
Abstract
This study investigates factors influencing women's childbirth experiences, aligning with World Health Organization guidelines emphasizing the importance of a positive pregnancy and childbirth journey. Conducted at the RigaMaternity Hospital between June 2022 and February 2024, the research included 133 women who completed 2 postpartum questionnaires—the short version of the Quality from the Patient's Perspective at discharge, and the Childbirth Experience Questionnaire (CEQ) 4 weeks later. Key findings emerged from the CEQ analysis. The contract either midwife or doctor was the main factor for higher satisfaction with labor across all CEQ domains. Unplanned medical interventions such as episiotomy were associated with lower scores in the domains “Own capacity” and “Perceived safety.” In contrast, patients who experienced a spontaneous perineal tear reported significantly more positive answers on “Own capacity” and “Participation” scales. A moderate negative correlation was observed between postpartum blood loss and “Own capacity” (ρ = −0.331, P < .001). These findings highlight the central role of communication, individualized care, and minimized medical intervention in shaping women's childbirth experiences, underscoring the need for supportive and respectful maternity care practices.
Introduction
Recent changes in maternity care emphasize women's experiences and well-being, rather than focusing solely on morbidity and mortality. The World Health Organization highlights the importance of ensuring positive pregnancy and childbirth experiences.1,2 Factors such as personal values, clinical variables, and pre-existing conditions can significantly influence these experiences. 3 Traumatic births, in turn, may affect future family planning, increase psychiatric issues, and lead to requests for elective cesarean section.4–7
Several questionnaires have been developed to evaluate satisfaction with labor and birth, the outcome of experience, and the quality of care.8–11
The aim of this study was to assess factors influencing the childbirth experience of primiparous women in Latvia. The short version of Quality from the Patient's Perspective (s-QPP) was used which evaluates aspects such as nutrition, privacy, equipment, information provided, and pain management. 12 The Childbirth Experience Questionnaire (CEQ) was also selected, as it offers a valid scoring system, is comprehensive, and specifically explores first-time mothers’ perceptions of their birth experience. 13
Method
The single-center, prospective, observational, cohort study was conducted at the Riga Maternity Hospital, a secondary-level monodisciplinary perinatal care facility in Latvia. During the study, the birth rate declined from 20 000 to 21 000 to 12 000 to 14 000 births per year in Latvia. The decision to include 150 participants was based on the limited study population: healthy nulliparous women undergoing labor induction without any systemic diseases or pregnancy complications. We considered 150 participants feasible and sufficient for meaningful exploratory analysis. Women participated in the postnatal questionnaire study between June 2022 and February 2024. All patients gave their informed consent.
Inclusion criteria were primipara, singleton pregnancy, cephalic presentation, gestational age ≥37 weeks, Bishop scale score ≤6, intact membranes, and induction of labor (IOL). Exclusion criteria were age <18, inability to read and understand the informed consent, systemic comorbidities, and pregnancy complications.
The IOL was performed according to the hospital protocol, using a combined method: Foley catheter (up to 60 mL of saline), transcervical, for 12 h or until spontaneous expulsion, plus misoprostol perorally 25 μg every 2 h until regular uterine contractions or catheter removal, followed by amniotomy.
This study was designed to test the hypothesis that immediate postpartum assessments (s-QPP) primarily reflect satisfaction with the tangible aspects of care, whereas the 1-month assessment (CEQ) captures a more comprehensive psycho-emotional experience. This approach might reveal a decline in satisfaction over time, as initial positive feelings fade and more critical reflections emerge.
The s-QPP is a condensed version of the original Quality from the Patient's Perspective (QPP) questionnaire, developed in 2002, and is grounded in a theoretical model based on patients’ conceptions of care quality.12,14 The s-QPP explores 4 core dimensions: medical–technical competence, physical–technical conditions, identity orientation, and the sociocultural atmosphere. Each item is assessed in terms of perceived reality (“this is what I experienced”) and subjective importance (“this is how important it was to me”), using 4-point Likert scale: 1 = totally disagree, 2 = mostly disagree, 3 = mostly agree, 4 = totally agree. The short form has demonstrated acceptable reliability and validity and is recommended for clinical use, particularly in contexts where patient fatigue or time constraints may limit response to longer instruments.12,14
The CEQ was developed in 2010 and was specifically designed for administration approximately 1 month postpartum, a period when experiences remain vivid but emotional processing has begun. 13 It has been translated and validated in several languages, including English, 15 Spanish, 16 Danish, 17 etc. The CEQ consists of 22 items grouped into 4 empirically derived domains: own capacity (eg, sense of control and pain management), professional support (eg, midwifery care and communication), perceived safety (eg, feelings of security and birth-related memories), and participation (eg, involvement in decision-making). Items are rated on a 4-point Likert scale, along with additional visual analog scale assessing labor pain, sense of security, and control, which are transformed into categorical variables: 0 to 40 = 1; 41 to 60 = 2; 61 to 80 = 3; 81 to 100 = 4, as specified in the CEQ instructions. Ratings of negatively worded statements and the pain item were reversed, so the higher scores reflect more positive scoring. 13
The s-QPP was administered in the paper form on the day of discharge. Four weeks postpartum, participants were contacted by email and invited to complete the CEQ using Google Forms. If no response was received, a reminder and survey link were subsequently sent via WhatsApp.
The CEQ and s-QPP questionnaires were validated at the Riga Maternity Hospital at the beginning of the study. Both instruments underwent validation in accordance with the Psychology Laboratory guidelines for adapting research instruments, based on the International Test Commission Guidelines for Translating and Adapting Tests, Second edition. 18 First, the s-QPP and CEQ were translated from English to Latvian by 2 independent translators, after which team members proofread and edited the translations. Second, 5 postpartum women completed the questionnaires and took part in face validation. A team member conducted cognitive interviews to assess content, clarity, and acceptability. Afterward, the following changes had been added. In the s-QPP the question “My relatives and visitors were treated well” was supplemented with the option “It does not concern me,” as the study took place during the COVID-19 pandemic, when visitors and participation in labor was prohibited. In the CEQ, the item “My midwife devoted enough time to my partner” was rephrased as taking into account that not only a partner but also another family member or doula could be present at the birth. The answer option “Not applicable” was added to the questions “I had the freedom to choose the method of pain relief I wanted during childbirth” since women understood that epidural anesthesia was the only option for pain relief, and “The midwife dedicated enough time to the person accompanying me” due to COVID-19 restrictions on accompanying persons during childbirth. In the Latvian language, there are no distinct terms for “labor,” “birth,” and “childbirth.” The Latvian term covers all stages, and similar issues have been noted in other languages during face validation. In Latvian, the understanding of a specific stage of labor is based on the text and content. Finally, 50 women were asked to fill in the questionnaires. Internal consistency was measured by calculating Cronbach's alpha for each of the domains. A Cronbach's alpha was >.70 (satisfactory) across all domains.
Statistical analyses were carried out using IBM SPSS Statistics version 27.0. For nonparametric data, the median and interquartile range, parametric data—mean, standard deviation were used. Parametric t-tests were applied to normally distributed data, whereas nonparametric tests (Mann–Whitney U test and Kruskal–Wallis test) were used for non-normally distributed data or small sample sizes. Statistical significance was defined as P < .05. To account for multiple testing, P-values were adjusted using the Holm–Bonferroni method for familywise error rate.
Correlations between interventions and CEQ domains were assessed using Spearman rho. Correlation coefficients were interpreted as follows: 0.01 to 0.19 = negligible, 0.20 to 0.29 = weak, 0.30 to 0.39 = moderate, 0.40 to 0.69 = strong, and ≥0.70 = very strong relationships.
Results
Out of 150 patients, 96.0% (N = 144) completed the s-QPP, and 91.3% (N = 137) completed the CEQ. Both questionnaires were obtained from 88.7% (N = 133) of participants, who were therefore included in the further analyses.
The study populations were predominantly in their late 20s, with a mean maternal age of 28.9 years. The median gestational age at delivery was 41 weeks. Patients’ characteristics and the obstetrical data are presented in Table 1.
Characteristics of the Study Population.
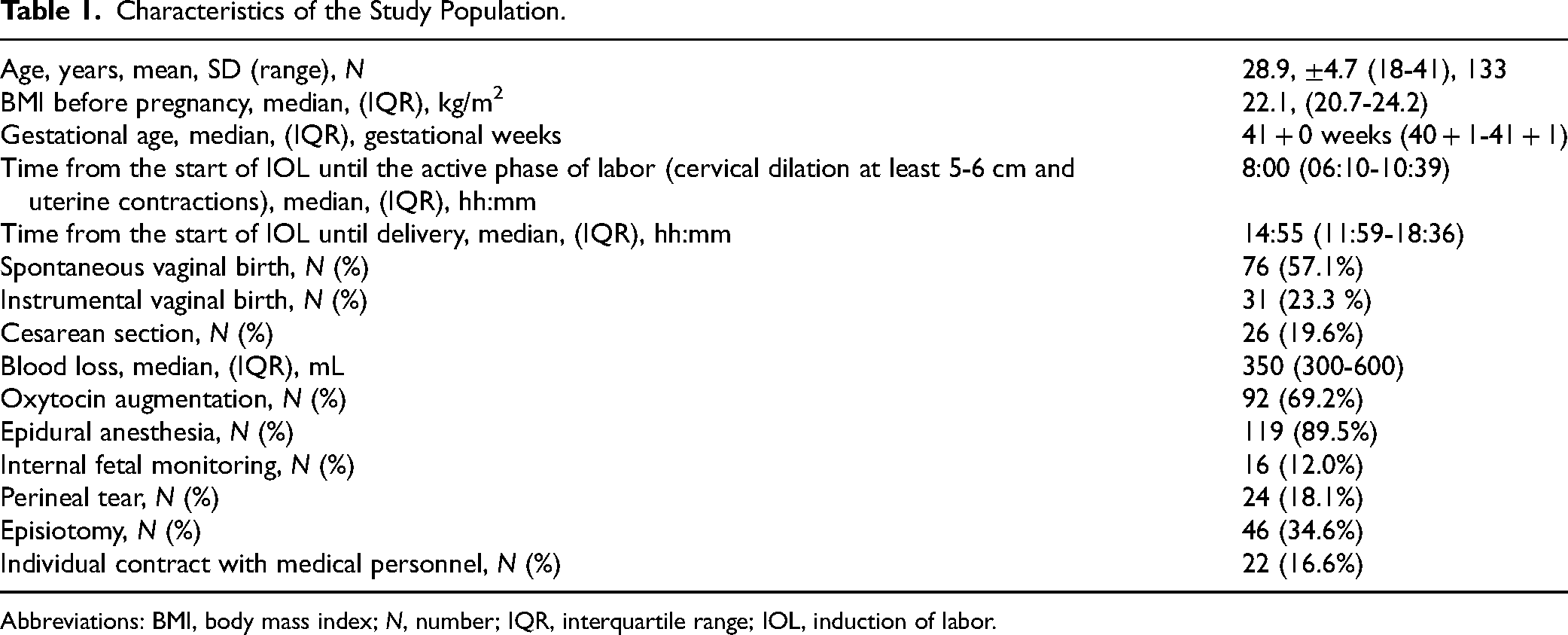
Abbreviations: BMI, body mass index; N, number; IQR, interquartile range; IOL, induction of labor.
The mean scores on all s-QPP items were above 3 points (Table 2). The lowest-rated questions were “I received food and drink that I liked” (3.19) and “I had a comfortable bed” (3.03). In contrast, patients reported relatively high scores for medical care, pain relief, information provided, and privacy. The mean scores in the CEQ were generally lower, ranging from 1.79 to 3.61. The lowest score was for the statement regarding the experienced pain during childbirth (1.79), whereas effective pain relief received the highest mean score (3.61). On the “Professional support” domain, questions related to midwifery care received the highest ratings: the midwife devoted enough time to the patient (3.54), kept the patient informed (3.56), and made the patient feel well cared for (3.59) (Table 2).
Dimensions and Factors of s-QPP and CEQ.

Abbreviations: s-QPP, short version of the Quality from the Patient's Perspective; CEQ, Childbirth Experience Questionnaire.
Mean and standard deviation (SD).
When comparing mean scores across domains, the s-QPP showed consistently higher values (>3.33), while in the CEQ the highest scores were achieved for “Professional support” (3.55) and “Participation” (3.05) domains. However, patients reported lower satisfaction with the emotional aspects—whether they felt strong, capable, happy, tired, or scared (“Own capacity” mean score 2.47; “Perceived safety” mean score 2.99) (Table 3).
Comparison of Responses of Questionnaires.

Abbreviations: s-QPP, short version of the Quality from the Patient's Perspective; CEQ, Childbirth Experience Questionnaire.
Mean and standard deviation (SD).
Table 4 summarizes various intervention scenarios and their impact on patient's satisfaction across the 4 CEQ domains. Women with an individual contract with either a midwife or a physician reported significantly higher scores across all 4 domains, as confirmed by the Holm–Bonferroni correction. Analysis by mode of delivery revealed significant differences in the domains of “Own capacity,” “Perceived safety,” and “Participation.” Episiotomy was associated with significantly lower scores in “Own capacity” and “Perceived safety.” Conversely, women who sustained a perineal tear reported significantly higher scores in “Own capacity” and “Participation.” In contrast, obstetric interventions, including oxytocin augmentation and internal fetal monitoring, were linked to significantly lower scores in the “Own capacity” domain.
Summary of Patient Satisfaction Across Delivery Intervention Scenarios in the 4 CEQ Domains.
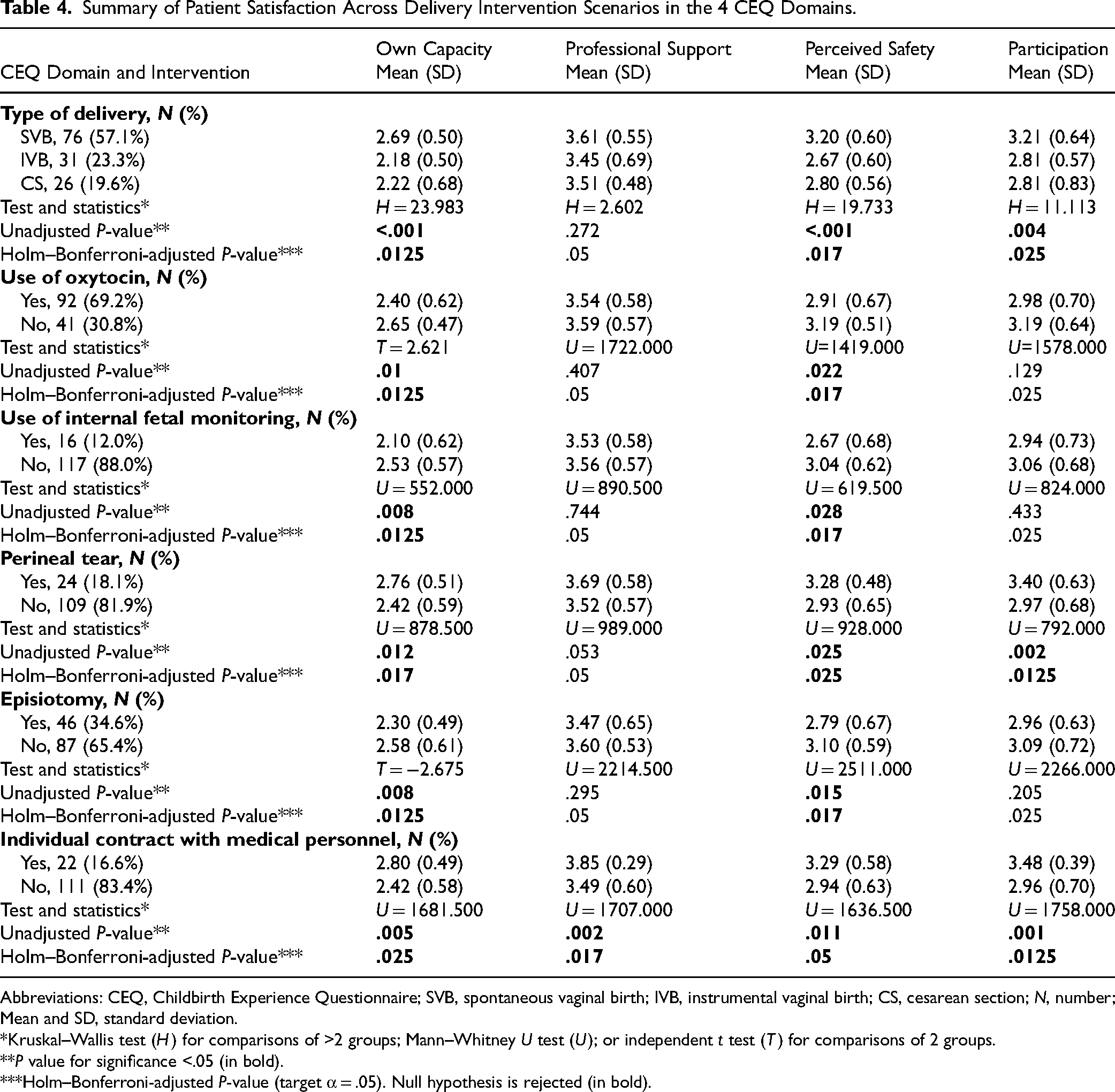
Abbreviations: CEQ, Childbirth Experience Questionnaire; SVB, spontaneous vaginal birth; IVB, instrumental vaginal birth; CS, cesarean section; N, number; Mean and SD, standard deviation.
*Kruskal–Wallis test (H) for comparisons of >2 groups; Mann–Whitney U test (U); or independent t test (T) for comparisons of 2 groups.
**P value for significance <.05 (in bold).
***Holm–Bonferroni-adjusted P-value (target α = .05). Null hypothesis is rejected (in bold).
Among the 31 patients who experienced an instrumental vaginal birth (IVB), 83.9% (N = 26) underwent an episiotomy, whereas only 26.3% (N = 20) of those with a spontaneous vaginal birth did so.
A significant but weak negative Spearman's rho correlation was found between the time from the beginning of IOL to the time baby was born, and both the “Own capacity” (ρ = −0.227, P = .009) and “Perceived safety” (ρ = −0.182, P = .036) domains (Figure S1 in the Supplemental materials). This indicates that the longer the duration from the start of IOL to delivery, the lower the scores on the “Own capacity” and “Perceived safety” domains.
A moderately strong negative correlation was noted between the blood loss and the “Own capacity” domains (ρ = −0.331, P < .001), indicating that greater blood loss is associated with lower scores on this domain. A weaker, yet significant, correlation was observed between blood loss and the “Perceived safety” domain (ρ = −0.276, P = .001), suggesting that increased blood loss is associated with lower perceived safety (Figure S2 in the Supplemental materials).
Discussion
To our knowledge, this is the first study in Latvia to explore primiparous women's opinions of their childbirth experience during the first postpartum month using 2 validated patient experience tools: the s-QPP questionnaire, administered shortly after birth at discharge, and the CEQ 1 month later. Our results demonstrated factors positively impacting the childbirth experience as the type of delivery and contract with midwife or doctor. Factors negatively impacting maternal perception of capability and security of childbirth are instrumental vaginal delivery, cesarean section, oxytocin augmentation, internal fetal monitoring, episiotomy, excessive blood loss, and prolonged induction-to-delivery time.
Opinions differ regarding the optimal timing for assessing feelings and the overall experience of childbirth. Our study strategy was to use 2 different validated instruments at different time points, demonstrating that the timing of questionnaire administration matters—patients provided more positive responses immediately after delivery compared with 1 month postpartum. In our study, the s-QPP questionnaire completed in the hospital setting yielded fewer findings than the CEQ.
The results of the s-QPP questionnaire demonstrated that primiparous women reported high levels of satisfaction with the care they received during their hospital stay, particularly in domains related to medical and technical competence and the interpersonal aspects of care. Most women agreed that they received effective pain relief, underwent timely examinations, and were treated respectfully by doctors and midwifes. Notably, while overall satisfaction was high, lower mean scores were observed in aspects related to physical comfort, such as bed quality and satisfaction with food and drink, suggesting that nonclinical factors still influence women's perceptions of quality. 10 Using the s-QPP in this context highlights its utility as a practical, patient-centered tool for evaluating the quality of care at the point of discharge when experiences are still fresh and feedback can be effectively captured. 9
The chief revelations were observed analyzing different factors and the CEQ, likely reflecting a shift from initial emotional reactions to a more balanced, often critical evaluation of their birth experience, in accordance with previous findings where early optimism fades over time, allowing for a clearer perspective. 15 Our study group, due to primiparity and IOL, is at higher risk for poor childbirth experiences. 19 Unpredicted interventions, such as episiotomy, oxytocin augmentation, internal fetal monitoring, and postpartum hemorrhage, significantly impacted whether mothers felt capable and strong, able to control and manage labor, whether they handled the situation well, and whether they had positive memories of childbirth.
From the results, women who did not have internal fetal monitoring felt more capable during labor, possibly indicating that while the presence of advanced equipment can enhance the perceived technical competence of healthcare providers, it may also increase anxiety for some patients. A similar conclusion was reached in a UK national survey, which revealed that although few women wanted to see medical equipment during childbirth, it was important for two-fifths of them to know that the equipment was available but out of sight, as they preferred to maintain a nonclinical atmosphere. 20
Local hospital protocols recommend episiotomy for primiparous women in the case of IVB, and this is also evident from the results, which show that most episiotomies occur during IVB. The main purpose of episiotomy is as a protective measure against obstetric anal sphincter injury in nulliparous women at term during IVB. 21 The results of the study show that women who underwent episiotomy reported significantly lower scores in both “Perceived safety” and “Own capacity” after 1 month. This is consistent with the notion that episiotomy may negatively impact women's psychological and emotional well-being during labor. 22 However, other studies indicate that neither episiotomy nor labor induction significantly affects patient satisfaction. 23 When an intervention is necessary or desired, women wish to maintain a sense of personal accomplishment and control by being actively involved in decision-making. 24 In cases where an episiotomy is to be performed, the woman should be informed both before the procedure and after delivery, to promote understanding of the necessity and the extent of the intervention.
Contrary to expectations, perineal tears did not negatively affect mothers’ perceptions of childbirth. Women who experienced a spontaneous perineal tear reported a more positive childbirth experience compared with those who underwent an episiotomy. This may be because natural occurrences, such as perineal tears, are perceived differently from medical interventions. A spontaneous tear may occur in a birth process where the woman actively participated, felt in control and experienced greater empowerment. In contrast, an episiotomy—often accompanied by vacuum extraction or forceps—can involve a perceived loss of control and feelings of helplessness, which may contribute to psychological distress and a negative body image.25,26 Research confirms that episiotomy is associated with higher rates of perineal pain, dyspareunia, and overall dissatisfaction compared with perineal tear repair.27,28 This suggests that the psychological sense of agency and involvement in decision-making may have a stronger influence on overall satisfaction than the physical consequences of perineal trauma.
Findings suggest that oxytocin administration may be linked to lower patient-reported feelings of safety during labor, while women who did not receive oxytocin felt more capable. This aligns with research indicating oxytocin's negative impact on childbirth experience.29–31 Another study found that oxytocin use may increase postpartum posttraumatic stress symptoms. 32 Conversely, a prospective observational study associated synthetic oxytocin with a reduced risk of postpartum mood disorders, even after accounting for newborn hospitalization and negative birth experiences. 33 In conformity with patient-centered care, patients should be informed of risks and benefits and reassured about oxytocin's safety, as supported by available research.
Individual contracts with medical personnel result in significantly higher scores across all 4 CEQ domains. Personalized care from midwives provides more time and thorough information, fostering safety through trust and emotional security. Familiarity with childbirth helps reduce fear and anxiety, enhancing confidence during labor. Studies indicate that educating patients before delivery is crucial for alleviating misconceptions and improving overall birth experiences.34,35 Ultimately, these factors significantly influence women's feelings of safety and their memories of childbirth. Positive interactions with staff enhance the childbirth experience, supporting the importance of professional support.
Limitations
The study has several strengths and limitations. One of the strengths of this research was having both s-QPP and CEQ questionnaires included in 1 study. Rarely these 2 questionnaires are used together, and additionally patient experience was assessed both immediately and remotely after labor, which allowed us to evaluate the difference of patient's perspectives of labor over time. A limitation of the study could be the small sample size, which possibly limited the revealing of supplementary or diverse findings. Further investigation could provide critical insights for improving maternity care services. A valuable direction for future research would be to examine how IOL influences postpartum recovery, mental health outcomes, and family planning.
Conclusion
Childbirth is a highly personal experience, and there is no universal tool to assess it. Various questionnaires can be employed to document mothers’ experiences. Our findings revealed that main factors positively affecting the childbirth experience were the type of delivery and having a contract with midwife or doctor. These findings are particularly relevant for healthcare providers in Latvia. The legislation and working conditions should be changed to promote that 1 midwife could work with 1 patient at a time and devote more energy and care for patients. Such improvements may also have a broader impact on national population policies and efforts to encourage higher birth rates, which is particularly important in small countries.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251413864 - Supplemental material for Childbirth Experience Among Primiparous Women in Latvia Using Short-Quality from Patient's Perspective (s-QPP) Questionnaire and Childbirth Experience Questionnaire (CEQ)
Supplemental material, sj-docx-1-jpx-10.1177_23743735251413864 for Childbirth Experience Among Primiparous Women in Latvia Using Short-Quality from Patient's Perspective (s-QPP) Questionnaire and Childbirth Experience Questionnaire (CEQ) by Agnija Vecvagare, MD, Beāte Sārta, MD, Laura Rācene, MD, Līva Ķīse, MD, Zane Rostoka, MD, Ieva Pitkēviča, MD, Katrīna Laura Vaganova, Dace Rezeberga, MD, PhD, and Natālija Vedmedovska, MD, PhD in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735251413864 - Supplemental material for Childbirth Experience Among Primiparous Women in Latvia Using Short-Quality from Patient's Perspective (s-QPP) Questionnaire and Childbirth Experience Questionnaire (CEQ)
Supplemental material, sj-docx-2-jpx-10.1177_23743735251413864 for Childbirth Experience Among Primiparous Women in Latvia Using Short-Quality from Patient's Perspective (s-QPP) Questionnaire and Childbirth Experience Questionnaire (CEQ) by Agnija Vecvagare, MD, Beāte Sārta, MD, Laura Rācene, MD, Līva Ķīse, MD, Zane Rostoka, MD, Ieva Pitkēviča, MD, Katrīna Laura Vaganova, Dace Rezeberga, MD, PhD, and Natālija Vedmedovska, MD, PhD in Journal of Patient Experience
Footnotes
Acknowledgments
We extend the heartfelt gratitude to Jeļena Perevožčikova of Riga Stradiņš University for her invaluable assistance with the statistical analysis.
Author contribution
AV: Questionnaire translation, validation, distribution, data curation, writing - original draft, formal analysis, resources, writing - review and editing, visualisation. BS: Questionnaire translation, validation, distribution, writing original draft, writing - editing, resources, visualisation. LR: Conceptualization, methodology, investigation, formal analysis, writing - review and editing. LĶ: Questionnaire translation, validation, data curation. Ieva Pitkēviča: questionnaire distribution, data curation. ZR: questionnaire distribution, data curation. KLV: questionnaire distribution. DR: Conceptualization, methodology, writing - review and editing, supervision. NV: Conceptualization, methodology, writing - review and editing, supervision.
Data Availability
The data that support the findings of this study are available in Rīga Stradiņš University Institutional Repository Dataverse at https://doi.org/10.48510/FK2/OUKKBV, UNF:6:qs/Z2M9HcG9bfbo3Pq4E6g== [fileUNF].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The Riga Stradiņš University Research Ethics Committee approved the study in March 2022 (No. 2-PĒK-4/152/2022).
Informed Consent
All participants provided written informed consent prior to data collection for their anonymized information to be published in this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the Latvian Council of Science project “Role of Metabolome, Biomarkers and Ultrasound Parameters in Successful Labour Induction,” project No. lzp-2021/1-0300.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.