address issues with highest impact on individuals and families.
Strengths and Limitations
The limitations of this study included the relatively short timeframe for data collection and the use of convenience and snowball sampling. This sampling method likely resulted in an overrepresentation of participants from acute care and small number of participant from other sectors. We did not collect demographic data related to the ethno racial background of our participants, which may have contributed to a deeper understanding of issues of power associated with relational work. Nevertheless, we were able to reach a large number of respondents representing a broad range of disciplines and organizations from both health and social services from one large urban Canadian city. To the best of our knowledge, this is the first descriptive survey of providers of systems navigation support in Canada.
Conclusion
The results of this survey provide a snapshot of what various providers from different disciplines and organizations are doing to provide navigation support to clients in a large urban Canadian community. Although we have described characteristics of clients from the provider's perspective, the views of clients themselves are a critical missing piece of this picture. This is needed to understand if and how system navigation influences and impacts clients in improving their health which points to a key area for future research. Studies which determine best practices in overcoming barriers to navigation are also warranted. Navigation is one small piece of the puzzle that can enable more integrated services for clients, especially those who suffer from long-term health and social conditions. The current sociopolitical context in Canada is creating further economic and social marginalization by creating processes of exclusion and health inequities for vulnerable groups (Bryant et al., 2011). Public policy changes are needed to recover some of the losses over the past 25 years to the public welfare system and social supports. In the meantime, individuals who need navigation support are growing in number. The work of navigators is meant to alleviate the barriers to health and social care, but does not address the larger systemic issues that have created inequities and greater needs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study described in this article was supported by Community Health Planning & Integration, Public Health Services, Hamilton, Ontario, Canada.