
Abstract
Background
Nipple-sparing mastectomy (NSM) followed by implant-based breast reconstruction (IBR) is a widely accepted for early-stage breast cancer, supporting esthetic preservation and enhancing quality of life. The BREAST-Q is the gold standard patient-reported outcome measure PROM for evaluating satisfaction and post-operative wellbeing. This study employed the newly adapted Vietnamese BREAST-Q version 2.0, to assess patient satisfaction after NSM with IBR and explore influencing factors within a Vietnamese cohort.
Methods
A pilot linguistic validation of the BREAST-Q version 2.0 was first conducted in 20 patients from July 2021 to May 2022, demonstrating internal consistency and convergent validity. A subsequent cohort of 55 post-operative patients undergoing NSM with immediate IBR (July 2022-July 2024) participated in satisfaction assessment across eight BREAST-Q domains. Statistical significance was defined at P < .05.
Results
The tool demonstrated acceptable internal reliability (Cronbach's α = 0.70) and strong convergent validity with objective esthetic scoring (r = 0.912; P < .001). Among 55 participants (mean age (43.2 ± 7.4 years), notable post-operative outcomes included Physical wellbeing-Back & Shoulder (62.3 ± 7.9), Physical Wellbeing-Chest (84.5 ± 18.6), Psychological Wellbeing (73.9 ± 15.7), and high Implant Satisfaction (81.9 ± 22.0). However, esthetic satisfaction declined significantly post-operatively (75.9 vs 65.8; P < .001). Patients ≥40 years reported higher psychological wellbeing (76.2 vs 66.3; P = .04). Reduced esthetic results correlated with lower overall satisfaction.
Conclusion
The Vietnamese BREAST-Q shows acceptable internal consistency and strong convergent validity, supporting its clinical utility. The decline in post-operative esthetic satisfaction highlights rising patient expectations, emphasizing the need for improved cosmetic outcomes and individualized care planning in Vietnam.
Keywords
Introduction
Breast cancer (BC) constitutes the first most frequently diagnosed cancer among women. Early-stage BC diagnosis notably correlates with a survival rate exceeding 93% within the first 5 years post-diagnosis. 1 Surgical intervention has consistently served as a fundamental component of BC management, often representing the primary treatment modality in early-stage cases. Mastectomy, involving the surgical removal of breast tissue, is commonly recommended as an initial therapeutic approach. This procedure may be executed with or without immediate breast reconstruction, utilizing either artificial implants or autologous tissue in the same operative session. The immediate implant-based breast reconstruction (IBR) aims to enhance patients’ physical and emotional wellbeing by restoring the natural breast appearance, significantly improving both quality of life (QoL) and overall treatment outcomes.2,3
The BREAST-Q instrument has emerged as the foremost and extensively utilized patient-reported outcome measure (PROM) for evaluating outcomes following post-mastectomy breast reconstruction. 4 Recognized for its robust validation and high reliability, it has significantly contributed to breast reconstruction research over the past decade,5,6 enhancing the understanding of how factors such as reconstruction techniques, timing, adjunctive therapies, and patient characteristics influence patient-reported outcomes.7–10 Existing literature highlights variations in baseline satisfaction levels across diverse demographic groups, identifying significant associations between patients’ body satisfaction and body mass index (BMI), as well as correlations between social confidence and variables including race, age, and socioeconomic status. These findings underscore the critical importance of pre-operative consultations addressing more than just technical aspects, ensuring interventions are customized to meet individual patient needs and expectations. 11
Although breast reconstruction outcomes are well studied in Western populations, Vietnamese patients’ experiences remain under-measured due to the absence of a validated local PROM. This study introduces the first Vietnamese BREAST-Q, providing a standardized tool to evaluate satisfaction and QoL after reconstruction within the cultural context of Vietnam. Its availability will enhance clinical evaluation, enable international comparison of outcomes, and establish a foundation for future research and quality-of-care improvement. Our study represented the first effort to translate and culturally adapt the BREAST-Q instrument into Vietnamese, rigorously adhering to standardized guidelines. This comprehensive adaptation process encompassed forward translation by two independent translators, reconciliation, backward translation by two additional bilingual experts, expert panel review, and cognitive debriefing interviews with patients representative of the intended target population. All stages were conducted under the supervision of the Q-Portfolio team to guarantee linguistic accuracy, cultural appropriateness, and conceptual equivalence with the original instrument. 12 The objectives of our study were to evaluate patient satisfaction following nipple-sparing mastectomy (NSM) with IBR using the BREAST-Q version 2.0 Vietnamese scale and to identify factors significantly influencing patient-reported satisfaction outcomes.
Methods
Study Design and Selection Criteria
A pilot study for BREAST-Q version 2 validation (10 for linguistics and 20 for tool validation) was done from July 2021 to May 2022 with inclusion criteria: (i) Small to medium-sized breast with the estimated volume less than 350 mL; (ii) Ptosis grade 1 or 2; (iii) Early-stage BC with tumor size smaller than 3 cm; (iv) Underwent NSM immediately followed by IBR. Andexclusion criteria: BMI > 30; Severe comorbidities; Smoker; Prior diagnosis and treatment of contralateral BC; Previous radiation to the breast and chest wall; Incomplete participation in treatment; Early-stage BC with neoadjuvant chemotherapy.
The study cohort was done by recruiting patients with the same criteria as the pilot study from July 2022 until July 2024.
Sample Size Calculation
Surgery for BC is a low-risk procedure. However, a multitude of complications can occur for both lumpectomy and/or mastectomy such as seroma, hematoma, infection, or skin necrosis. Injury to surrounding blood vessels, including the axillary vein. 3 In a previous study, the partial nipple necrosis was observed at the rate of 0.7%. 13 Based on this observation, the sample size was calculated using the formula for a descriptive study, resulting in a required minimum sample size of 32 at a 95% confidence level. Our study successfully recruited up to 55 patients.
Variables and Measurement Tools
The dependent variables such as post-operative complications and its severity were collected. The independent ones include age at diagnosis, tumor size, clinical stage, skin incision, complications, the Garbay for breast esthetic score, 14 and Vietnamese BREAST-Q version 2 with 8 domains relevant to surgical outcomes including: Physical wellbeing (Back & Shoulder; Chest; Sex; Psychology) and Surgery Satisfaction (Pre- and Post-operative satisfaction with breast; Breast animation deformity; Implant satisfaction) from Q-Portolio website. 15
Statistical Analysis
All statistical analyses were conducted using Stata version 12. Continuous variables were presented as medians with interquartile deviation, while categorical variables were displayed as frequencies and percentages. To compare groups, the χ2 test, Fisher's exact test, and Student's t-test were utilized based on the nature of the parameters. A significance level of P < .05 was used to determine statistical significance.
Results
Validation of Vietnamese BREAST-Q Version
The BREAST-Q Reconstruction scales were translated from English into Vietnamese under the oversight of the Q-Portfolio translation coordinator, following ISPOR best-practice guidelines for linguistic validation. The process included dual forward translation with reconciliation, single backward translation, expert review, cognitive interviews with 10 mastectomy patients (including 5 with reconstruction), and final proofreading to ensure conceptual equivalence and cultural relevance. The work was conducted by professional translation teams in Vietnam under the management of the first author at Ho Chi Minh City Oncology Hospital. (See Appendix 1 for the certificate issued on December 20, 2022).
Internal consistency was assessed using Cronbach's alpha on the detailed item scores within each of the 8 domains/subscales. A Cronbach's alpha 0.70 is generally considered acceptable for newly developed or translated instruments. The analysis demonstrated acceptable to good internal consistency across most domains, providing strong preliminary evidence that the items within each domain are highly coherent and measure their respective intended construct reliable. For the convergent validity, we tested the correlation between the patient's subjective satisfaction scores and an independent, objective measure of the surgical outcome the Aesthetic Score (A Score), assessed by the surgeon/clinical expert with the hypothesis “Domains measuring patient satisfaction with the outcome should correlate strongly and positively with the objective A Score.” The good statistically significant correlation (r = 0.912) between the total score of the relevant BREAST-Q domains and the objective A Score provides robust preliminary evidence of Convergent Validity, confirming that the Vietnamese tool successfully measures the same construct (surgical outcome quality) as assessed by clinical experts (as in Table 1).
Cronbach's Alpha for Each Domain and Convergent Validity (n = 20).

Demographics and Clinical Characteristics
Our cohort comprised 55 patients diagnosed with early-stage BC, exhibiting a mean age of 43.2 years and a mean BMI of 22.5 ± 2.8. The majority of cases were localized in the left breast (56.4%). Tumors size smaller than 3 cm with invasive carcinoma account for 81.8%. Cancer stages include 0, I, IIA, and IIB with 20.0%, 45.5%, 32.7% and 1.8%, respectively.
The majority of cases underwent axillary surgery, with 78.2% of patients undergoing lymph node biopsy, 7.3% undergoing lymph node dissection, and 14.5% undergoing both procedures. The prevalent types of skin incisions were Periareola (76.4%); Radial (10.9%); Inframmary fold (5.5%), and Superior periareolar (7.3%). The mean breast esthetic score at the 6-month was 8.0 ± 0.7. Post-operatively, 10% (n = 5) of patients reported complications including skin necrosis (n = 1), infection (n = 2), infection & skin necrosis (n = 1), and infection & visible implant (n = 1) (See Table 2).
Demographic and Surgical Details (n = 55).
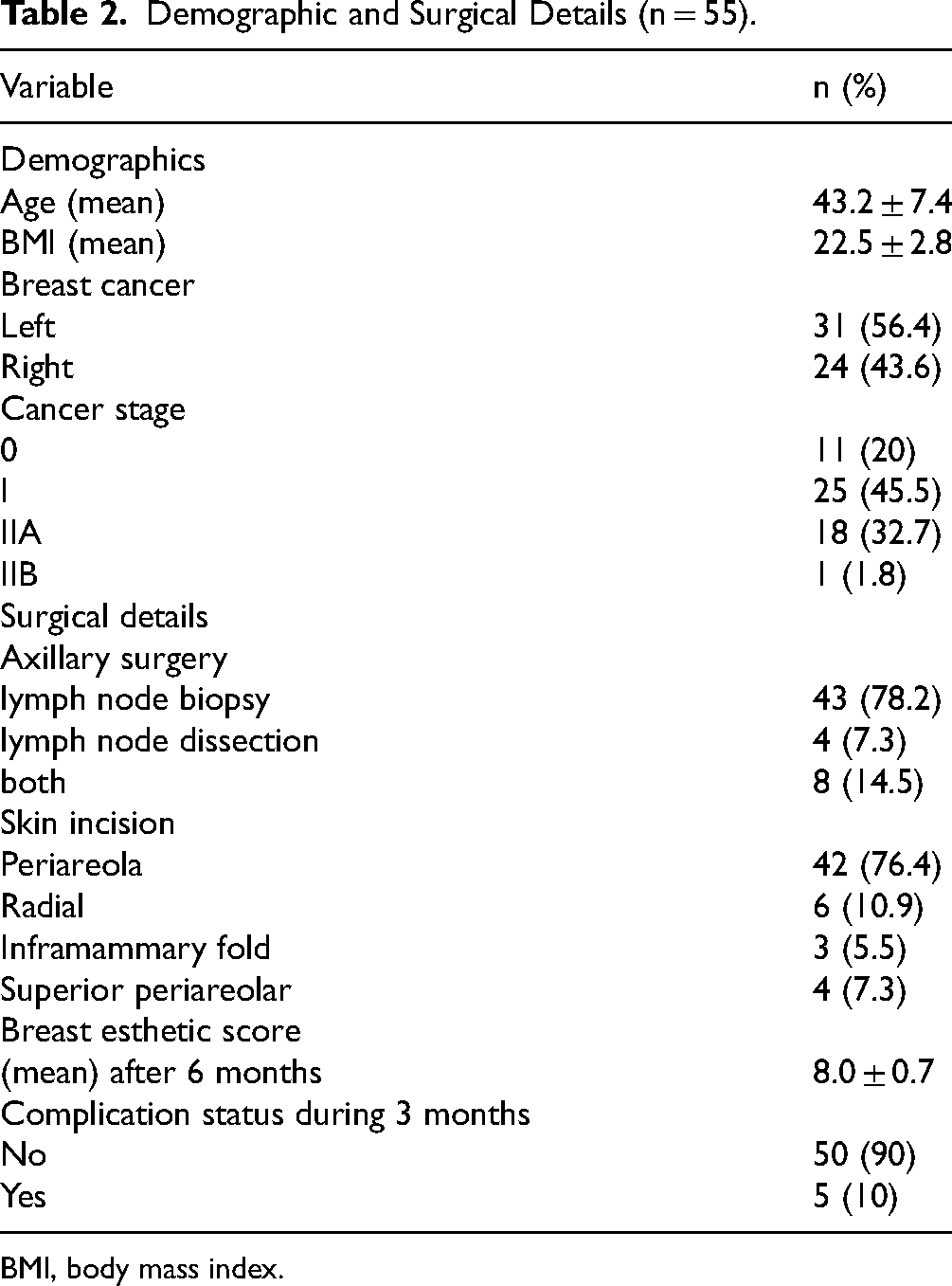
BMI, body mass index.
Patient Satisfaction Score Measured by BREAST-Q
The BREAST-Q scores (0-100 scale) demonstrated varied outcomes across different domains with intermediate scores in physical wellbeing-back & shoulder (62.3 ± 7.9) sex (63.2 ± 20.2) and psychology (73.9 ± 15.7), higher scores, reflecting better satisfaction in physical wellbeing- chest (84.5 ± 18.6), Pre-operative Satisfaction with Breast (81.9), and Post-operative Satisfaction with Breast (80.9), indicating strong psychological and surgical satisfaction outcomes. In contrast, the score comparison between pre- and post-operation showed a significant reduction in satisfaction scores regarding breast esthetics (mean pre-operative score: 75.9 ± 2.4; mean post-operative score: 65.8 ± 2.1; P < .001). These findings indicated that, on average, patients experienced a decline in satisfaction following surgical intervention relative to their pre-operative perceptions (See Table 3).
BREAST-Q Score of 8 Domains.

Factors Associated to Physical Wellbeing (n = 55)
The comparative analysis between high and low esthetic score patient groups reveals no statistically significant differences in physical and psychological scores following surgery. Notably, the scores pertaining to sexual function were higher in the low esthetic rating group (64.3 vs 59.3; P = .45), indicating that esthetic perceptions do not necessarily correlate with satisfaction in sexual life. The scores nearly equal between 2 groups including physical wellbeing-back and shoulders (62.1 vs 62.4; P = .291), physical wellbeing-chest (83.5 vs 84.7; P = .84), and psychology (74.4 vs 73.7; P = .90), suggesting that esthetic factors may have a limited impact on these outcomes.
The analysis of score differences between the two age groups (<40 and ≥40 years) indicates that most physical and psychological parameters do not demonstrate statistically significant differences, with the exception of the psychological factor. Specifically, average scores for the physical wellbeing-back and shoulders (60.5 vs 62.9; P = .37), physical wellbeing-chest (83.2 vs 84.8; P = .79), and sexual function (68.9 vs 61.5; P = .25) showed no significant discrepancies between the age groups. However, the psychological score was significantly higher in the patients aged ≥40 years (76.2 vs 66.3; P = .04), suggesting that older individuals may exhibit superior psychological adaptation following surgery or possess more realistic expectations regarding esthetic and functional outcomes (See Table 4).
Physical Wellbeing in Relation to Esthetic Score and Age Group.
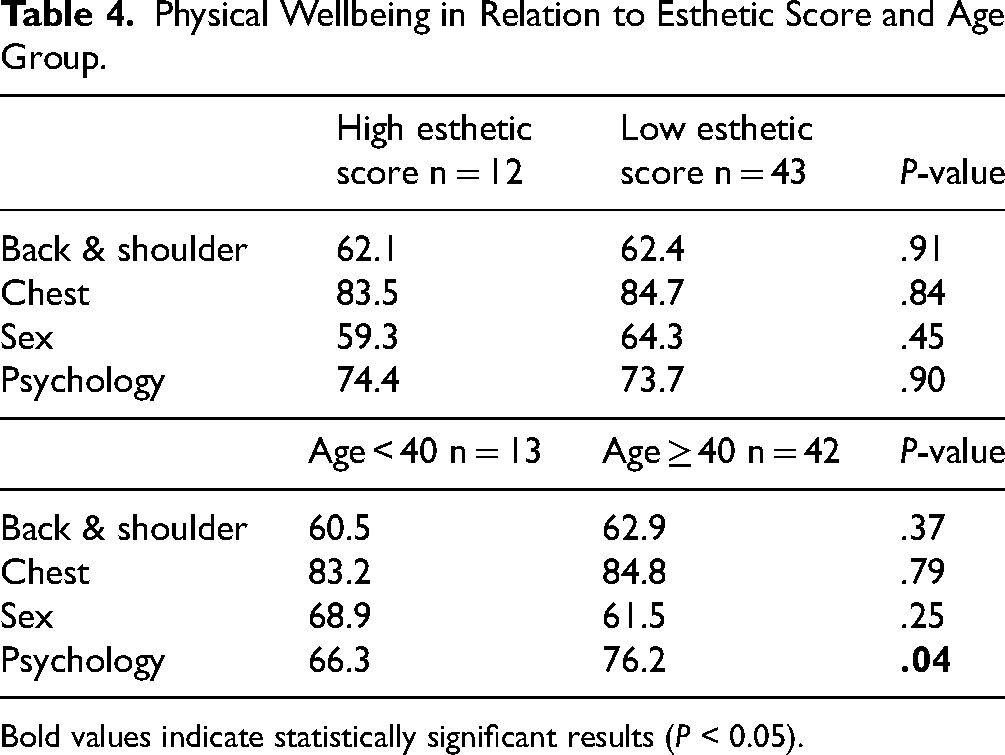
Bold values indicate statistically significant results (P < 0.05).
Factors Associated to Breast Satisfaction (n = 55)
An analysis of satisfaction scores regarding breast esthetics was conducted, stratified by esthetic score group after a period of 6 months, utilizing the GARBAY Scale. In the high esthetic score group (n = 12), no significant change was observed in satisfaction scores before and after surgery, with values recorded at 70.9 ± 4.9 and 67.3 ± 3.4, respectively (P = .15). These findings suggested that patients who achieved high esthetic outcomes maintained a stable level of satisfaction following surgical intervention. Conversely, in the low esthetic score group (n = 43), a significant reduction in satisfaction scores was noted, with scores decreasing from 77.4 ± 2.8 to 65.5 ± 2.5 (P < .0001). These results indicated that poor esthetic outcomes were associated with a substantial decrease in post-operative satisfaction, highlighting the importance of esthetic results in the overall patient experienced following surgery.
A stratified analysis of satisfaction scores concerning breast esthetics was performed, categorized by age group. In the group aged less than 40 years (n = 13), a significant decrease in satisfaction scores was observed, with scores declining from 70.3 ± 4.5 to 60.2 ± 4.4 (P = .003). Similarly, in the group aged 40 years and older (n = 42), a marked reduction in satisfaction scores was noted, with scores decreasing from 77.7 ± 2.8 to 67.6 ± 2.5 (P = .001). These findings indicated that both age groups experienced a statistically significant decline in satisfaction scores following surgery. This suggested that age is not the determining factor for diminished satisfaction.
A stratified analysis of satisfaction scores related to breast esthetics was conducted, focusing on two groups defined by the presence or absence of surgical complications. In the complication group (n = 7), a significant decrease in satisfaction scores was observed, with scores decreasing from 71.0 ± 6.5 to 58.4 ± 5.4 (P = .006). Conversely, in the no complication group (n = 48), a similar significant reduction in satisfaction scores was noted, with scores declining from 76.7 ± 2.6 to 66.9 ± 2.3 (P = .0001). These findings demonstrated that both groups, irrespective of the occurrence of complications, experienced a statistically significant decrease in satisfaction scores. This suggested that complications were not the sole determinants of reduced satisfaction (See Table 5).
Breast Satisfaction in Relation to Esthetic Score, Age Group, and Surgery Complications.

Bold values indicate statistically significant results (P < .05).
Discussion
Our Vietnamese BREAST-Q version 2 has the official certificate of translation from Q-Porfolio and the overall Cronbach's alpha of 0.70 and the good convergent validity with Pearson's correlation between the total score of the relevant BREAST-Q domains and the objective esthetics score (r = 0.912, P < .001). The analysis of BREAST-Q scores revealed significant variations in patient satisfaction following NSM and IBR. Positive outcomes were observed in Physical Wellbeing and Back & Shoulder Wellbeing, while elevated scores in Psychological Wellbeing and Surgery Satisfaction indicated strong psychological contentment. However, a notable decline in satisfaction regarding breast esthetics was observed post-operatively compared to pre-operative assessments, suggesting reduced satisfaction following surgery. Additionally, lower esthetic scores were associated with significantly decreased satisfaction, highlighting the critical importance of esthetic outcomes in the patient experience for early-stage BC treatment.
About tool validation, due to limited in number of patient with strict inclusion criteria, we could only perform a small sample size of the pilot study (N = 20), hence performing an exploratory factor analysis (EFA) or confirmatory factor analysis (CFA) is statistically inappropriate. However, the high internal consistency results strongly support the original 8-domain structure of the BREAST-Q. And the Test-retest reliability was not assessed in the pilot phase due to limitations in follow-up time for this initial pilot cohort. These barriers are considered as our study limitations. With the overall Cronbach's alpha of 0.70, our tool was accepted for using in our study cohort.
The average score for Physical Wellbeing-Back & Shoulder in a non-pathological population (79), closely correlating with the current study's result (62.3 ± 7.9), indicating that post-operative discomfort in this area does not exceed the reference standard. 4 Conversely, the score for Physical Wellbeing-Chest (84.5 ± 18.6) was significantly higher than the Mundy's result of 93, suggesting substantial discomfort in the chest region post-surgery. 16 In contrast, scores for Psychosocial Wellbeing (73.9 ± 15.7), Sexual Wellbeing (63.2 ± 20.2), and Satisfaction with Breast post-operatively (81.9 ± 14.2) surpassed published reference values, 17 indicating marked improvements in psychological and sexual satisfaction. The Surgery Satisfaction score (75.9 ± 18.2) also reflected a high level of satisfaction with the surgical intervention. Although no benchmark data exists for breast animation deformity, this measure has shown high reliability (Cronbach alpha ≈ 0.92). 18 These findings demonstrate that despite ongoing physical discomfort, particularly in the chest, patients experience a significant enhancement in subjective QoL following the intervention.
In our study, the analysis of two patient groups categorized by esthetic ratings (high and low) showed no statistically significant differences in physical and psychological post-surgery scores. This suggests that esthetic evaluations may not adequately reflect satisfaction in sexual life or psychological status, consistent with the observations of Etlahir. 19 In contrast, previous studies employing the BREAST-Q, such as the work of Choi reported a moderate correlation between expert esthetic ratings and various patient satisfaction metrics, including satisfaction with breast appearance, psychosocial wellbeing, and sexual wellbeing. Their reported Spearman correlation coefficients ranged from 0.24 to 0.29 (P < .05), indicating a notable yet imperfect relationship. 20 Additionally, Luong et al found that after breast augmentation, patients experienced significant increases in satisfaction with breasts, psychosocial wellbeing, and sexual wellbeing compared to their pre-surgery assessments. They also reported that physical wellbeing (specifically related to the chest) tended to decline, but this did not negatively impact overall patient satisfaction. 21 Thus, while our results align with some findings from earlier studies by highlighting that esthetic ratings do not exclusively determine satisfaction, they also suggest differing dynamics regarding patient-reported outcomes. Particularly, the lack of significant differences in our study indicates that individual perceptions and psychological factors may play a more crucial role in shaping experiences post-surgery.
In our study, the comparison of scores between the two age groups indicates that the majority of physical and psychological wellbeing aspects do not demonstrate statistically significant differences. Specifically, the mean score for the Back & Shoulder region was 23.8 for the older group compared to 22.3 for the younger group (P = .81), the Physical Wellbeing-Chest score was 32.3 versus 30.9 (P = .83), and the Sexual Wellbeing score was 68.9 compared to 61.5 (P = .25). However, the Psychosocial Wellbeing score in patients aged ≥40 years (76.2) was significantly higher than that of the younger cohort (66.3; P = .04). Similar to Kim's analysis, older age exhibits positively associated with psychosocial wellbeing. 22
In this study, patient satisfaction scores regarding breast esthetics significantly decreased post-operatively compared to pre-operatively (mean pre-operative score: 75.9 ± 2.4; post-operative score: 65.8 ± 2.1; P < .001). This finding suggests that patients generally felt less satisfied with their breast area following the intervention. These results are at odds with the majority of previous studies utilizing the BREAST-Q scale. According to Pusic—the developers of BREAST-Q—and subsequent research by Mundy, breast satisfaction scores typically increase or remain stable following surgical procedures, particularly among groups undergoing breast reconstruction or tissue-sparing techniques.4,16 In earlier studies, when techniques for breast surgery and reconstruction were relatively novel, patients might have had lower baseline expectations and were more likely to experience satisfaction due to the innovative nature of these procedures. As these techniques have become more common, it is plausible that patient expectations have similarly evolved. Today's patients are often more informed and have higher standards regarding esthetic outcomes, which may contribute to their perception of satisfaction. Thus, while previous research indicated increased satisfaction levels, the contemporary landscape reflects a shift where patients seek not only functional improvements but also optimal esthetic results. As surgical techniques advance and patient awareness of options expands, healthcare providers must adapt to these changing expectations, ensuring comprehensive discussions regarding anticipated outcomes and potential post-operative satisfaction.
Study Limitations
Our study provides the first comprehensive assessment of patient satisfaction after NSM and IBR using the Vietnamese BREAST-Q, demonstrating strong preliminary psychometric performance and clinically meaningful insights. However, the small sample size limited statistical power and restricted full psychometric validation, preventing EFA/CFA and test-retest assessment, while the single-center design may reduce generalizability. Future multi-center studies with larger cohorts and complete validation procedures are needed to confirm scale stability and strengthen the evidence for broader clinical application.
Conclusion
Our study highlights the BREAST-Q Vietnamese version as a crucial tool for assessing patient-reported outcomes following breast surgery and it is primarily validated with Cronbach's alpha and good convergent validity with an objective clinical measure. Our study highlights the BREAST-Q Vietnamese version as a crucial tool for assessing patient-reported outcomes following breast surgery. Its application can enhance understanding of patient satisfaction and QoL in Vietnamese populations by capturing both esthetic perceptions and psychological wellbeing. Future use of this instrument will aid clinicians in tailoring care to better meet patient expectations and improve overall healthcare practices in BC management. By integrating the BREAST-Q Vietnamese version into clinical and research settings, we could foster a patient-centered approach that prioritizes physical and emotional wellbeing post-surgery.
Footnotes
Acknowledgments
The authors would like to thank all individuals and organizations who supported this study.
Author Contributions
DTB contributed to conceptualization, methodology, data curation, manuscript revision, formal analysis, writing – original draft preparation and final version. HNV contributed to methodology, data curation, and manuscript revision. TCT contributed to conceptualization, manuscript revision, and formal analysis. XDP contributed to conceptualization, methodology, and manuscript revision. VQL contributed to conceptualization, methodology, and manuscript revision. All authors gave their final approval and agree to be accountable for all aspects of the work.
Ethical Approval
The study was approved by Hanoi University of Medicine Ethics Committee in Biomedical Research approved with Decision No. 671/GCN-HDDDNCYSH-DHYHN dated June fourth, 2022, and all study participants provided informed consents.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Appendix: Q-Porfolio's certificate.