
Abstract
Understanding denture patient experiences is vital for improving care outcomes. This research explored the lived experiences of patients undergoing rehabilitation with removable complete dentures, a topic often overlooked in qualitative oral healthcare research. Using a constructivist grounded theory approach, 25 adults treated through the public health service in Tasmania's Southern Dental Clinic between 2017 and 2022 were interviewed to gain insight into their journeys. Semistructured, face-to-face interviews were recorded, transcribed, and analyzed using NVivo 12, following a structured coding and memoing process. The study uncovered a 4-phase progression: journeying to the unknown (confronting unfamiliar experiences), transitioning to knowing (developing understanding), deciding on the known (making informed choices), and living in the known (applying gained knowledge). These phases form the foundation of the substantive theory renormalizing the disrupted, which illustrates how patients continuously move between disruption and efforts to restore normalcy. This theory challenges the traditional view that denture rehabilitation ends with denture placement. It calls for interdisciplinary, person-centered support to address the emotional, psychological, and practical challenges patients face, ultimately improving long-term outcomes for those living with complete dentures.
Introduction
Understanding patient experience is increasingly recognized as a vital component for improving health outcomes, encompassing factors such as patient satisfaction, quality of life, treatment adherence, and rapport with healthcare professionals. 1 Historically, healthcare quality has been assessed primarily through clinical effectiveness and patient safety, often overlooking the experiential dimension of care.2,3 However, studies have shown that exploring patient experience can provide critical insight into care quality, enabling healthcare providers to identify and improve care components such as poor communication, limited accessibility, and emotional distress.4,5
In oral healthcare, patient experience has typically been measured through patient satisfaction and oral health-related quality of life, with a strong emphasis on functional and aesthetic outcomes.6,7 Rehabilitation in this context aims to restore function, enhance appearance, and improve overall oral health, thereby contributing to greater holistic well-being. 8 Clinical outcomes such as chewing efficiency, facial aesthetics, and smile satisfaction, along with systemic conditions like heart disease and diabetes, all influence rehabilitation and post-treatment quality of life. 9 Further oral health outcomes have been shown to have a profound effect on self-esteem and activities of daily living, yet are generally only assessed through quantitative, score-based methods that may oversimplify the patient journey. 10 Therefore, there is a need for qualitative approaches to capture the psychological, social, and emotional complexity of patient experiences often missed by other methods. Recent research has highlighted the physical, psychological, social, and affective responses that patients experience throughout oral health treatment. 11 Oral healthcare should consider environmental influences, such as family support and community context, in addition to individual health conditions. 12 These factors are particularly significant in removable complete denture rehabilitation, where challenges such as poor retention, chewing difficulties, speech issues, discomfort, and aesthetic dissatisfaction are frequently reported.13,14
Previous research suggests that experience with removable complete denture rehabilitation can be positive11,15 or negative. 11 In one study, denture wearers report increased comfort while swallowing, improved speech confidence, better aesthetics, reduced gum sensitivity, and easier chewing thus suggesting that patient experience is highly variable and deeply personal. 15 Variation in experience can be shaped by individual expectation, the path to edentulism, and the extent to which patients are prepared emotionally and clinically for life with dentures. 16
It is important to understand the experiences of patients who undergo rehabilitation with removable complete dentures to improve care through empathetic, person-centered clinical practices and enhanced patient support. We aim to co-construct a theory based on the influence of social and psychological processes that reflects patient experience, while making meaning of the perspectives and views of oral health patients. This study, therefore, addresses a gap in current literature and will provide valuable insight for future professional practice and policy in oral health.
Methods
To meet the explorative aim for this qualitative study, a constructivist grounded theory (CGT) approach was utilized. Unlike classical grounded theory, which treats a researcher as a passive observer, CGT positions a researcher as an active participant in meaning-making. This study is inherently tied to ontological and epistemological considerations, particularly within CGT, suggesting that multiple social realities exist, and that knowledge is co-constructed between researchers and participants. In this study patients’ experiences with denture rehabilitation are shaped by their personal, social, and historical contexts. By adopting a qualitative, interpretive stance, this research acknowledges that patient experiences cannot be understood through rigid methodologies but require an openness to dialogue, critique, and contextual analysis. 17
This study was approved by Tasmanian Human Research Ethics Committee (reference no. H0018568). All participants provided written and verbal informed consent prior to enrolment and at the commencement of the interview respectively in the study.
Sampling Strategy
Purposive sampling was used to recruit 25 adult participants (over 18 years of age) who had received treatment with removable complete dentures between 2017 and 2022 in Tasmania's Southern Dental Center. This approach ensured that the selected participants had relevant experience and insight into the most current denture rehabilitation process.
Setting
Public oral health services in Tasmania are delivered through major dental clinics, including the Southern Dental Centre in New Town. Eligibility for these services requires patients to hold a Pensioner Concession Card or a Health Care Card, granting access to government-funded dental care. All participants in this study received their treatment at the Southern Dental Centre in New Town, Hobart.
Data Collection
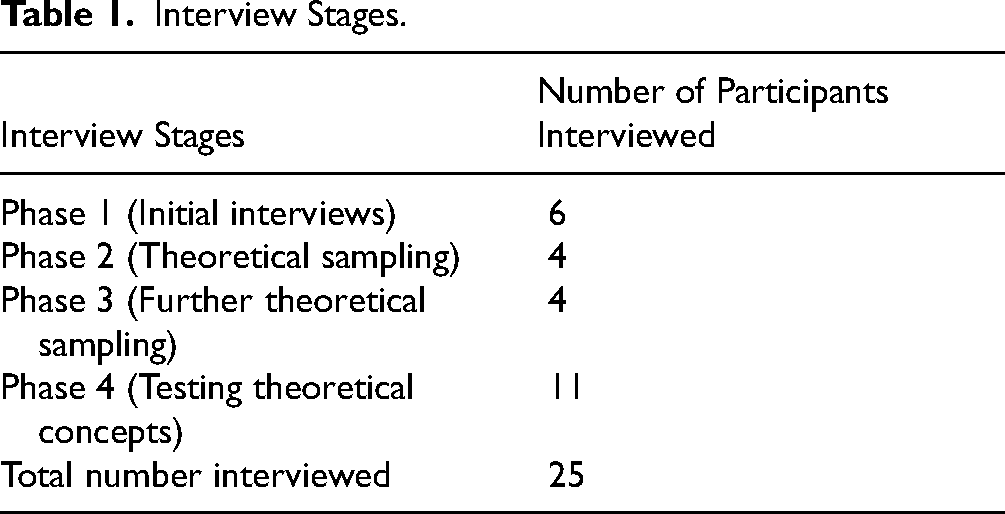
Face-to-face, semistructured interviews captured participants lived experiences with removable complete dentures, focusing on their perspectives during rehabilitation. Interviews were audio-recorded and transcribed verbatim for analysis. The interviews took place during 4 phases (Table 1). Theoretical sampling guided the interview process, allowing for continuous refinement of emerging categories. This approach uses an iterative process of ongoing comparison within and among data sets, researcher field notes, and memos.18,19 Data collection continued until theoretical sufficiency was achieved. Theoretical sufficiency was defined as repetition of codes and lack of emerging categories where data was collected until concepts reached a stable and comprehensive level. Theoretical sampling and memo writing were employed throughout data collection to refine categories and achieve theoretical sufficiency.
Interview Stages.
Data Analysis
Interview transcripts were coded using NVivo version 12 software, allowing for easy sifting, sorting, and discovering of relations between categories. Consistent with a CGT approach, data collection, coding, and analysis took place concurrently. Coding and memoing were utilized including line-by-line initial, focused, and theoretical coding. Following the guidelines of Charmaz, the analysis began after the initial interview, linking coding to theory development. The researchers adhered to coding principles which progressed through 3 phases: initial, focused, and theoretical coding, aimed at forming theoretical concepts. Researchers used coding phases, memo writing, and constant comparison to refine and test concepts.
Reflexive Statement
There is an acknowledgment of the reciprocal dynamic between researcher (a dental prosthetist) and participants (patients) in this study, aligning with constructivist principles. This interaction is fundamental to understanding the social and psychological issues arising from tooth loss and denture-wearing experiences. There is respect of boundaries within this relationship, particularly the personal nature of denture use, as some participants may be reluctant to discuss their experiences in unfamiliar settings. To honor these boundaries, privacy was ensured, fostering a research environment conducive to open discussions. This methodology was selected to co-construct meaning and knowledge with participants, ensuring their perspectives shaped the findings. It facilitated an iterative constant comparison process, allowing data to be revisited for deeper analysis. Purposive sampling was continually guided by emerging data, making participant selection dynamic. Rooted in postmodernist and interpretivist philosophies, the approach aligned with internal perspectives on meaning-making and enabled a structured coding process emphasizing theoretical sensitivity. This allowed new concepts to emerge without relying on preconceptions.
Results
The rehabilitation of edentulous participants with removable complete dentures was an intertwining of different experiences taking place from the commencement of tooth loss to living with removable complete dentures after the rehabilitation process. The findings showed that rehabilitation experiences involved progressing through 4 phases situated in 2 key domains: (disrupted and renormalizing) and constitute the renormalizing the disrupted substantive theory (Figure 1).

Renormalizing the disrupted theory.
Domain 1: Disrupted
Disrupted refers to the significant physical, psychological, behavioral, and socioeconomic disturbances and challenges triggered by tooth loss and rehabilitation with removable complete dentures. These disruptions altered the natural oral state and were present throughout the 4 phases “Journeying to unknown,” “Transitioning to knowing,” “Deciding on the known,” and “Living in the known” illustrating the persistent impact of disruption across the entire denture rehabilitation journey. This has been depicted in Figure 1.
Journeying to Unknown
Characterized by unfamiliar and abrupt and surprising occurrences, disruption was marked by anticipating and experiencing tooth loss which triggered strong emotional reactions grief, fear, and anxiety as participants confronted both physical change and uncertainty as expressed here, I walked in, not really knowing what was going to happen. I was a bit thrown away; I didn’t know what to expect. But when I went in there, and they told me I needed my teeth out, I said, yes, that all right. So, they took them out. (P20)
Disruption was further influenced by factors such as excessive sugar consumption, unaffordable dental care, untreated water, and delays in seeking dental help due to phobia. This disruption peaked when participants “succumbed” to edentulism undergoing multiple extractions or complete clearance in one sitting caused by neglected oral hygiene, drug use, or infection. For example, “I had a pretty drug habit for a lot of years. That ruined my teeth. But that was, yes, 20-odd years ago. But you can’t fix them after that to be honest, once they were damaged” (P15).
Transitioning to Knowing
Participants began actively acknowledging the impacts of tooth loss. They sought information, developed coping strategies, and experienced heightened anxiety. This period signified a shift to a new “self,” marked by changes in identity, feelings of regret, and emotional responses associated with loss. Captured by one participant, “It impacted my health, my wellbeing, my mental health, my emotional health… it had changed me in a big way that I didn’t see coming” (P7).
Disruption extended to function—eating, speaking, and oral care. Participants struggled with certain foods and faced embarrassment from speech difficulties, social withdrawal, and the loss of a smile, affecting confidence and self-image due to loss of all the teeth as expressed here, “I’d get in the stage of even covering my mouth while talking or being afraid to smile… especially in photos” (P15).
Deciding on the Known
Disruptions in this phase stems from making decisions about oral health and denture use based on the reality understood. Disruption remained evident in how they responded to both the condition of edentulism and the realities of removable complete denture rehabilitation—particularly following their initial denture fitting. Some participants expressed aesthetic dissatisfaction with their new dentures, describing them in animalistic terms, a phenomenon of “animalizing” to highlight the psychological struggle with appearance; “And I felt, in the beginning, like I looked like Bugs Bunny” (P14).
Disruption extended to social interaction. Despite a desire to stay connected, many participants felt uncomfortable dining out or attending gatherings due to altered facial appearance or fear of judgment. The physical signs of edentulism, like sunken cheeks, provoked self-consciousness and led some to isolate themselves socially. “Because I don’t want everyone to know that I’ve got false teeth… If they ask me, have I got false teeth I’m going to say no” (P4). The stigma surrounding dentures also disrupted participants’ confidence in personal and romantic relationships. Edentulism and denture use became barriers to dating, with participants fearing rejection or embarrassment. For example, “And another thing, like, I'm single. So, there's no way I was going to go out and pick up, or find anyone, a relationship or anything like that the way I was” (P15).
Participants also encountered disruption through internalized and societal perceptions of dentures as a sign of old age. For younger and middle-aged individuals, this created emotional dissonance and stigma, complicating the adjustment process. The mismatch between their age and the societal image of denture users undermined their self-esteem as explained here, “When I didn't have as many teeth, and they were getting taken out, I was just a bit ashamed, because I didn't think I was old enough to have dentures” (P24).
Living in the Known
Disruptions were marked by ongoing challenges which included difficulties with eating, chronic pain, speech impediments, denture looseness, and the sensation of bulkiness. Eating specific foods such as steak or apples was viewed as a benchmark of rehabilitation success. Participants who couldn’t manage these foods experienced frustration and felt their adjustment was incomplete. Many had to modify their diets, avoid hard-to-chew items, and in some cases experienced weight loss, which added to the stress of adapting. “I can’t eat an apple because I don’t have the biting power or the chewing power like you do. If I had an apple, I’d have to cut it up. I don’t have steak because I can’t chew properly” (P16). Further, denture-related anomalies contributed significantly to lifestyle disruption. These issues demanded constant vigilance during meals, making participants feel vulnerable and requiring them to be more selective and cautious with food. To manage pain, participants often relied on self-care remedies or sought frequent adjustments from clinicians to alleviate discomfort. I took Disprin if it was painful. I took them out and rinsed with saltwater and did all that. (P11)
Domain 2: Renormalizing
Renormalizing involves adjusting expectations, attitudes, and behaviors post-rehabilitation. It encompasses the phases of transitioning to knowing, deciding on the known (making informed decisions), and living in the known (drawing on experience). Many participants actively sought professional support and made informed choices to better adapt to life with dentures. Rebuilding confidence and accepting their circumstances helped participants with renormalizing.
Transitioning to Knowing
Soon after losing their final teeth, most participants became aware of a familial pattern of tooth loss and denture use, commonly involving parents, siblings, grandparents, and in some cases spanning several generations. Recognizing these shared experiences supported participants’ renormalization, as it reduced feelings of isolation and framed denture wearing as a familiar and shared life experience rather than an individual failure. As 1 participant reflected, “My sister is going through the same thing (tooth extracted and subsequent denture wearing). And Mum had dentures from an early age because that's just what they did” (P7).
Deciding on the Known
Deciding on the known was grounded in participants’ deliberate choice to act on their circumstances often enabled by a willingness to seek and accept professional support, which helped them adjust to substantial changes in their oral health. Through this process, participants began to rebuild confidence and re-establish stability in everyday life. Central to this transition was the medicalization of dentures, whereby dentures were understood not merely as replacements for teeth but as therapeutic interventions that alleviated wider health concerns, including infection, pain, and weight-related issues, as was noted that through treatment using dentures, “It was just the pain would have been taken away” (P15).
Acceptance of dentures was frequently described as psychologically challenging, leading participants to advocate for short-term therapeutic support to assist with emotional adjustment. This reflected an awareness that psychological resilience was as important as physical adaptation. Their views were underpinned by recognition that dentures had become part of their “new normal,” as illustrated by the statements, “(I suggest using) short-term therapy when you’re not coping very well” (P9), and “I accept the fact that I’ve got to have dentures, absolutely, 100%” (P20).
Additionally, social reintegration marked a significant aspect of renormalizing. Participants sought to overcome stigma and re-establish social, family, and professional relationships. This return to everyday social engagement was seen as a powerful sign of regained confidence and personal transformation because, “It makes you feel more comfortable in your own skin… I crack a joke or whatever… then not be like (covering mouth) … I'd be like (grinning showing full set of teeth)” (P23).
Living in the Known
Living in the known is marked by participants integrating dentures into their daily lives, gradually developing habits to accommodate denture use. Participants thrived managing disruptions through practical strategies. Participants engaged in activities like speech exercises and food preparation modifications to which enabled some to function in social settings. For example, when asked about their new eating habits, 1 participant suggested “So, chop (the food) up really small before you eat it, and still, it's a learning process of learning to eat again” (P14). For those who gained some confidence in eating, speaking, and smiling, this led to an improved self-image and increased personal resilience, and had great praise for dentures noted here. “Yes, they look 100% better on what my teeth did, so it's always been a good thing. It's never been, I’ve got these shitty dentures” (P15).
A key component demonstrating renormalizing was normalizing and positivizing denture use in which participants had to reframe their perspective, to no longer seeing dentures as signs of aging or decline but as functional solutions to restore oral function. This shift allowed them to embrace denture use without shame, adopting a more confident and affirmative mindset as “The people that I have around me now, all my family and all of their friends know I've got dentures… I'm not overly fussed” (P10).
Finally, renormalizing was demonstrated by the effort being made by participants to break generational trends of poor oral health in families and communities through an expressed desire to educate younger family members about dental care, encouraging prevention over neglect. “I’ve always tried to get my children to look after their teeth… And my grandkids, I’m always on to them about their teeth” (P13).
Discussion
Theoretical Contributions
The study developed the theory “renormalizing the disrupted,” offering a framework to understand patients’ experiences of tooth loss and denture rehabilitation across 2 domains: disrupted (impacts) and renormalizing (restoring normalcy), addressing a key gap in oral health literature (physically, psychologically, emotionally, and socially). This theory has been developed through a CGT approach focusing on the social process of denture rehabilitation. It has become clear that this social process involved a series of events that are related to one another. 20 By explicating the elements of the denture rehabilitation process this study has been able to explain phenomena under investigation. 21 Through advance abstractions the explanatory power of the theory “renormalizing the disrupted” was enhanced 20 contributing to a new and deep understanding of denture rehabilitation.
The theory demonstrates similarities with Bury biographical disruption model, where chronic illness disrupts life and identity. The similarities between renormalizing the disrupted theory and Bury's 22 concept of biographical disruption are reflected across 4 key areas. First, both theories emphasize identity transformation, with Bury referring to the “shocking awareness of the break between the past and the future,” 23 a notion echoed in the current study through some experiences described in journeying to unknown and transitioning to knowing phases. Second, both recognize changes in social relationships. Bury observed altered social ties and the importance of social support, 24 which parallels the study's focus on learning relationally, responding to socialization demands, and breaking the trend. Third, both theories detail a process of adaptation, with Bury discussing regaining meaning and function, 24 while the current theory addresses adaptation through such categories as medicalizing dentures and reframing self for instance. Renormalizing the disrupted theory differs from Bury's model in that it is situated specifically within the context of edentulism and denture adaptation, offering a focused and experiential understanding of disruption and renormalizing. Another difference is that it delineates 4 interconnected phases, which provides a structured framework that assists clinicians in recognizing and addressing patients’ support needs throughout the rehabilitation process specific for individuals in this context.
This study found that alongside coping and adjustment, participants actively engaged in strategies of normalizing and positivizing to embrace life with dentures. Despite functional and aesthetic anomalies, many emphasized their strengths, collaborated with practitioners, or independently managed challenges. These behaviors countered social stigma and reframed denture use as empowerment rather than disability. This aligns with previous research25,26 that underscores the power of narrative reconstruction and positive reinterpretation in managing life disruptions. Normalizing involved regaining confidence in public and relational spaces, reconstructing body image, and fostering emotional resilience. Svinhufvud et al 25 describe similar identity reconstructions following oral changes, while Xanidis and Gumley 26 highlight self-compassion and mindfulness as critical tools for managing discomfort and stigma. The findings of this study provide deeper meaning through the lens of Goffman's seminal work 27 in which people protect themselves when they depart from socially approved appearances. It includes learning experiences concerning managing relationships with the nonstigmatized in variety of personal and social situations and this is observed within the theory renormalizing the disrupted. Moreover, parallels can be drawn with Charmaz and Rosenfeld's work, 28 who articulate that the experienced body becomes a looking glass through which the person gains and interprets images of self. The looking glass body forces reflexivity about self and situation, which led in the study to the concept of normalization.
Practical Implications
Importantly, while patients often regained a degree of normalcy through improved appearance and function participants continued facing persistent difficulties, consistent with previous research. 29 These included chewing problems, speech issues, looseness of dentures, gum chronic irritation, and emotional struggles, even post-rehabilitation. Similar ongoing disruptions were found in other studies30,31 emphasizing that denture provision does not mean end of intervention. Participants often saw dentures as a symbol of decline, reinforcing negative self-perceptions and delaying treatment-seeking. This aligns with previous findings 29 and illustrates the emotional burden of denture use. Participants also reported ongoing psychological, emotional, and physical challenges, including anxiety and social withdrawal, as seen in previous work.32,33 This demonstrates that long-term support is essential.
In light of these complex experiences, this study advocates for patient-centered care models that extend beyond the technical aspects of denture provision. Clinical care should be paired with psychological support, social reintegration strategies, and clear communication to improve adaptation and outcomes. Mindfulness-based interventions34,35 and therapies such as acceptance and commitment therapy and cognitive behavioral therapy36,37 are recommended to help patients navigate the psychological demands of wearing dentures.
Some participants saw dentures as therapeutic devices that relieved pain and aesthetic anxiety. This holistic view may boost patient engagement, reduce stigma, aid adjustment, and support broader public health integration and funding. Overall, it highlights dentures’ wider therapeutic value a perception supported by Ceraulo et al. 38
Additionally, the study stresses the importance of collaborative, interdisciplinary care, involving professionals like psychologists, dietitians, and speech therapists to meet diverse patient needs. Interventions such as mindfulness 39 and cognitive behavior therapy 40 have previously been linked to more positive outcomes in oral healthcare. Strong clinician–patient communication and shared decision-making41,42 are also essential for setting realistic expectations and enhancing treatment adherence. Further research could focus on the value of pretreatment including psychological counseling, stigma reduction interventions, and early interdisciplinary collaboration.
Dietary concerns emerged as a significant ongoing challenge for denture wearers, consistent with previous studies,43,44 prompting a recommendation to integrate nutritional counseling into denture care to address these functional difficulties holistically. In addition, the study underscores the importance of early oral health education within families as a preventive measure against future tooth loss. Supported by previous work45–47 the findings advocate for family-centered oral health programs and community outreach initiatives as essential strategies for instilling lifelong preventive habits and ultimately reducing long-term reliance on dentures.
Strengths of the Study
This study used a CGT approach to explore the experiences of patients with removable complete dentures, resulting in the theory renormalizing the disrupted. It offers novel insights into denture rehabilitation and contributes significantly to oral health research and patient-centered care through flexible, in-depth interpretation.
Limitations of the Study
The study was limited to English-speaking, public-sector volunteers. This population may not reflect private care or non-English speakers and may not be generalizable to these settings. However, this study provides valuable insights applicable to similar clinical and cultural areas and may be adapted for other settings. Further, we recognize that bias may be present in this study in the form of sampling bias and interviewer bias, despite best efforts to reduce this.
Conclusions
This study contributes significantly to understanding the lived experiences of individuals undergoing rehabilitation with removable complete dentures by developing the grounded theory renormalizing the disrupted. Employing a CGT approach, it identifies interconnected phases reflecting varying levels of disruption and adaptation. The use of a CGT approach has resulted in new theoretical contributions in the field of oral health, providing a solid foundation for further research.
This novel theory reframes denture rehabilitation as a lifelong process requiring continuous support. It advocates for systemic changes in oral healthcare to provide improved patient experience. Oral healthcare providers should consider their patients’ care across different phases of treatment and rehabilitation and aim to understand the disruption and renormalizing processes. Opportunities to employ the principles of this theory include better professional education, organizational person-centered care models, and long-term support, to improve outcomes and quality of life for denture wearers.
Footnotes
Acknowledgments
We would like to express our gratitude to Dr Ioan Jones, Clinical Director of Oral Health Services Tasmania, Department of Health, as well as the participants for their time and effort in agreeing to be interviewed for this study. Additionally, various software tools were used throughout the research process, including NVivo 12 for data analysis, Endnote for managing references, ChatGPT for paraphrasing and spell-checking, and Perplex A1 for generating and validating references.
Author Contributions
Conceptualization: SC, PJvD, SJP, and SP; literature searching: SC; writing initial draft: SC; writing—review and editing: SC, SJP, PJvD, and SP; supervision: SJP, PJvD, and SP. All authors have reviewed and approved the last version of the manuscript.
Data Availability
Data was not made available due strict organizational privacy policy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval to report this research study was obtained from Tasmanian Human Research Ethics Committee (reference no. H0018568).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Both written and verbal informed consent were obtained, with written consent provided before data collection and verbal consent confirmed at the beginning of each interview.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Tasmanian Human Research and Ethics committee.