
Abstract
Oral immunotherapy (OIT) is an emerging treatment for pediatric food allergies; however, decision support strategies in Japan remain underdeveloped and culturally nuanced. This qualitative descriptive study explored the OIT decision-making experiences and support needs of children, their parents, and healthcare professionals. Fourteen participants were recruited from 2 tertiary medical centers in Tokyo and Kanagawa. Individual semi-structured interviews were conducted and thematically analyzed. Three core themes emerged: navigating complex choices by balancing safety, burden, and values; centering on the child's voice through participation, emotional awareness, and autonomy; and bridging gaps in informational, emotional, and peer support to enable shared decision making (SDM). A conceptual model grounded in the Ottawa Decision Support Framework and the Japanese cultural context illustrates how stakeholder-specific needs interact to shape the quality of decisions. This study highlights the rarely examined intersection of pediatric autonomy, clinical uncertainty, and sociocultural context. These findings underscore the need for culturally responsive and child-inclusive SDM strategies and tailored decision aids to support families navigating pediatric OIT.
Introduction
Food allergy burdens children globally, with a prevalence of ∼8% in young children in some Western countries,1,2 and is a growing public health concern in industrialized regions. 3 Oral immunotherapy (OIT) offers potential desensitization and improved quality of life,4,5 but can have consequences for long-term home management and carries risks of adverse reactions, including anaphylaxis.6,7
In Japan, pediatric OIT is rapidly expanding, but the practice has not yet been standardized, and implementation varies across settings.8,9 As a result, families may not receive consistent information or specialized counseling, which can hinder decision making and contribute to distress and uncertainty.4,5
Shared decision making (SDM) is critical for OIT4,5 and aligns choices with patient values. 10 The Ottawa Decision Support Framework (ODSF) supports SDM by identifying decisional needs and was recently updated to validate and expand these concepts.11,12 However, pediatric SDM is complex, involving multiple stakeholders and developmental considerations, and children's preferences may be missed. 13
Pediatric SDM remains under development in Japan. Deference to healthcare professionals (HCPs) and limited child involvement may constrain open dialogue, and few tools are available to support age-appropriate participation in OIT decisions.14,15 Despite children's rights to express views 16 and internationally recognized strategies for youth involvement, 17 few tools exist in Japan to support age-appropriate participation in OIT decisions.4,18
To date, no Japanese qualitative study has comprehensively explored OIT decision making from the interdependent perspectives of children, parents, and HCPs. Understanding their needs in Japan's sociocultural and healthcare context, in which decision support is poorly defined, is critical for designing effective and inclusive interventions. 5
Building on this gap, we investigated the decision-making experiences and support needs of children, parents, and HCPs in pediatric OIT in Japan. By incorporating children's perspectives, these findings, aligned with systematic patient decision aid development frameworks, Coulter et al 19 provide foundational evidence for developing inclusive tools that may strengthen SDM practices in Japanese pediatric care.
Methods
Study Design
This study employed an exploratory qualitative descriptive design20,21 to investigate the OIT decision-making experiences and support needs of children with food allergies, their parents, and HCPs in Japan. Adhering to the COREQ guidelines, 22 participant triangulation (children, parents, and HCPs) captured multifaceted perspectives on this phenomenon, where clinical decisions intersect with complex emotional and social realities. 23
Participants and Recruitment
Participants were recruited via convenience sampling facilitated by pediatric allergy specialists at 2 tertiary medical centers in Tokyo and Kanagawa (April 2020-March 2021). The inclusion criteria targeted parents of children newly diagnosed with IgE-mediated food allergy who had made an OIT decision, children aged 9 to 18 years who were involved in OIT decision making, and pediatricians/nurses providing OIT decision support. Fourteen participants (5 parents, 3 children, and 6 HCPs; Table 1) were enrolled in the study. None of the participants declined to participate in the study. Four parents chose OIT, and one chose avoidance. The COVID-19 pandemic presented recruitment challenges, potentially affecting sample size and diversity.
Demographic Characteristics of Study Participants (N = 14).
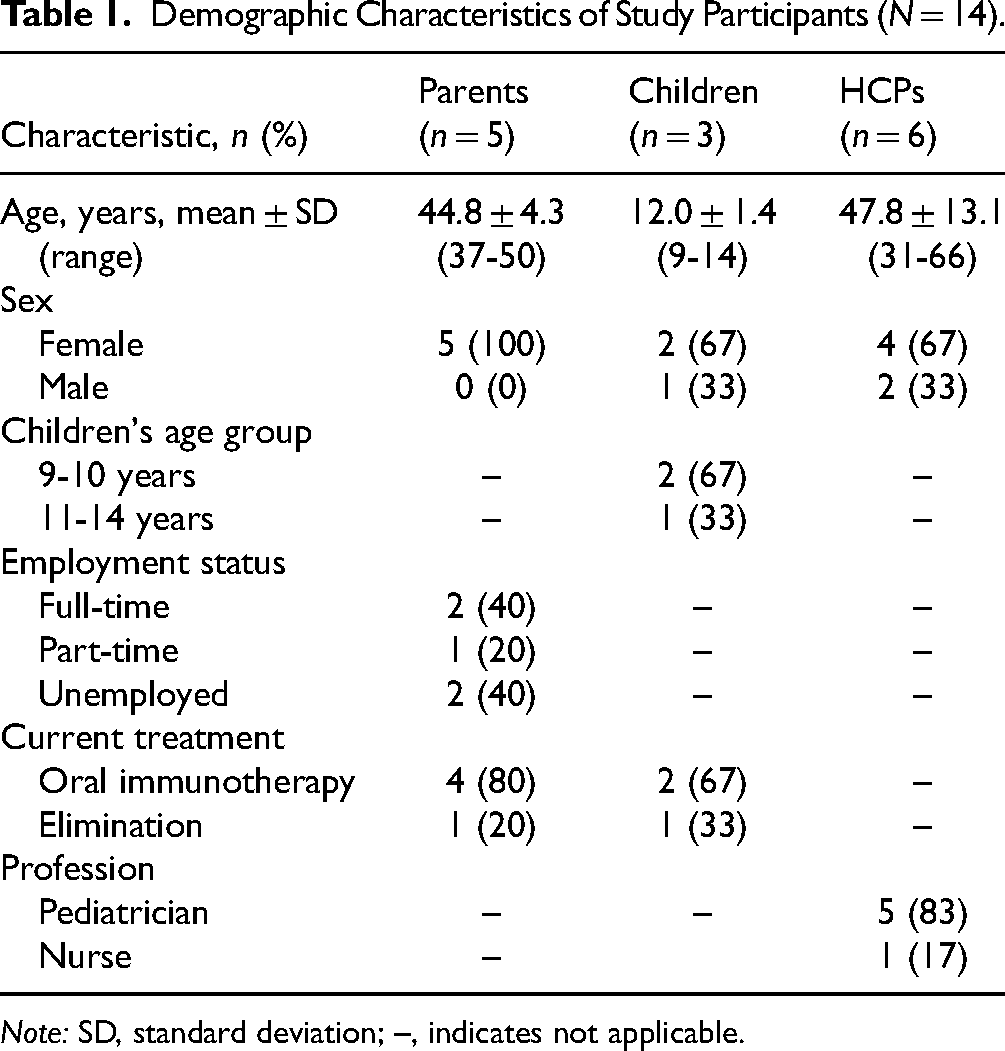
Note: SD, standard deviation; –, indicates not applicable.
Data Collection
The first author, a female registered nurse, university teacher, and mother of a child with severe food allergies, trained in qualitative research and with no prior relationship with the participants or recruiting hospitals, conducted semi-structured interviews (30-60 min). Participants were informed of the researcher's background as an HCP and were interested in improving their OIT experience. Separate group-specific interviews were conducted to explore perceptions, decision-making experiences, and support needs (see Supplemental Material: Interview Guide). Interviews, audio-recorded and transcribed verbatim, were held online per participant's preference or in person at a private location convenient for the participants, such as a hospital meeting room or quiet space. The children chose to conduct individual interviews or be interviewed with their parents. We conducted iterative data collection and preliminary analyses. Recruitment limitations due to the COVID-19 pandemic precluded definitive judgment of thematic saturation, although the enrolled participants provided rich data.
Data Analysis
Data interpretation was guided by reflexive thematic analysis. 24 Verbatim transcripts, managed in NVivo 14 (QSR International), were inductively coded line-by-line by the first author without a predetermined framework. The codes were iteratively reviewed, grouped into subcategories, and abstracted into overarching themes through constant comparisons and reflections. To ensure analytical rigor, the first author maintained reflexive memos throughout the analysis. Participant checking was not performed to minimize participant burden and logistical constraints related to the study timeline. Instead, rigor was enhanced through regular discussions with a second experienced qualitative researcher. These discussions involved co-reviewing selected transcripts and preliminary codes, exploring alternative interpretations, challenging assumptions to deepen reflexivity, and ensuring thematic coherence with the theoretical framework, while acknowledging the interpretive nature of reflexive thematic analysis. The identified themes were interpreted and organized using the ODSF as a conceptual lens, situating participants’ experiences within a structured model of decisional needs, support mechanisms, and outcomes.
Ethical Considerations
Ethical approval was obtained from St. Luke's International University (No. 19A-086) and the Tokai University School of Medicine (No. 19R-272). All adult participants and the parents of child participants provided written informed consent, and the children provided assent. Participation was voluntary, and the data were anonymized.
Results
Fourteen participants (5 parents, 3 children, and 6 HCPs) were enrolled in this study. The demographic characteristics, including age, sex, and treatment status, are shown in Table 1.
Three primary themes emerged from the participant interviews: (1) navigating complex choices (balancing safety, burden, and values); (2) centering the child's voice (participation, emotions, and autonomy); and (3) bridging gaps in support (toward child-inclusive SDM). Table 2 presents illustrative quotes and detailed supporting data for each theme. These themes contribute to the conceptual model of OIT decision making and support needs, as shown in Figure 1.

A Child-Centered Conceptual Model for Shared Decision Making in Pediatric Oral Immunotherapy in Japan.
Themes and Illustrative Quotations From Stakeholders.
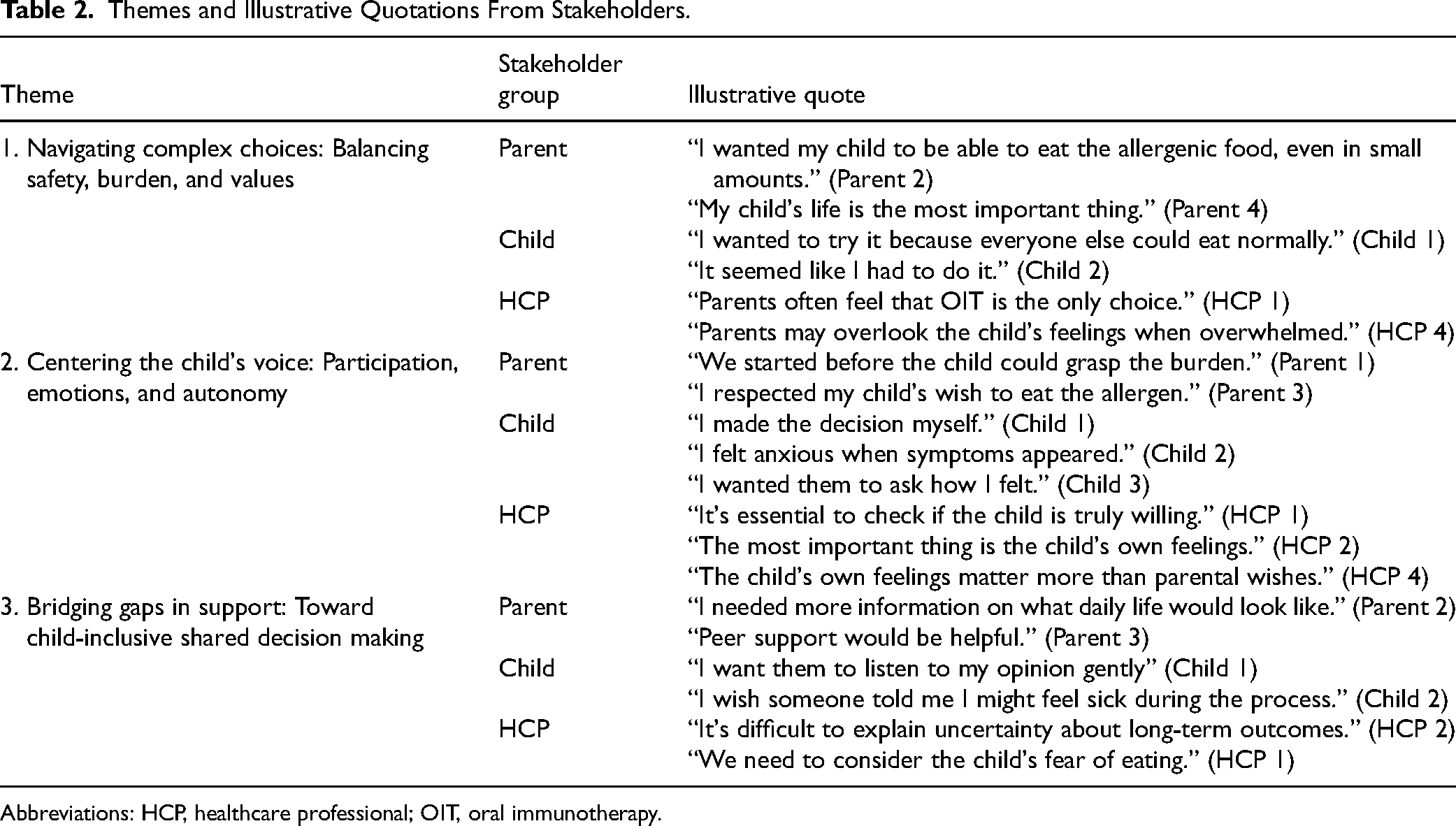
Abbreviations: HCP, healthcare professional; OIT, oral immunotherapy.
Theme 1: Navigating Complex Choices: Balancing Safety, Burden, and Values
Decision making regarding OIT presents families with complex considerations that require balancing child safety, treatment burden, and personal or family values. These tensions reveal overlapping decision-making challenges for parents, children, and HCPs.
The parents primarily wanted to protect their children from life-threatening reactions. “My child's life is the most important thing,” said one (Parent 4), emphasizing foundational concern. Others hoped to ease restrictions and constant anxiety regarding accidental exposures. “I wanted my child to be able to eat allergenic food, even in small amounts” (Parent 2), reflecting a common desire for normalcy. However, these hopes were tempered by concerns about daily dosing, long-term uncertainty, and the emotional toll of possible treatment failures.
Children's roles and perspectives varied. Some were eager to try OIT to eat like peers: “I wanted to try it because everyone else could eat normally” (Child 1), while others felt pressured: “It seemed like I had to do it” (Child 2). These responses suggest that children's perceived agency is shaped by how the options are framed.
The HCPs noted that families often considered OIT to be their only choice, particularly in severe cases. “Parents often feel that OIT is the only choice” (HCP 1). Another observed, “Parents may overlook the child's feelings when overwhelmed” (HCP 4), highlighting how emotional stress may skew decision making. Overall, OIT decisions were influenced by clinical considerations and relational and emotional complexity.
Theme 2: Centering the Child's Voice: Participation, Emotions, and Autonomy
This theme explored how children's perspectives were included or excluded in their decision making. It addressed their levels of participation, emotional responses, and emerging autonomy.
Children reported varying degrees of involvement. One child said, “I made the decision myself” (Child 1), reflecting autonomy. Others noted gaps in communication: “I wanted them to ask how I felt” (Child 3). Another shared emotional difficulty during treatment: “I felt anxious when symptoms appeared” (Child 2).
Parents have also adopted different approaches. One said, “We started before the child could grasp the burden” (Parent 1), while another said, “I respected my child's wish to eat the allergen” (Parent 3). These views highlight the need for a balance between protecting children and supporting independence.
HCPs emphasized the need to recognize children's viewpoints. “It's essential to check if the child is truly willing” (HCP 1), said one. Another stressed, “The child's own feelings matter more than parental wishes” (HCP 4). Centering on the child's voice means acknowledging their emotional capacity and inviting their input in developmentally appropriate ways.
Theme 3: Bridging Gaps in Support: Toward Child-Inclusive SDM
Participants across groups identified gaps in informational and emotional support necessary for effective OIT and inclusive SDM.
Parents wanted more than the clinical facts. “I needed more information on what daily life would look like” (Parent 2), one parent said, emphasizing the importance of practical insight. Emotional support was also important. “Peer support would be helpful” (Parent 3) captured the value of shared experiences.
Children sought emotional support and preparation. “I want them to listen to my opinion gently” (Child 1), one child said. Another added, “I wish someone told me I might feel sick during the process” (Child 2), showing a need for anticipatory guidance.
The HCPs acknowledged barriers such as time constraints and uncertainty. “It's difficult to explain uncertainty about long-term outcomes” (HCP 2). Another participant noted, “We need to consider the child's fear of eating” (HCP 1). The HCPs emphasized presenting OIT as a genuine choice, not as a default, and called for interdisciplinary collaboration.
Integrative Summary and Model Development
The 3 themes of navigating complex choices, centering the child's voice, and bridging gaps in support, along with stakeholder-specific decisional needs and preferences (Table 2), informed the development of a conceptual model for OIT decision-making in Japan. As shown in Figure 1, this model, grounded in the ODSF, illustrates how addressing emotional and informational needs (Themes 1 and 3) and focusing on children's perspectives (Theme 2) can enhance decision quality. The model depicts the interplay between stakeholders, culturally embedded features of the Japanese healthcare context, and SDM processes. It emphasizes children's voices and agency as central to ethical and effective decision making in pediatric food allergy care.
Discussion
This study explored decision-making experiences surrounding OIT for food allergies among children, their parents, and HCPs in Japan through reflexive thematic analysis. Three inductively constructed themes were mapped onto the ODSF, resulting in a context-specific conceptual model of stakeholder experience and support needs.
Theme 1: Navigating Complex Choices
This theme underscores that OIT decisions are sensitive to preferences, involving significant trade-offs that place them in a “grey zone” of medical decision making.4,25 Our findings revealed Japanese parents’ intense desire for normalcy and safety juxtaposed with deep anxieties about treatment burdens and uncertain outcomes. While globally recognized, this internal conflict may be amplified in Japan by the rapidly expanding yet not fully standardized OIT landscape. 4 Although clinicians must clearly communicate OIT's benefits and risks, 26 our study suggests that Japanese families struggle to balance these against their values, reflecting a universal need for robust decision support. Such support should aim to enhance “decision quality” by ensuring families are adequately informed, hold realistic expectations, and make choices congruent with their values.4,27
Theme 2: Centering the Child's Voice
This theme highlights the ethical imperative 26 and practical challenges of involving children in healthcare decisions. Our results showed varied OIT involvement in Japan, ranging from active participation to feelings of pressure.
Children's emotional narratives, hope, anxiety, ambivalence, and a desire to be heard (“I want them to listen to my opinion gently”) align with pediatric SDM literature and the psychosocial impact of food allergy on their developing autonomy and identity. 28
While international calls for child participation in SDM grow,17,26,29 the Japanese sociocultural context, which values indirect communication and group harmony, may pose barriers to open expression. 14 These cultural factors might interact with developmental challenges, 28 making it harder for Japanese children to articulate true preferences regarding OIT. For example, one child felt obliged to start OIT (“It seemed like I had to do it,” Child 2). This account illustrates how sociocultural expectations of harmony and deference in Japan tend to suppress children's dissenting voice. Similar complexities in pediatric SDM, such as managing parent–child conflicts, have also been noted in the international literature. 4 Parents and HCPs may recognize the importance of children's feelings but struggle to include them in SDM, indicating a critical need for age-appropriate communication tools, specialized HCP training, 17 and safe spaces for children to express themselves.
Theme 3: Bridging Gaps in Support
The third theme revealed substantial informational and emotional needs among all stakeholders and called for enhanced support. These findings align with the ODSF's emphasis on addressing “decisional needs”11,27 and with international OIT information needs studies. HCPs acknowledged these needs but faced barriers, such as time constraints and difficulties communicating uncertainty, a point also highlighted in the Canadian Society of Allergy and Clinical Immunology (CSACI) guidelines by Bégin et al 26 regarding the need for clear information. The data suggested that HCPs tended to convey uncertainty qualitatively, referring to individual variation and the need for cautious dose titration, while the use of quantified probabilities or visual formats was limited. Parents sought practical guidance in day-to-day life, children sought advance notice of potential short-term reactions, and HCPs identified uncertainty about long-term outcomes as challenging. Practical solutions may be to state knowns and unknowns, distinguish short- and long-term horizons, use plain language scenarios when numbers are not available, confirm understanding with brief teach-back and values clarification, and agree on a review plan with timing, goals, and criteria to pause or stop. This underscores the need for structured, multifaceted support systems. 26
Moreover, support-system design should consider family decision-making structures. In this study, all parent participants were mothers, and decisions were frequently centered on maternal perspectives. One mother reported, “We started before the child could grasp the burden” (Parent 1), illustrating how caregiving responsibilities concentrated in mothers may intensify anxiety and narrow opportunities for balanced family deliberation. While this maternal predominance is consistent with caregiving practices in Japan, similar gendered dynamics have been reported internationally as contextual barriers to pediatric SDM. 13 These findings highlight the importance of designing support strategies that not only provide balanced information but also address caregiver burden and family dynamics, thereby ensuring that children's voices are not overshadowed in the decision-making process. Moreover, recent evidence in pediatric settings links higher perceived SDM with greater satisfaction with care, along with improvements in knowledge and reductions in decisional conflict.30–32
Insights from this needs assessment directly informed the development of a Japanese OIT Decision Aid (DA). At the time of this study, the Japanese DA was in the prototype stage; it has since been pilot-tested with parents and healthcare professionals to assess feasibility and usability, and a larger-scale evaluation is planned. Clinically, the DA is intended to standardize balanced, plain language information on OIT, prompt explicit elicitation of the child's preferences, and support conversations about uncertainty. While existing DAs, primarily from Western contexts, offer frameworks and the value of refining DAs through patient and caregiver feedback has been established,18,33 our findings underscore the need for a DA specifically tailored to the Japanese cultural context. This includes integrating the child's voice and addressing parental anxiety within a rapidly evolving OIT system. Developing a culturally sensitive DA that prioritizes child participation and balanced information 7 is critical for fostering genuine SDM in Japan. This involves presenting OIT as a true choice, empowering families, respecting their autonomy, and aligning with the core principles of ethical patient-centered care.4,25,27
Theoretical Contributions and Implications for the ODSF in the Japanese Context
This study applied the ODSF by showing its utility and necessary adaptations in a non-Western, pediatric, and preference-sensitive treatment setting. Our conceptual model, derived from synthesized stakeholder experiences, expands the ODSF by articulating culturally specific manifestations of decisional needs (eg, children's social anxieties and parental information gaps) and introducing facilitative mechanisms for eliciting the child's voice in Japan's OIT context. While reaffirming the universal validity of the ODSF's core components, our model reconceptualizes its application by addressing both the globally limited integration of children's perspectives in decision making and Japan's cultural context. In doing so, it offers a refined lens for tailoring support strategies to the context, aligning with the patient-centered ethos advocated in the CSACI guidelines 26 and advancing child-centered ideals foundational to the ODSF.12,26
Limitations
This study offers preliminary insights from a qualitative exploration of the OIT decision-making process in Japan, but has several limitations.
First, its exploratory nature and relatively small sample size (N = 14), with only 3 child participants, limited the ability to reach thematic saturation, especially from the perspective of children. This may have constrained the depth and variability of the insights into children's experiences. In addition, the child participants were concentrated in a narrow age range, which further restricted the diversity of the developmental perspectives captured. Second, the inclusion of heterogeneous stakeholders—patients, parents, physicians, and nurses— provides valuable diversity and complicated interpretations. The mixing of roles with different positions and responsibilities may have blurred subgroup-specific experiences, limiting the precision of the thematic analysis. Third, the predominance of female participants, particularly mothers, may have introduced a gender-related bias. Mothers’ perspectives were strongly represented, while fathers’ perspectives were not. This imbalance could have influenced the interpretation and restricted the transferability of the findings to broader populations.
Finally, reliance on participants from specific institutions and single-time-point interviews limited generalizability. Moreover, recruitment during the COVID-19 pandemic may have influenced the sample composition.
Conclusion
Using the ODSF, this study identified 3 priorities in pediatric OIT decision making in Japan: balancing safety, burden, and values; elevating children's voices; and addressing gaps in support. These findings inform the development of a culturally adapted DA that highlights the importance of child participation and context-sensitive support. Future research with larger and more diverse samples is needed to refine and validate this model and to advance child-inclusive SDM in Japanese clinical practice. These contributions reinforce culturally sensitive, child-centered decision support in Japan and inform pediatric SDM internationally.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251406346 - Supplemental material for Patient and Family Experiences and Support Needs in Pediatric Oral Immunotherapy Decision Making: A Multi-Stakeholder Qualitative Study in Japan
Supplemental material, sj-docx-1-jpx-10.1177_23743735251406346 for Patient and Family Experiences and Support Needs in Pediatric Oral Immunotherapy Decision Making: A Multi-Stakeholder Qualitative Study in Japan by Junko Hayama, Kanako Yamamoto, Kota Hirai, Koichi Yamaguchi, Hiroyuki Mochizuki and Kazuhiro Nakayama in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735251406346 - Supplemental material for Patient and Family Experiences and Support Needs in Pediatric Oral Immunotherapy Decision Making: A Multi-Stakeholder Qualitative Study in Japan
Supplemental material, sj-docx-2-jpx-10.1177_23743735251406346 for Patient and Family Experiences and Support Needs in Pediatric Oral Immunotherapy Decision Making: A Multi-Stakeholder Qualitative Study in Japan by Junko Hayama, Kanako Yamamoto, Kota Hirai, Koichi Yamaguchi, Hiroyuki Mochizuki and Kazuhiro Nakayama in Journal of Patient Experience
Footnotes
Acknowledgments
The authors wish to express their sincere gratitude to the children, parents, and healthcare professionals who generously participated in this study and shared their valuable experiences regarding OIT decision making.
Author Contributions
JH: conceptualization, methodology, investigation (led interviews and data collection), formal analysis (led qualitative analysis), writing the original draft, writing the review, and editing. KY: formal analysis (supporting qualitative analysis and interpretation), supervision, writing, review, and editing. HK: supervision, writing, review, and editing. KN and HM: supervision, writing, review, and editing (critical review).
Consent to Participate
All adult participants and parents of the children provided written informed consent before their participation in the study. Children provided written or verbal assent appropriate for their age and understanding before participating in the interviews. The participants were informed that they could withdraw from the study at any time without penalty.
Consent to Publication
This manuscript does not contain any individual data in any form that would require specific consent for publication (eg, identifiable images or videos). All participant data (eg, quotes) were anonymized to protect confidentiality.
Data Availability Statement
Due to the sensitive nature of the interview data involving a small number of child participants, and to maintain their anonymity and confidentiality, raw data (transcripts) are not publicly available. These key findings are supported by the anonymized quotes presented in this article. The interview guides used in this study are available as Supplemental material.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical approval was obtained from St Luke's International University (No. 19A-086) and the Tokai University School of Medicine (No. 19R-272). Participation was voluntary, and the data were anonymized.
Funding
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI (Grant No. 24K13911).
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.