
Abstract
We performed a retrospective cohort study of patients admitted to a novel, home-based COVID Virtual Observation Unit (CVOU) from an urban, university-affiliated emergency department with ∼112,000 annual visits. Telephone-based survey questions were administered by nursing staff working with the program. Of 402 patients enrolled in the CVOU, 221 (55%) were able to be contacted during the study period; 180 (45%) agreed to participate in the telephone interview. Overall, 95% (169 out of 177) of the surveyed patients reported 8 to 10 on the likelihood to recommend CVOU and 82% (100 out of 122) rated the quality of care as 10 out of 10. Over 90% of respondents reported that all role groups (nurses, paramedics, and physicians) treated them with courtesy and respect, explained things in an understandable way, and listened to them carefully. Over 80% of respondents reported that the program kept them at home. In summary, patient experiences with this novel home-based care program were highly positive. These data help underscore the importance of patient-centeredness in home-based care, and further support the concept of these innovative care models.
Introduction
Patient experience is increasingly recognized as one of the most important measures of healthcare quality and effectiveness, with well-established positive impacts on outcomes including decreased hospital readmission, improved clinical outcomes,1-3 decreased medicolegal risk,4,5 and decreased emergency department (ED) use. 6
During the second surge of COVID in our city, we implemented a novel COVID Virtual Observation Unit (CVOU) to help symptomatic patients who tested positive for COVID to safely isolate at home with the aid of remote monitoring. Our approach paired remote symptom and oxygen saturation monitoring with a Mobile Integrated Health (MIH) platform utilizing community paramedics and was staffed by nurses and physicians. While several COVID remote monitoring programs utilized pulse oximeters and/or self-reported symptoms, none that we know of combined these with community paramedicine to expand the scope of patient care in the home.
Patient experience with other home-based care has been reported in palliative care, 7 home dialysis, 8 hospital at home,9-11 and telehealth for patients isolated at home with COVID. 12 Prior work in this area has demonstrated the importance of care coordination, patient education and communication, and personalization of care. Since this CVOU program is novel, it is critical to better understand patients’ perspectives. As part of our quality improvement, we sought to better understand and characterize patient experience with the CVOU care model. Our aim was to understand the patient's overall experience and their perceptions of interactions with program staff and the value of the program.
Methods
Study Design, Setting, and Population
We performed a retrospective cohort study of patients admitted to our novel CVOU from an urban, university-affiliated ED with ∼112,000 annual visits. All adult patients who were enrolled in the CVOU from January 13 to March 19, 2021, were eligible for inclusion. There were no exclusion criteria.
As a quality improvement effort, this analysis was exempt from human subject review by the Institutional Review Board.
Participation
Patients enrolled in the CVOU program reported their symptoms either through our electronic health record's patient-facing mobile app, a web application, or a daily phone call from nurses dedicated to this program. Patients were enrolled for the recommended 14 days of COVID isolation. If a patient reported symptoms that were worse than the day prior, an alert was sent to the nurse who triggered a nurse phone call to assess the patient. If the nurse was concerned about the need for a potential ED visit, they contacted the remote physician covering the program who determined via phone call if the patient could remain at home, needed transport to the ED, or could have an MIH paramedic dispatched to the patient's home. The MIH paramedic evaluated the patient, including resting and exertional vital signs, and facilitated a video visit with the covering emergency medicine attending physician.
Survey Instrument, Data Collection, and Variables
A survey instrument assessed patient experience across several domains (see Online Appendix 1) and was generated through a combination of questions from 2 patient experience survey services, ED Consumer Assessment of Healthcare Providers and Systems, 13 and NRC Health, 14 to allow for direct comparison of feedback to current ED metrics. The primary outcome was overall satisfaction, as determined by the answer to the questions, “On a scale from 1–10, with 1 being not at all likely and 10 being highly likely, how likely would you be to recommend the COVID Symptom Monitoring program to your friends and family?” and “If using any number from 0 to 10, where 0 is the worst care possible and 10 is the best care possible, what number would you use to rate your care from the COVID Symptom Monitoring program?” Secondary outcomes included patients’ experience with different role groups in the program and their experience with aspects of patient experience, such as feeling listened to and whether their providers in the CVOU were knowledgeable.
The phone-based survey was administered by nurses working in the CVOU between March 29 and April 2, 2021, which could have been up to 79 days after discharge. The survey was conducted in the patient's preferred language, and an interpreter was available by phone when the nurse did not speak the same language as the patient. Up to 3 attempts were made to reach each patient by phone. When a nurse reached a patient, the patient was asked if they would be willing to respond to patient experience questions. If the patient agreed, informed consent was assumed.
Statistical Analysis
Descriptive statistics were used to assess patient responses to the survey questions. All study variables were selected a priori for analysis.
Results
Study Cohort Response Rate and Characteristics
Of 402 patients enrolled in the CVOU, 221 (55%) were reached for the follow-up survey, and 180 (45%) agreed to participate in the telephone interview. The mean age of the respondents was 57 years old (SD = 17) and 56% were female. We did not require respondents to answer all questions on the survey, and some patients chose not to answer certain questions. Denominators are described below when it was not 180.
Overall Patient Experience
Overall, 95% (169 out of 177) of the patients reported 8 to 10 on the likelihood to recommend CVOU, with 83% (n = 147) reporting 10 out of 10 (see Online Appendix 1). Regarding the quality of the care, 82% (100 out of 122) of patients rated it as 10 out of 10. Regarding the patient's perception that the program avoided an ED visit, 83% (138 out of 167) reported positively. Of the respondents, 96% (170 out of 177) reported that they were reassured being monitored at home and that being monitored at home was the right decision for them (Table 1).
Respondents General Perceptions of the COVID Virtual Observation Unit (CVOU).

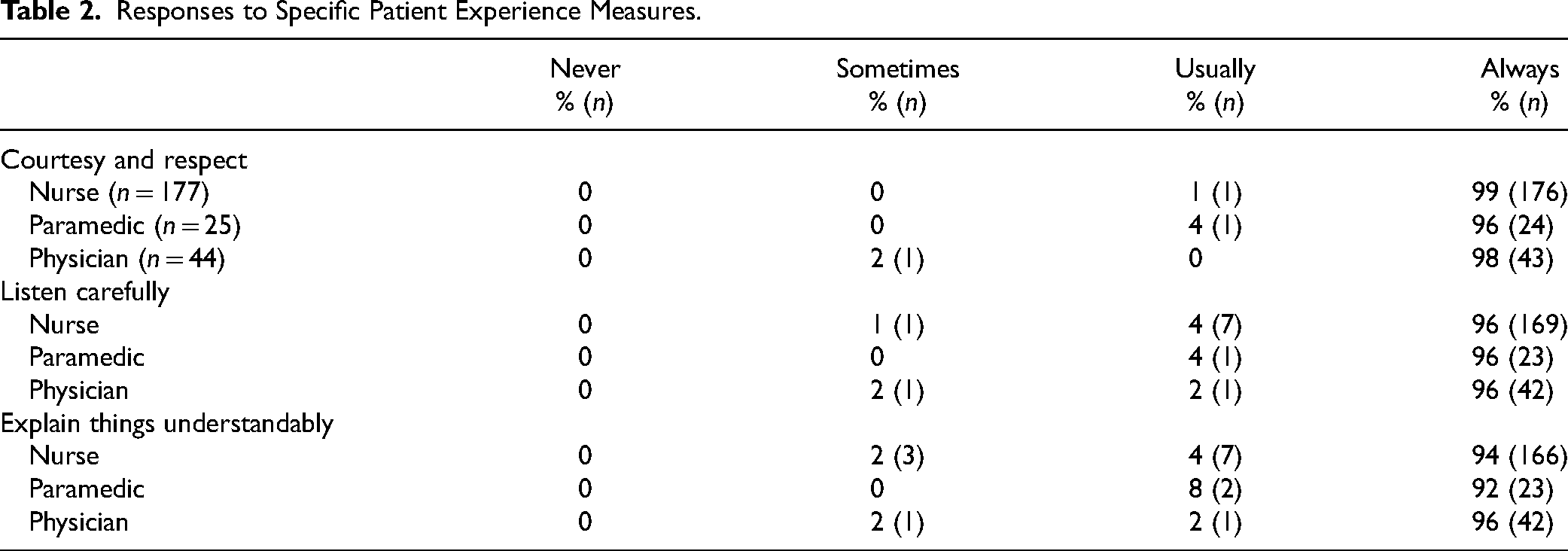
With respect to patient-centered communication, across all 3 role groups (nurses, paramedics, and physicians), over 90% of respondents indicated that they were “always” treated with courtesy and respect, were explained things in a way they could understand, and were listened to carefully (Table 2).
Responses to Specific Patient Experience Measures.
Discussion
In this study, we describe the experience of patients enrolled in a novel CVOU. Prior studies have proven the importance of patient experience on program feasibility, health outcomes, and provider satisfaction.7-11,15. Very few have measured patient experience with home-based care provided by emergency medicine teams, and none with a CVOU care model incorporating both remote symptom monitoring and MIH resources. Our study demonstrated a very positive experience both overall and on specific measures of the patient experience.
Although we cannot make direct comparisons to other care models, performance on these measures compare very favorably to ED and hospital-based care model measures and benchmarks. As the clinicians in this program are based in emergency medicine, a specialty with somewhat lower patient experience scores compared to other care venues, the high experience scores were welcome during the difficult COVID surge in the ED.
Home-based care will likely play a larger role in the healthcare system with the development of Hospital at Home programs, 9 and with a push to a home-to-home time of zero. 16 Given that these models tend toward patient-centered care more than within clinics or hospitals, patient experience may be even more important to these models in the future. As healthcare professionals, we are bringing our work into the patient's homes. Patient experience should inform further development and refinement of such programs.
Our results underscore another benefit of home-based care models, and the feasibility of emergency medicine physicians and nurses caring for patients outside of the brick-and-mortar EDs and ED observation units.
Limitations
This study has several limitations. First, as a single-center study at a tertiary care center, our results may not be generalizable to all healthcare settings. However, given the fundamental similarities between models of emergency care and the patients we serve, it is likely that at least some components of our results will be broadly applicable. In addition, the low survey response rate, although consistent with national satisfaction survey response rates, introduces the possibility of selection bias which could have influenced the results. Another limitation was the use of the CVOU nurses in the survey administration. It is possible that the patients rated their experience higher if a nurse who took care of them in the CVOU was the one administering the survey. Patients or patient advocates were not involved in the survey design; however, the survey instruments, from which the CVOU were adapted, report that patients had provided input into their survey questions. Since respondents could skip questions, our results may not be capturing the full picture of the patients’ perceptions of the program. While patients were asked for any further comments, their responses were not always captured verbatim and thus were not analyzed using accepted qualitative methods. Future studies would be valuable to better understand a patient's perspective regarding successes and potential areas of improvement. Finally, to keep our survey a reasonable length, we did not investigate all domains of patient experience, and thus our study is subject to omitted variable bias and the findings can only be interpreted in the context of the variables we analyzed.
Conclusion
Patient experiences with a novel home-based care program were highly positive, both in terms of overall satisfaction and specific measures of care quality and effectiveness. While further study is warranted, these data help underscore the importance of patient-centeredness in home-based care, and further support the concept of these innovative care models.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735231171124 - Supplemental material for Patient Experience With an In-Home COVID Virtual Observation Unit: An Analysis
Supplemental material, sj-docx-1-jpx-10.1177_23743735231171124 for Patient Experience With an In-Home COVID Virtual Observation Unit: An Analysis by Emily M Hayden, Stephen C Dorner, Jonathan D Sonis and Benjamin A White in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.