
Abstract
Video-based care has become a routine part of outpatient care delivery, yet older adults continue to face barriers in accessing and engaging with this modality. This study analyzed the comments provided within 7155 patient experience surveys from adults aged ≥65 years across a large, multi-specialty medical practice to identify challenges experienced with video-based visits. Thematic analysis revealed the highest proportion of positive comments were related to experience with people (71%), while barriers were often related to technical issues with video tools (73%). Most comments related to processes were positive, often highlighting convenience (67%). Using design thinking, we mapped the patient journey and proposed both immediate solutions, such as testing environments and clearer instructions, and long-term innovations like voice-guided support and emotionally intelligent interfaces. Our findings suggest that while video visits offer convenience, they must be redesigned with older adults in mind to ensure equitable, effective, and human-centered care.
Plain language summary
Older adults face challenges using video visits for healthcare, including technical issues, confusing processes, and feeling less connected to providers. This study analyzed patient feedback and proposed solutions, like clearer instructions and voice-guided tools, to make video visits easier, more personal, and better suited to older patients’ needs.
Introduction
Video-based appointments with healthcare providers have become an integral part of clinical care since wide-spread implementation of telemedicine during the COVID-19 pandemic. Video-based care helps bridge a gap persisting among patients in need of healthcare services but experiencing diminished care access. Patients residing in rural or medically underserved areas, and experiencing transportation barriers, diminished socioeconomic status or physical disabilities can be uniquely served by video-based care.1,2 In the United States, older adults are more likely to experience transportation barriers due to physical limitations, inability to drive, or lack of access to vehicles, and many older adults reside in rural or medically-underserved areas.3,4 The intersection of these experienced barriers makes older adults prime beneficiaries of video-based medical care.
Although video-based medical care appears to be a good option for this population, research continues to demonstrate that older adults experience barriers to using video-based care. Older adults experience several patient-level barriers in their ability to connect to video-based care, including digital literacy related to operating video care platforms and troubleshooting audio and video issues.5–8 Older adults also experience physical limitations in their ability to successfully engage with video-based medical care, including hearing, vision, memory, and motor impairments.5,7,9 Evidence has demonstrated the instrumental role of caregivers in facilitating participation in video-based medical appointments among older adults,6,8,10 and the enabling abilities of “on-demand” technical support to connection to and participation in video appointments.8,11
As academic medical centers and multi-specialty clinical practices often leverage shared digital infrastructure to support video-based appointments, opportunity exists to understand the barriers experienced by older adults using video-based care across multiple general and specialty medical practices for multiple care needs. To date, most published studies have evaluated single specialties, such as geriatrics 12 or occupational therapy,10,13 specific populations, such as patients of the US Veterans Health Administration8,13 or individuals residing within independent or skilled living facilities. 9 Additionally, assessments to date have been of limited sample sizes. No published studies were identified leveraging design thinking to advance current barriers experienced by older adults during video-based healthcare appointments into technical capabilities enabling ideal video-based healthcare appointments for older adults.
The present study aims to describe the barriers experienced by older adults who completed a video-based visit with a large, multi-specialty, integrated medical center, and to leverage design thinking to transform reported barriers into idealized procedures for video-based medical appointments. We analyzed responses from 7155 patient experience surveys collected following video-based appointments as part of routine clinical operations. Thematic analysis was used to identify, analyze, and report on patterns identified within the open-ended items as reported by patients after video-based appointments. Journey mapping was used to visualize the experiences of patients and to outline major barriers experienced across the video-appointment process. Design thinking was used under a human-centered framework to identify solutions to address major barriers across differing time horizons proposing short-term and long-term solutions.
Methods
Study Design, Setting, and Participants
We sought to describe the barriers experienced during video-based telemedicine visits following the incorporation of video-based care as a routine part of clinical practice. We first assessed trends in video visits as a portion of total outpatient visits for older adults across a large, multi-specialty medical practice. We then described the experience of video-based care as reported by older adults and performed a thematic analysis of barriers faced by this population as reported through routine patient experience surveys. Finally, we utilized human-centered design to describe the experience of older adults using video-based care for routine healthcare needs using patient journey mapping and recommend solutions following design synthesis. The setting for this investigation is a large, academic Department of Internal Medicine with outpatient practices located at Mayo Clinic in Rochester, Minnesota, USA. These practices see over 350 000 unique patients annually within the clinical divisions of community internal medical, endocrinology, gastroenterology, general internal medicine, geriatrics, hematology, hepatology, infectious disease, nephrology, occupational medicine, palliative care, preventive medicine, pulmonary, rheumatology, and sleep medicine. As the present study utilized de-identified information collected for routine clinical operations, the Mayo Clinic Institutional Review Board deemed this project to not be human subjects’ research.
Data Collection
Outpatient Video Visits
To understand the rate of video-based care provided to older adults over time, we extracted all completed visits from our scheduling software from January 1, 2018 to December 31, 2024 for all outpatient clinics within the Department of Internal Medicine. We compared visit rates by year to understand differences between in-person and video visits for patients aged ≥ 65 years. We also examined characteristics of patients aged ≥65 years who had a video visit in 2024 by patient experience survey completion.
Patient Comments Following Video-Based Visits
Routinely collected experience surveys as part of clinical care from January 1, 2024 to December 31, 2024, for patients aged ≥ 65 years were leveraged for this investigation. Patient experience surveys are deployed via a simple random sample of unique patients among eligible encounters for each provider, up to a maximum of 50 patients per month. Patients receive either a paper or email survey and a reminder delivered 1 week later. Sample exclusions include therapy and nurse-only visits, deceased, “Do Not Survey” list, and vulnerable patients. Once a patient is surveyed, they cannot be selected again for 30 days. A copy of the deployed survey instrument is included as Supplemental Appendix 1.
Data Analyses
Qualitative Analysis
Thematic analysis of patient comments was completed leveraging grounded theory. Open coding was used for the identification of initial themes for all comments included with returned patient experience surveys. We examined surveys received from patients aged ≥ 65 years, who had a telemedicine visit with a provider from any area of the entire Rochester Department of Medicine during January 1 to December 31, 2024. Comments in response to the prompt “Please tell us about anything that impressed you about your experience.” or to the prompt “Please tell us about anything that disappointed you about your experience.” were included for analysis. After removing general comments “Good,” “Great,” etc, keywords were derived from patient comments via close examination of responses, whereby recurring patterns and terms arose. Coding was performed to capture core messages included within patient comments, enabling data transformation into generalizable, theoretical elements describing the barriers experienced by patients engaging with Telemedicine visits. Iterative review of comments was performed until no new themes were identified, and when all coders agreed upon the identified themes. A completed Standards for Reporting Qualitative Research (SRQR) checklist is provided as Supplemental Appendix 2.
Research Team Descriptions and Reflexivity
Themes were derived from coded values. Qualitative analyses were performed by 5 analysts. Our research team comprises individuals with diverse backgrounds and experiences, enriching our study approach. Analyst A, a 45-year-old white male, brings extensive experience in statistical programming and remote work. Analyst B, a 51-year-old white male, contributes insights from sociology, psychology, and public health, informed by his personal caregiving experience. Analyst C, a Generation-Z white female with a degree in statistics, offers a fresh perspective on digital health and chronic conditions. Analyst D, a first-generation Asian American woman trained in public health science and epidemiology, provides a critical lens on healthcare access and equity. Analyst E, a 41-year old white female with advanced training in healthcare delivery science, brings a wealth of experience from public health and healthcare systems. Our collaboration is grounded in mutual respect and critical dialogue, allowing us to challenge assumptions and enrich interpretations. We recognize that our positionalities are not fixed and are committed to ongoing reflexivity throughout the research process.
Quantitative Analysis
Simple count (n) and proportion (%) are provided as descriptive statistics for all reported data. Age was compared using the Wilcoxon Rank Sum and categorical variables were compared using the Chi Square test for independence (Χ2). All data management and statistical analyses were performed using Statistical Analysis Software (SAS) Version 9.2 (Cary, NC). Results are considered significant if the P-value is less than .05.
Design Synthesis
Using a human-centered design framework, we translated key themes into a visual patient journey map that illustrates the patient experience from scheduling a video-based appointment to engaging with technology and participating in the visit. Journey maps can be used to highlight each stage of the experience and to pinpoint areas for improvement to inform the development of an ideal video-based visit experience. 14 Notes from stakeholder sessions were consolidated and organized according to the relevant process steps, with repeated observations reinforcing data saturation. 15 These insights, grounded in the team's understanding of outpatient practice workflows and validated by clinical team members, revealed systemic challenges throughout the patient journey. Guided by human-centered design principles, we generated targeted opportunities for improvement, each aligned with 1 of 3 conceptual pathways. 15
To address immediate barriers experienced with video-based care, we applied the initial phases of design thinking: empathize, define, and ideate. 14 This approach enabled rapid solution generation. Simultaneously, we extracted future-forward concepts of a video-based care experience, laying the grounded for transformative innovation to better meet the needs of patients in the future. 16
Results
Rate of Video Visits for Older Adults Over Time
The rate of video-technology use for outpatient medical appointments for adults aged ≥ 65 years increased dramatically from around 1% prior to the Covid-19 pandemic in 2020, to more than 13% post-pandemic (Figure 1). Increased use of video-technology has remained above 13.5% of the total outpatient visits for those aged ≥ 65 years for the subsequent years.

Rate of completed outpatient clinic visits completed in person (light grey bar) versus via video (dark grey) among patients aged ≥ 65 years across a large, multi-specialty academic medical center. Number of visits is provided along the y-axis with year provided along the x-axis. Volumes for in person clinic visits and video-based visits are provided, along with the rate of video-based visits as proportion of overall clinical volume in parentheses.
Patient Experience With Video Visits for Routine Outpatient Care
The Mayo Clinic Office of Patient Experience received 7155 responses to their routine patient experience surveys for video-based care among patients aged ≥ 65 years in 2024, out of a total of 56 966 unique patients seen across the Department of Medicine outpatient clinics (Supplemental Appendix 3). Most of our survey response population was male, of white race and non-Hispanic ethnicity, married or within a life partnership, residing within a location that is not local to our clinic site, and had completed college or post-graduate education. Our survey response population differed from the overall population seen based on age, gender, race, ethnicity, marital status, distance of primary residence from our clinic site, highest level of education achieved, and whether the patient was paneled within our primary health care practice.
Barriers Experienced by Older Adults With Video-Based Appointments
Three themes were identified via thematic analysis of 1012 comments provided within patient experience surveys of older adult patients following video-based appointments for routine care. Table 1 provides the proportion of comments associated with each sentiment (Positive, Negative, Mixed/Neutral) within each of the following themes:
People: individual preferences, relationships, healthcare team / staff Process: login process, instructions, waiting room Technology: connectivity, video, audio
Thematic Review of Patient Experience Surveys Provided by Older Adults who Participated in a Video-Based Outpatient Visit (N = 1012).

Among 74 responses in the “People” domain, 71% were positive, highlighting effective communication and enhanced understanding through visual aids. Patients reported that “Several staff members provided excellent explanations and guidance to make the Zoom conference easy, efficient, and effective.” and that “[Doctor] used a split screen to show previous data and helpful information. Those visuals increased my understanding.” Thirteen percent of respondents expressed dissatisfaction with the lack of personal connection, saying “The technology was great and the connection was wonderful. It was too bad that the doctor severed any possibility of a personal connection.” The “Process” domain, comprising 177 responses, showed a similarly high proportion of positive feedback (67%), emphasizing convenience and efficiency, an “Excellent way for an annual checkup. Convenient when you don't live locally.” Though 22% reported logistical frustrations, such as connection delays. “It took 1 3/4 hours to connect. Once [Doctor] called, the visit was perfect. Help lines to connect me with video were ineffective. Very frustrating trying to connect for almost 2 hours.” The “Technology” domain, with the largest response pool (N = 245), revealed a more critical perspective: only 28% of responses were positive, while 42% were negative, citing issues like video freezing and access denial. Two patients explained “Call was scheduled as a video conference. When I attempted to check in, I was denied account not able to have video conference.” And “A number of times during the Zoom appointment, the video froze which put it out of sync with the audio. This made the conversation difficult to follow. It could have been my end that was the problem, or just a bad connection.” Mixed or neutral sentiments were present across all domains, reflecting nuanced experiences. Additionally, the table identifies specific barriers encountered during virtual visits and proposes both short-term and idealized solutions, such as implementing hold music or visual countdowns to mitigate uncertainty during waiting times.
Design Synthesis and Proposed Solutions to Barriers Experienced by Older Adults
A summarized version of the journey experienced by patients as they schedule, prepare for, and attend their video-based outpatient appointments is depicted in Figure 2. The Scheduling phase includes self-scheduling or finalizing appointment details and confirming payment. In the Preparing phase, patients are instructed to download necessary communication tools and test their connection. The Connecting phase involves joining a virtual waiting room, checking in, and making any necessary appointment adjustments. Annotations highlight operational challenges and improvement opportunities, such as the need for alternative confirmation methods for patients without portal access, the potential for automated reminders, and the importance of proactive communication to mitigate technical barriers. Emphasis is placed on enhancing patient engagement, reducing barriers to access, and ensuring a seamless virtual care experience. Design synthesis and creation of short- and long-term, idealized solutions to address the common barriers reported by older adults following video-based appointments are reported in Table 2.
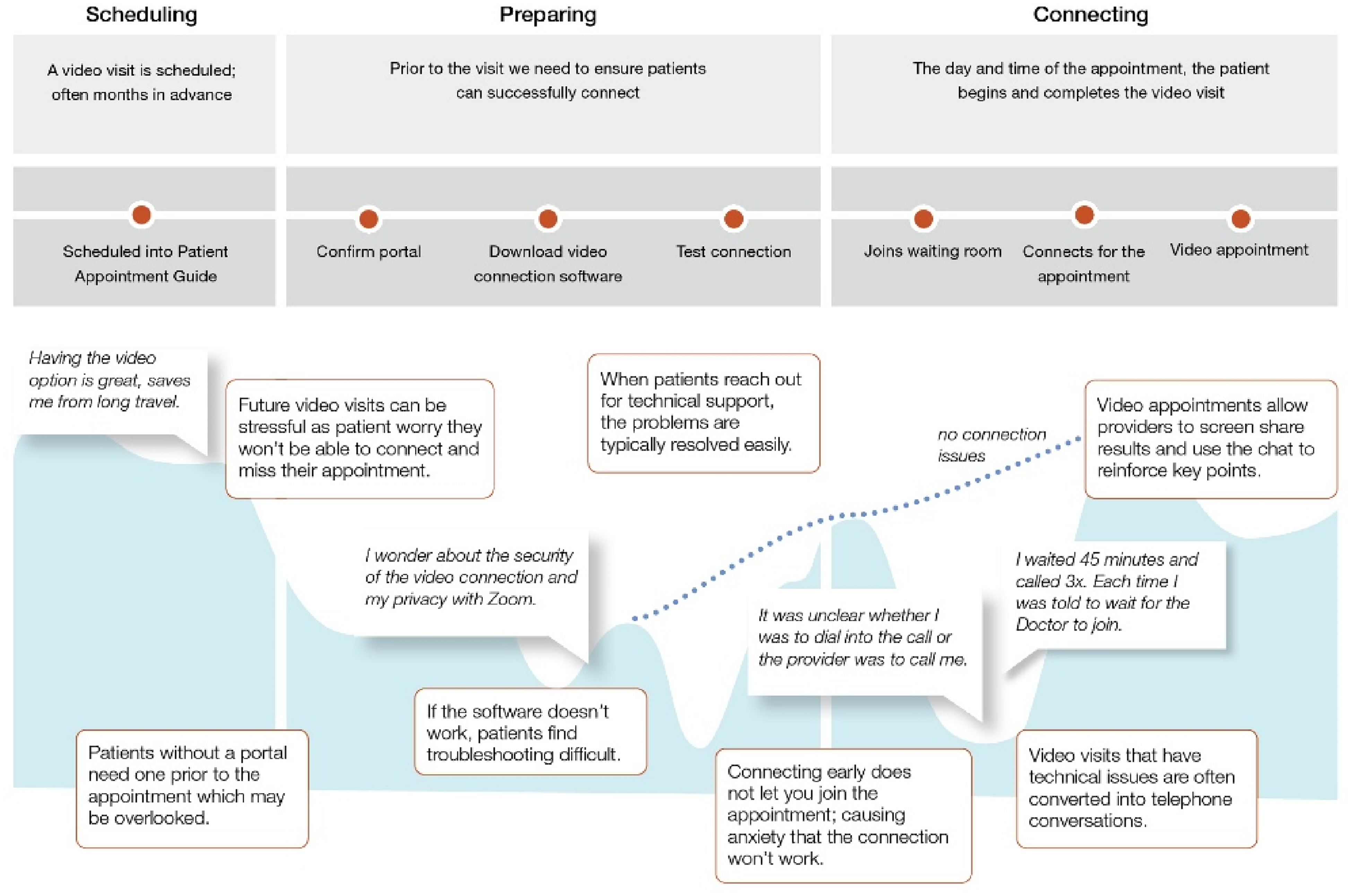
Patient journey map of older adult experiences with video-based visits as part of routine clinical care.
Design Synthesis and Future Ideation of Solutions to Meet Barriers Experienced by Older Adults in Use of Video-Based Visits for Routine Clinical Care.

Discussion
Implications for Practice
Across our multi-specialty, outpatient practice, we observed an increased rate of video-based appointments among individuals aged ≥ 65 years of age during the Covid-19 pandemic, with consistent utilization of video-based care in the subsequent years as proportion of total care delivered. Thematic review of all patient-provided comments revealed insight into the people, process, and technology dynamics experienced by patients aged ≥ 65 years who completed a video-based visit for outpatient care in 2024. Patients described challenges establishing personal connection during video visits, loss of nonverbal cues, distracting virtual backgrounds, and perceived provider multitasking. Logistical issues with the process to log-in procedures and virtual “waiting rooms,” as well as technical issues with audiovisuals and internet connections, were also prominent.
To address these concerns, we propose immediate practice-level solutions, such as sandbox environments that allow patients to test the video visit prior to their appointment. Additionally, reducing virtual wait times and implementing messages of reassurance about connection status may improve patient experience with video visits. Providers can enhance engagement by adopting best practices for digital interactions, including warm greetings, active listening, and summarization. Screen-sharing and live chat features were positively received and should be leveraged to support patient understanding and personal connection.
Implications for Policy
The persistence of barriers among older adults since wide-scale adoption 5 years ago highlights the need for system-level interventions. Digital health literacy remains a critical determinant of telemedicine engagement,5,7–9,11 with many older adults expressing anxiety and difficulty navigating the multi-step processes currently in place.9,13 We support the call for digital health literacy screening to be included as standard intake for all healthcare systems who utilize telemedicine. 17 Such screening could identify patients in need of support to engage with video-based care and inform tailored interventions.
Equity in access to video-based care must be prioritized. Policies to promote inclusive design and outreach strategies to support patients across age groups could ensure video care systems are accessible and usable. As national medical societies continue to publish best practices to support digital models of care, guidelines should be expanded to include workflow redesigns that move the delivery of digital care beyond the traditional brick-and-mortal models.
Implications for Research
Much of the published literature to date reflects the experiences of early pandemic conditions, when video-based models of care were rapidly developed and deployed. 8 Our findings contribute the experiences of older patients post-surge, demonstrating that barriers to video-based care for older adults persist. Future research should explore the role of innovative support options, like voice-activated digital navigators 18 and real-time sentiment analysis tools. 19 These technologies, already being used in education and ecommerce, may offer hands-free, intuitive support using voice-prompting to guide users through the use of digital tools and live analysis of conversations to identify negative emotions to immediate course correct when a patient's experience is challenged. Emerging technologies like these offer scaleable solutions to improve the healthcare experiences of older patients.
Additionally, research is needed to design and evaluate alternative workflow models that include novel aspects like asynchronous scheduling and wait-less video visits. Our study is among the first to report patient-reported challenges with virtual “waiting rooms,” including uncertainty about connection status and provider availability. Investigating the impact of clinical workflow design on patient experience and satisfaction will be essential as video-based care continues to evolve to greater meet the needs of people.
Strengths and Limitations
Our study included a large, randomly sampled survey (n = 7155) embedded within a large, multi-specialty clinical practice, enhancing the ecological validity of our findings. A mixed-methods approach, including design thinking and journey mapping, allows for actionable insights based on barriers experienced by older adults in use of video-based care. However, the cross-sectional nature of our study and reliance on self-reported barriers may introduce reporting bias. The response sample was from a single, tertiary healthcare system, which limits our generalizability. Our assessment for response bias shows that our respondents differed significantly than the patients seen at our outpatient practice at large, with overrepresentation of white, educated, married individuals. These factors may limit the generalizability of our findings across populations, particularly underserved groups. While our sample size increased our statistical power, the qualitative basis for our approach precluded our ability to adjust for differences across populations. Finally, while our findings align with existing literature, this study offers limited novelty but reenforces that the barriers experienced by patients during the initial surge in video-based care persist and have not been adequately addressed. Future research should include targeted recruitment to facilitate broader representativeness and understanding.
Conclusion
Video-based care has become a routine part of clinical care for older adults since the COVID-19 pandemic, yet persistent barriers continue to limit access and use. While prior studies have documented general challenges, particularly related to the time period closest to the pandemic, our work offers a novel synthesis of patient-reported barriers. By applying design thinking and journey mapping, we move beyond descriptive accounts to propose both immediate and long-term solutions. Our findings underscore the need for video-based care to evolve beyond traditional workflows and embrace user-centered design that prioritizes the unique needs of aging populations. This study contributes actionable insights that bridge the gap between patient experience and system-level innovation to inform digital delivery of healthcare into the future.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735261416449 - Supplemental material for From Barriers to Solutions: A Design Synthesis to Improve Video Visit Experience for Older Adults
Supplemental material, sj-docx-1-jpx-10.1177_23743735261416449 for From Barriers to Solutions: A Design Synthesis to Improve Video Visit Experience for Older Adults by Lindsey M. Philpot, Priya Ramar, Rachel E. Canning, Meredith A. DeZutter, Megan M. Dulohery Scrodin, Matthew G. Johnson, Daniel L. Roellinger and Jon O. Ebbert in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735261416449 - Supplemental material for From Barriers to Solutions: A Design Synthesis to Improve Video Visit Experience for Older Adults
Supplemental material, sj-docx-2-jpx-10.1177_23743735261416449 for From Barriers to Solutions: A Design Synthesis to Improve Video Visit Experience for Older Adults by Lindsey M. Philpot, Priya Ramar, Rachel E. Canning, Meredith A. DeZutter, Megan M. Dulohery Scrodin, Matthew G. Johnson, Daniel L. Roellinger and Jon O. Ebbert in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval,Statement of Human and Animal Rights
This project was reviewed by the Mayo Clinic Institutional Review Board (IRB) and was determined not to constitute human subjects research. The analysis was conducted using de-identified data collected during routine clinical operations, and therefore did not require IRB approval under federal regulations.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent
Informed consent was not required for this project, as the analysis was conducted using de-identified data collected during routine clinical operations and was determined by the Mayo Clinic Institutional Review Board (IRB) not to constitute human subjects research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.