
Abstract
Multilayer compression bandaging (MLB) for breast cancer-related lymphedema (BCRL) patients may be easier to apply during nighttime sleep. Little is known about the specific effects of nighttime multilayer bandaging (NMLB) alone. In the present study, we examined whether NMLB alone significantly improved the negative symptoms of BCRL such as excessive swelling and an unpleasant feeling. A pre–post study was conducted as a basis for the development of efficient self-care treatment. Eight middle-aged female patients with unilateral upper extremity BCRL voluntarily participated in this study. During the first 2 weeks, the participants were educated and trained in the self-bandaging technique. The participants then wore MLB on the affected extremity for the following seven nights at home from bedtime to the next morning (hereafter referred to as the intervention). We measured the segmental total body water (STBW) volume on the affected upper extremity using bioimpedance spectroscopy and subjective symptoms using a visual analog scale. Each parameter was measured at the beginning and end of the intervention periods. It was found that the STBW volume on the affected upper extremity decreased significantly during intervention. The mean STBW volume reduction was 0.088 L (p = .047, 95% CI [0.001, 0.175] L]). Subjective symptoms related to swelling (i.e., tightness, heaviness, and fullness) decreased significantly during intervention (p < .05). In conclusion, decrease in the STBW volume and subjective symptoms on the affected upper extremity were observed at the end of the intervention. These results suggest that NMLB reduces both swelling and swelling-related symptoms of BCRL.
Keywords
Introduction
Breast cancer-related lymphedema (BCRL) is a common chronic complication occurring after axillary lymphadenectomy (Petrek, 1996). The affected upper extremity becomes swollen from the accumulation of excessive interstitial fluid by a blockage of the lymph vessels. Almost one third of breast cancer patients suffer from BCRL (Petrek & Heelan, 1998) and it causes substantial deterioration in the patient’s quality of life (Chachaj et al., 2010; Petrek, 2004; Ridner, 2005).
Multilayer compression bandaging (MLB) has beneficial effects upon lymphedema. A previous study with 38 BCRL patients shows that almost 24-hour MLB reduces the excess limb volume by 26% (Johansson, Albertsson, Ingvar, & Ekdahl, 1999). MLB can be adjusted to the shape of a patient’s extremity and can thereby fit many types of patients. Although MLB has to be rewrapped at least once a day because the applied sub-bandage pressure diminishes by around 60 % after 24 hours (Damstra & Partsch, 2009), this characteristic allows us to use it safely throughout 24 hours period. MLB combined with exercise is also thought to increase the benefits of the treatment because muscle movement during exercise, that is, “muscle pump,” can accelerate the reduction of volume from lymphedema (Casley-Smith, Boris, Weindorf, & Lasinski, 1998; Partsch, 1991). This suggests that MLB therapy is better suited to the daytime when physical activity increases. MLB treatment during the day, however, may not be viable for the patient. According to Tsai, Hung, Yang, Huang and Tsauo (2009), patients were only able to wear MLB for approximately 50% of the prescribed treatment period during the day. In contrast, the patients were able to wear MLB for 90% of the prescribed time during the night. Accordingly, we focus on the effects of nighttime MLB (NMLB) therapy alone as it appears to be a more practical form of treatment. That is, the purpose of this study was to test whether NMLB alone significantly improved the negative symptoms of BCRL such as excessive swelling and an unpleasant feeling. In addition, it also examined whether NMLB interferes with the patients’ daily life in terms of sleep conditions and daily physical activities.
Material and Methods
Settings and Participants
A prospective clinical pre–post study was conducted. The protocol of the present study was approved by the Nagoya University Hospital’s Ethics Committee (No. 2015-58) and conforms to all conventions governing ethical conduct as stated in the Declaration of Helsinki. Written informed consent was obtained from all patients.
Patients with unilateral BCRL who were referred for lymphedema care in an outpatient unit of the Nagoya University Hospital were assessed for eligibility with the following criteria. Participants were required to have a prior history of radical treatment for their breast cancer. In order for a diagnosis of lymphedema, the affected arm circumference must have exceeded the contralateral upper extremity by more than 1 cm.This threshold level demonstrated the adequacy of diagnosing lymphedema in Japanese BCRL patients (Kitamura & Akazawa, 2010). Primary and adjuvant breast cancer treatments must have been completed at least 6 months prior to the present study. Ongoing hormonal therapy was allowed. All participants must have completed basic education in self-care techniques for BCRL through their practitioner. We excluded patients who had clinical evidence of ongoing breast cancer and or a serious comorbidity, had received lymphedema treatment within 6 months, had applied a new compression sleeve within 1 month, had an infection in the affected upper extremity, or could not understand or conduct self-treatment.
Intervention
The present study consisted of a 2-week preintervention period (Days 1–14) then a further 1-week intervention period (Days 15–22) (Figure 1). The schedule did not include 3 or more nonworkdays, that is, holidays and weekends. Participants maintained their daily life habits as usual through the entire schedule of the study, except for the measurement day (Days 8, 15, and 22). The participants were prohibited from eating or drinking anything 2 hours before measurement.
Schematic illustration of the schedule.
During the preintervention period, the participants were educated in how to apply MLB over five sessions (Figure 1). The MLB techniques which we used in the present study are shown in Figure 2. During these five sessions, they learned how to apply MLB step-by-step.
The procedure for participants applying MLB with some check points (listed in order). (a) Two gauzes (Elastomull®, BSN medical GmbH & Co.KG, Hamburg, Germany) were applied to the fingers and hand. Cotton tube stockinette (Tricofix®, BSN medical GmbH & Co.KG, Hamburg, Germany) was applied to the entire arm. (b) Two pieces of foam padding (Artiflex® and Compri Foam®, BSN medical GmbH & Co.KG, Hamburg, Germany) were placed on the hand and wrapped around the arm. (c). Three short stretch bandages (6, 8, and 12 cm width) (Comprilan®, BSN medical GmbH & Co.KG, Hamburg, Germany) were applied in the form of a spiral with a 50% overlap. The first short stretch bandage (6 cm width) was wrapped around the hand. The second bandage (8 cm width) was placed on the wrist and wrapped up to the elbow. The third bandage (12 cm width) was placed on the wrist and wrapped up to the shoulder. (d) Comfortable application (i.e., no pain, no numbness, and no paleness in fingertips) was checked and gradient pressure was applied from distal to proximal at 20–30 mmHgi (sub-bandage pressureii).
In the first session (Day 1), the researcher showed the whole procedure by applying MLB to the participants’ affected arm. In the second session (Day 3), participants practiced applying MLB by themselves with the researchers’ help. From the third to last session (Days 8, 11, and 15), participants further practiced the procedure so as to meet requirements.
Participants were provided with feedback on correct sub-bandage pressure levels during training. At the end of the educational session, we confirmed participants’ understanding regarding MLB technique and knowledge. We assessed whether the participants performed the MLB properly and understood the check points which had been taught in the educational sessions, for example, MLB with no pain, no numbness, and no paleness in the fingertips (see Figure 2(d)).
Each educational session took about 60 minutes. They wore MLB for about 5–10 minutes during each session.
During the intervention period, the participants wore MLB on the affected upper extremity by themselves through the night: The participants applied MLB immediately before they slept and removed the bandages after waking.
Measurements
During the baseline period (Days 8–14) and the intervention period (Days 15–22), participants were required to record their waking time and sleep time and the start and end time of MLB application in a diary. This was done to track the participants’ routines and to confirm that daily life continued as usual. The participants were expected to apply NMLB as long as the duration of sleep in the baseline period. In addition, the researchers measured the participants’ daily physical activity or metabolic equivalent tasks (METs) by multiplying METs by hours divided by days (MET × h/day) with the triaxial accelerometers (Active Style Pro HJA-750 c; OMRON HEALTHCARE Co., Ltd., Kyoto, Japan). METs measured with the triaxial accelerometers are similar to those measured by the indirect calorimetry (daglas-bag method) which is considered the gold standard (Ohkawara et al., 2011; Oshima et al., 2010).
The following measurements were made on Days 8, 15, and 22. To verify the effect of NMLB, segmental total body water (STBW) of the upper extremity was measured with bioimpedance spectroscopy (Inbody® S10; InBody co ltd, Seoul, Korea) in a supine position. STBW represents the sum of intracellular fluid and extracellular fluid of a certain segment. The Inbody® parameter is similar to measurements by the deuterium oxide dilution method which is considered the gold standard (Bedogni et al., 2002). The STBW volume was calculated with the manufacturer’s software (Lookin’body®120; InBody Co Ltd, Seoul, Korea). Measurement was not undertaken on Day 1 because such data might not be accurate if it was affected by participants’ life immediately before commencement of the study.
Changes in the shape of the affected upper extremity during the intervention period were recorded and monitored with a digital camera. The severity of subjective symptoms (i.e., tightness, limiting arm use, heaviness, fullness, pain, and numbness) was measured using a 100-mm visual analog scale (Gift, 1989). The symptoms were selected from previous studies which aimed to verify the effectiveness of BCRL treatment (Hamner & Fleming, 2007; Williams, Vadgama, Franks, & Mortimer, 2002).
Before the measurements, participants urinated and then wore a designated gown. After remaining in a climate chamber for over 20 minutes at 24℃ and 50% humidity, the measurement commenced.
Statistical Analysis
A paired two-tailed t test was used, and p values of less than .05 were considered significant. All data analyses were performed using the SPSS Statistics version 23 (IBM, USA).
Result
Demographic Data
Between May 2015 and May 2016, 11 patients were initially eligible to participate in the study, but 3 participants had to leave the study for personal reasons. No participants dropped out during the intervention period. Thus, a total of 8 female patients finished the study and are included in the analysis.
Demographic Characteristics.

Note. BMI = body mass index.
Comparison of the Objective Parameters Between Two Different Periods (n = 8).

Note. SD = standard deviation; Mins = minutes; METs × h/day = metabolic equivalent tasks (METs) by multiplying METs by hours divided by days.
Water Composition and Physical Presentation of the Upper Extremity
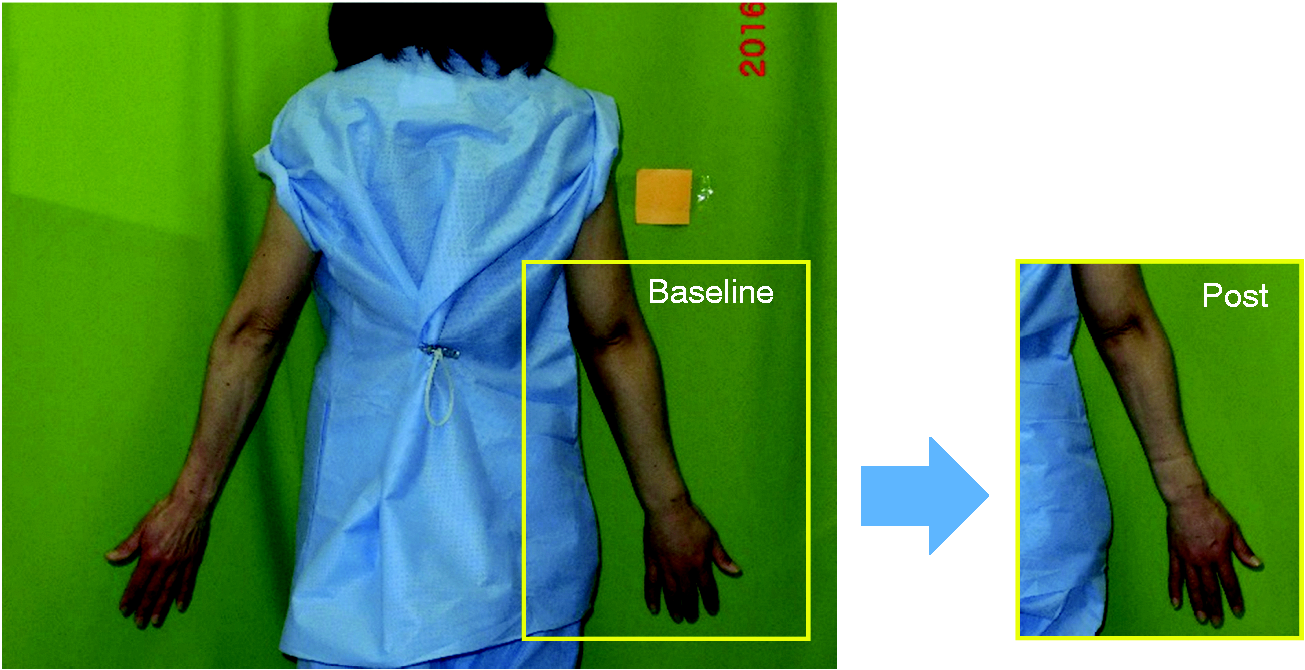
During the baseline period, the mean STBW volume on the affected upper extremity was 1.752 ± 0.336 L at the preliminary measurement and 1.795 ± 0.327 L at the baseline measurement (The mean difference: −0.042, p = .174, 95%CI [−0.110, 0.024] L). During the intervention period, the mean STBW volume on the affected upper extremity was 1.795 ± 0.327 L at the baseline measurement and 1.706 ± 0.304 L at the postintervention measurement (Figure 3). The volume of STBW decreased significantly at the postintervention (p = .047), with a mean STBW reduction of 0.088 L (95%CI [0.001, 0.175] L) of the affected upper extremity (Figure 3). An example of visual changes in the physical presentation during the intervention period is shown in Figure 4.
Mean STBW volume in the bandaged upper extremity: at baseline and postintervention (n = 8). The volume reduction was 0.088 L (p = .047, 95% CI [0.001, 0.175] L). *p < .05, T-bar shows standard deviation. An example of visual changes in the affected upper extremity (on her right upper extremity), during the intervention period. The picture on the left shows the baseline (Day 15) and the one on the right is postintervention (Day 22).
Severity of Subjective Symptoms
Comparison of the Subjective Symptoms by the Day of the Measurement with VAS (n = 8).
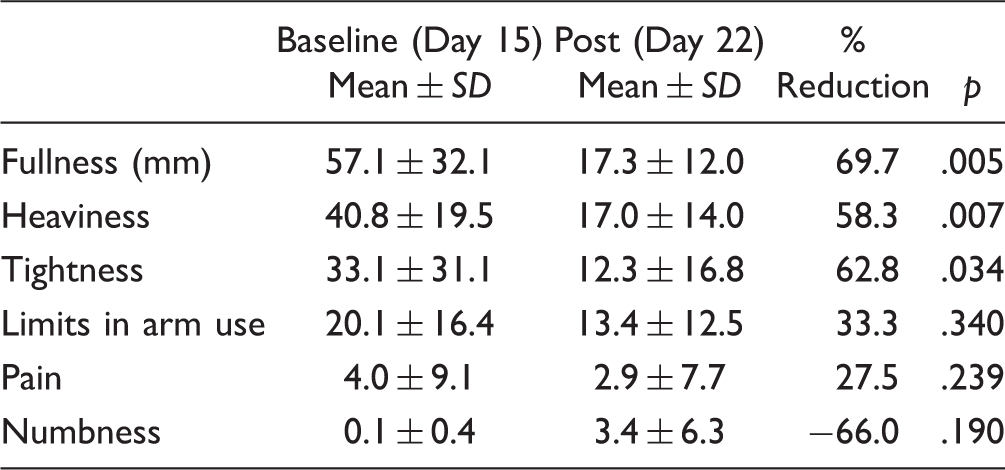
Note. SD = standard deviation. Ranging from a 0 mm (none) to 100 mm (worst possible).
Discussion
Swelling Reduction
We examined whether NMLB alone has a beneficial effect on lymphedema. Using impedance spectroscopy, the present study demonstrated the reduction of STBW in the affected arm. STBW volume decreased by approximately 0.088 L (average of eight participants) from the baseline (value at Day 22). Such reduction was not observed in the baseline period, that is, there was no significant difference in STBW between the preliminary (Day 8) and baseline (Day 15) measurement. Comparative analysis of the unaffected arm was not undertaken due to inherent variation between the two limbs (dominant and nondominant) related to differences in impedance (Smoot, Wong, & Dodd, 2011). Our results using the evaluation in the same arm at pre- and postintervention seem to have an advantage in verisimilitude and suggest that NMLB alone has a beneficial effect on lymphedema.
Up to now, when the objective was to reduce lymphedema swelling, MLB was recommended in combination with activity (International Lymphoedema Framework, 2012). Based on reports from the participants’ diary, all participants rested at night and worked in daytime during the entire study period. That is, it could safely be assumed that their physical activity level at night was lower than during the day. In short, the findings of the present study suggest that MLB during periods of low activity (i.e., nighttime) also has the ability to reduce swelling from lymphedema.
Changes in Subjective Symptoms
We found that subjective symptoms improved at the postintervention: patients reported that tightness, heaviness, and fullness had subsided at the postintervention. Such symptoms were reported with a higher intensity level at the beginning of our intervention. Moreover, the symptoms are also thought to be directly related to extremity enlargement. These results thus suggest that NMLB treatment is effective in reducing the negative impact of lymphedema swelling.
Self-NMLB as User-Friendly Way
Previous treatment for BCRL recommends MLB 24 hours per day (International Lymphoedema Framework, 2012). Twenty four-hour treatments, however, inflict various forms of suffering on patients such as spending enormous time and effort, a lack of enjoyment when going out due to a soft cast on the extremity all day, being forced to live an inconvenient life due to a limitation in the range of motion. This suffering raises the problem of nonadherence. Tsai et al. (2009) indicate the difficulty of day time usage of the bandage as patients only used the bandage for an average of 7.8 hours during the day (when it was supposed to be 16 hours). On the other hand, less difficulty in night usage was noticed. Patients used the bandage for an average of 6.0 hours (it was supposed to be 8 hours). Forner-Cordero, Munoz-Langa, Forner-Cordero, and DeMiguel-Jimeno (2010) showed the importance of participants’ dedication to MLB in conjunction with treatment efficacy. These studies have shown that MLB needs to be more practical in order to show its facility.
From the following results, we confirmed that NMLB may be practical and encourage patients to use their bandages more regularly. First, NMLB is easier because by the beginning of the intervention period we found that all participants were able to master the MLB technique and achieve appropriate sub-bandage pressure independently. Second, NMLB may be considered safe since we found none of the participants dropped out and no adverse events occurred. Third, it appears that the participants’ life is not interfered with by NMLB, as we found that the duration time of sleep and daily physical activity had not changed between the baseline period and the intervention period. Fourth, participants’ compliance with NMLB was good during the intervention period. We found that participants were able to use MLB by themselves at night as expected (i.e., recall the mean duration of sleep during the baseline period vs. the mean duration of NMLB during the intervention period: 394 vs. 403 minutes). Thus, NMLB treatment may encourage patients to use their bandages more regularly and so is likely to extend the application range of the compression bandages.
Limitations
Although the comparison of pre- and postintervention tests showed NMLB to be useful for clinical practice, our small sample size creates limitations regarding determination of the efficacy of NMLB and variations relating to participants’ demographic data (e.g., age, weight, BMI, and lymphedema severity). In addition, our short duration period and the lack of a control group also create limitations regarding the scope of our findings.
Accordingly, future research may wish to address these limitations to clarify the effects of NMLB.
Conclusion
Decrease in the STBW volume and subjective symptoms on the affected upper extremity were detected at the end of the intervention period. This suggests that NMLB alone reduces both swelling and swelling-related symptoms with BCRL. These results are evidence of the effectiveness of MLB in BCRL treatment.
Footnotes
Acknowledgments
The authors would like to thank associate professor Robert Joel Deacon in the Writing Center at Nagoya University for his editorial advice, and Aya Ando and Sayami Matsubara in the outpatient department at Nagoya University Hospital, Japan for their constructive support and comments throughout the study process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants-in-aid of The “YAMAJI FUMIKO NURSING FUND” and JSPS KAKENHI (Nos. 15K20666, 15K11468 and 16H05563).