
Abstract
Telemedicine is a growing treatment modality for opioid use disorder and can offer greater privacy, flexibility, and agency to patients who have experienced stigmatizing behavior in other treatment settings. Designing a welcoming and respectful virtual environment is one mechanism for creating a patient-centered experience, yet to date, patient preferences for telemedicine treatment for opioid use disorder have not been evaluated. We conducted a cross-sectional study to assess patient perspectives on Zoom backgrounds and provider attire among individuals receiving telemedicine treatment for opioid use disorder at a multi-state practice. A total of 601 patients participated in the study, of whom 60.4% were female and the average age was 41.4 years. Nearly 60% of respondents preferred real backgrounds during virtual visits. The majority of respondents did not have a preference for provider attire with the remaining respondents preferring casual attire to business casual or formal attire. Overall, we found that individuals with opioid use disorder prefer authenticity in backgrounds and personalized attire to establish trust and open communication in telemedicine.
Introduction
Opioid use disorder remains a critical public health challenge in the United States with opioid-related overdose causing 24 deaths per 100,000 persons in 2023, up from 14.6 deaths per 100,000 in 2016. 1 During the COVID-19 pandemic, the percentage of deaths attributable to unintentional opioid toxicity rose to over 20% of deaths among 20- to 39-year-old adults in the United States. 2 Policy changes during this time such as the Coronavirus Aid, Relief, and Economic Security Act and the Drug Enforcement Administration prescribing flexibilities facilitated virtual visits to treat opioid use disorder and allowed buprenorphine to be prescribed through telemedicine treatment.3,4 Between January 2020 and 2021, the availability of telemedicine appointments for substance use treatment increased 143%, and as of 2023, 6.2% of individuals with a substance use disorder accessed care via telemedicine.5,6
In telemedicine treatment for opioid use disorder, patients attend virtual visits through an app-based platform with advanced practitioners, collaborating physicians, medical assistants, licensed clinical social workers and therapists, certified peer recovery specialists, and patient navigators. 7 Medical providers can prescribe medications such as buprenorphine or naltrexone for at-home initiation or to continue medication treatment initiated in another setting.7,8 Studies have shown telemedicine is associated with high patient satisfaction as well as reduced likelihood of fatal overdose from opioid use and decreased hospitalizations.7,9,10 Furthermore, telemedicine bypasses common barriers to in-person care like privacy concerns and externalized stigma while emphasizing patient-centered care for individuals with opioid use disorder. Additionally, patients who face long waitlists to see a local in-person provider for opioid use disorder treatment can receive care from a telemedicine provider with greater availability preventing treatment delays. 11
The first 6 months of treatment for opioid use disorder are a critical period in care during which patients establish use of and stabilize on medications for opioid use disorder. 12 As a result, it is important that telemedicine treatment programs for opioid use disorder facilitate a welcoming and respectful virtual environment to support patient engagement in the early months of treatment. Thoughtful curation of the way providers present to patients is one mechanism through which telemedicine practices can create a non-judgmental patient-centered experience. A single study previously evaluated patient preferences for virtual backgrounds in outpatient visits within an academic health system and found a preference for backgrounds depicting a physician's office, particularly views showing physician credentials. 13 Additionally, a survey of U.S. patients found providers wearing white coats were viewed as more professional and that patients preferred that family physicians wear business attire with white coats. 14 However, to date, patient preferences for the virtual environment of telemedicine treatment for opioid use disorder specifically have not been evaluated despite the importance of the virtual design in establishing an open, collaborative space for opioid use disorder treatment. Given this gap in the literature, we aimed to evaluate patient preferences for and perceptions of provider attire choices, backgrounds, and name displays in telemedicine treatment programs for opioid use disorder.
Method
Participants
We conducted a cross-sectional study evaluating patient preferences for telemedicine design, among other outcomes related to patient satisfaction and care quality. The survey was conducted among patients residing in rural and non-rural areas enrolled in telemedicine treatment for opioid use disorder at a multi-state telemedicine practice, the care model of which has been described previously. 8 Patients were eligible to participate in the study if they were (1) aged 18 or older, (2) had a clinical diagnosis of opioid use disorder (3) resided in Michigan, Ohio, New Jersey, Florida, or Texas, (4) enrolled with a valid zip code, and (5) completed an initial medical evaluation and a follow-up medical appointment.
Sampling and Study Implementation
We mapped patient zip codes to 2010 Rural Urban Commuting Area (RUCA) codes to create sampling strata for patients living in rural areas defined as RUCA codes 4-10 and non-rural areas defined as RUCA codes 1-3. 15 Eligible patients were randomly selected from electronic health records to receive a study invitation by rural stratum and invited in two waves to create a balanced cohort targeting 600 patients representing rural and non-rural areas. The representation of rural and urban participants was intentionally balanced to allow for comparative analyses related to other assessments in the study.
Eligible patients received an initial invitation to complete the assessment through email followed by reminders to participate sent via email and text messages over 2 weeks. The study was administered through JotForm, an online survey development platform, and contained 80 questions. State of residence and engagement in treatment for opioid use disorder at the practice were confirmed through eligibility screening questions and informed consent to participate was collected at the start of the assessment. Participants received a $20 Amazon e-gift card delivered via email as compensation for their time and effort. This study was reviewed and approved by an independent institutional review board (Solutions IRB, Protocol #536).
Measures
Participants self-reported demographic information covering age, sex, race, ethnicity, education, employment status, and housing type. Other self-reported health history information was collected measuring years of opioid use, months in treatment, prior inpatient substance use or mental health treatment, other diagnosed substance use disorders, and diagnosed chronic health conditions including chronic pain, anxiety, depression, and hepatitis C.
Participants selected their preference for Zoom backgrounds and provider attire during virtual visits overall and by visit characteristics using the images shown in Appendix A. The background images featured providers in Zoom using a real home background, a virtual office background, and a virtual organizational background and the provider attire images featured providers in casual, business casual, and formal clothing. Participants were also asked to select which background and attire design made (a) it easiest to trust their provider, (b) their visit feel most welcome, (c) their visit feel the most private/confidential, (d) it easiest to communicate with their provider, and (e) the provider feel the most professional. Participants also provided preferences concerning name displays.
Analysis
We calculated the mean and standard deviation for age and counts and percentages of participants for all categorical variables describing demographics and health history. We also measured frequencies and proportions of patients who preferred each background and attire option overall and by visit characteristics. Analyses were conducted using Stata (Version 18, College Station, Texas).
Results
Six hundred and one patients in telemedicine treatment for opioid use disorder completed the online assessment out of 1800 invited (33.4%) (Table 1). The average age of respondents was 41.4 years (SD 8.6), 60.4% of respondents were female (n = 363), and 90.4% of respondents identified as White (n = 534). The sample was evenly balanced representing patients in rural and non-rural areas with 301 rural participants (50.1%) and 300 non-rural participants (49.9%). Over half of participants reported previously receiving inpatient treatment for substance use or mental health (57%; n = 334).
Summary Characteristics of Adults with Opioid Use Disorder.
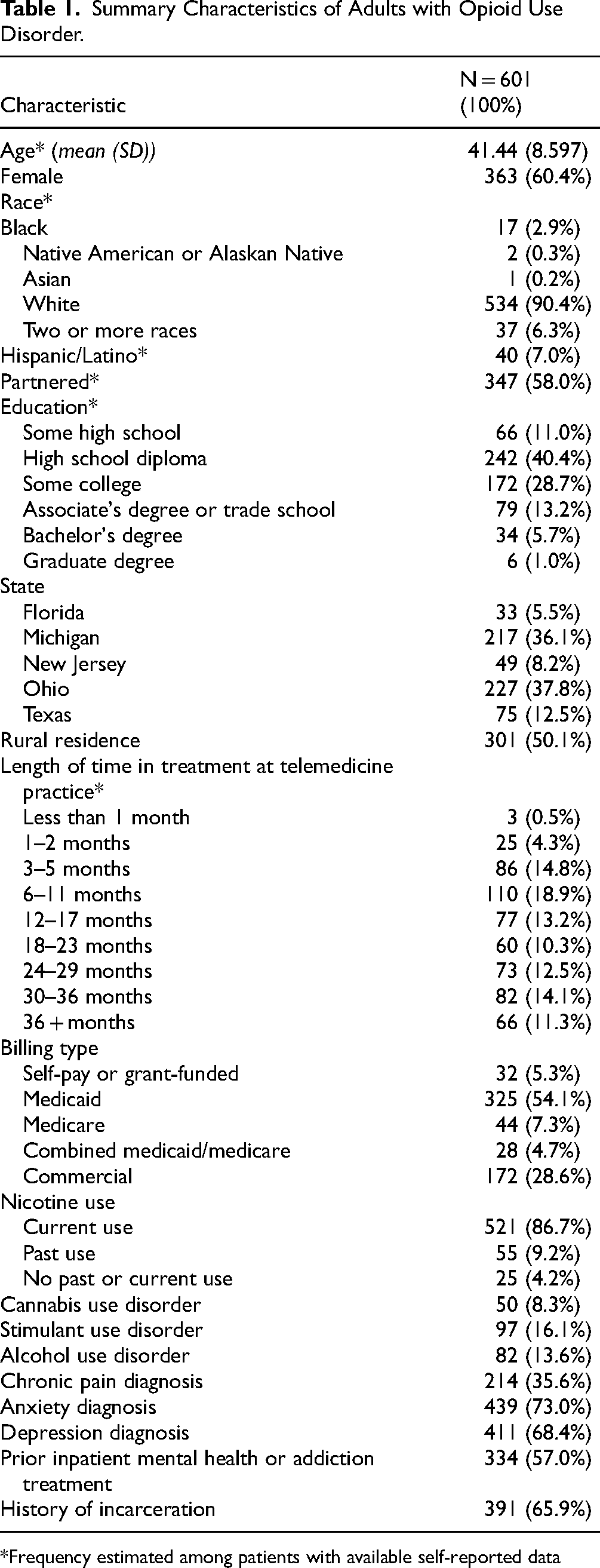
Frequency estimated among patients with available self-reported data
Overall, 58.9% of respondents preferred using real backgrounds during virtual visits (n = 354) compared to 15.0% (n = 90) who preferred an office virtual background. Less than 10% were in favor of an organizational virtual background (7.5%; n = 45), and 18.6% (n = 112) stated no preference (Table 2). Participants preferred real backgrounds across the visit characteristics assessed (Figure 1). Approximately 68% (n = 411) of participants reported real backgrounds made them feel the most welcome and 67.7% (n = 408) reported real backgrounds made it easiest to communicate with providers. Similarly, 62.7% (n = 377) of participants felt using a real background during visits made it easiest to trust their provider and 61.9% (n = 372) of respondents felt a real background made their visit feel the most private.

Zoom background and provider attire preferences among individuals receiving telehealth treatment for opioid use disorder.
Patient Preferences for Telemedicine Design.
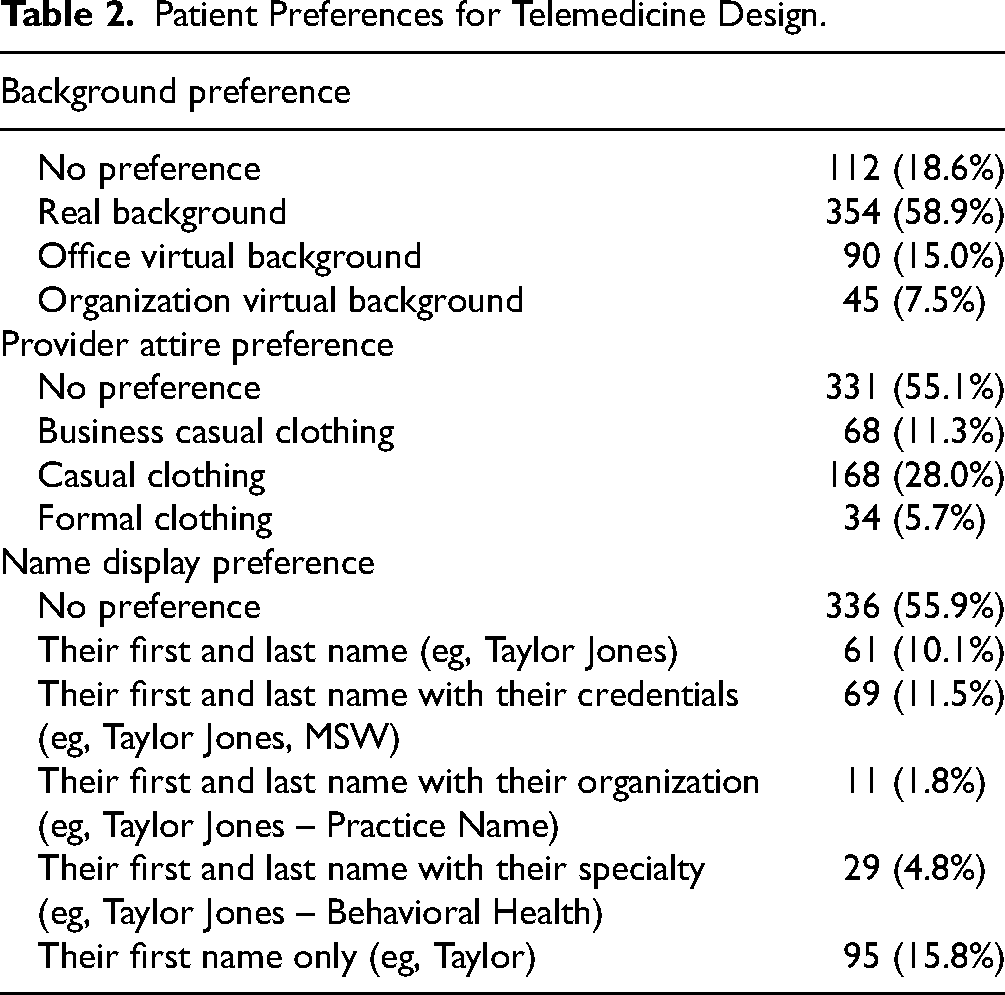
A majority of participants (55.1%, n = 331) did not have a preference for provider attire during visits with the remaining respondents preferring casual attire (28.0%, n = 168), business casual (11.3%, n = 68), and formal attire (5.7%, n = 34) (Table 2). Of the three attire options, casual clothing was preferred in terms of creating a supportive virtual environment. Approximately 66% of participants felt casual attire made it easier to trust their provider (n = 394) and 69.4% felt visits would feel more welcoming with providers in casual attire (n = 417) (Figure 1). In terms of professionalism, 45.4% of participants (n = 273) felt casual attire made their provider feel the most professional compared with only 24.3% of participants (n = 146) who felt formal attire made providers feel the most professional. Finally, 55.9% of respondents (n = 336) expressed no preference for a provider's name display in a virtual visit, but 15.8% (n = 95) preferred providers display only their first names, followed by first and last name with credentials (n = 69, 11.5%) and first and last name without credentials (n = 61, 10.1%).
Discussion
Our study found that patients receiving treatment for opioid use disorder through telemedicine favored the use of real backgrounds by providers during virtual appointments. Most patients did not have a preference for the attire worn by their provider, but those patients who did favored casual clothing that humanized their interactions with clinicians within a virtual environment.
Our findings differ from other studies, which have found that patients prefer virtual backgrounds depicting physicians’ offices alongside professional attire. Houchens et al found backgrounds showing a provider's home spaces were significantly less preferred by patients in virtual outpatient visits, 13 yet our sample favored seeing a provider's real environment over a virtual screen. Xun et al also found patients preferred formal attire by physicians to create a professional setting, 14 whereas patients in our sample either did not have a preference or felt casual attire was more professional and created a more supportive environment.
The large percentage of respondents who reported no preference for provider attire in virtual visits for opioid use disorder treatment could be interpreted in multiple ways. First, patients may feel other characteristics of their providers such as their mannerisms and tone of voice during visits are more impactful than attire in creating a welcoming environment. Secondly, patients may report no preference because they find only a part of a provider's outfit is normally visible within a video frame limiting its impact on their encounters. Finally, a lack of preference for provider attire may reflect patient flexibility and a desire for providers to be able to select attire that best represents their approach to care.
Nevertheless, our findings highlight that many individuals with opioid use disorder prefer authenticity in backgrounds and attire to establish trust and open communication in telemedicine.16,17 Many patients with opioid use disorder report feeling shame and anxiety about seeking treatment in shared public spaces and value the privacy offered in attending appointments from home. 16 The preference for providers to use a real background during virtual visits for opioid use disorder treatment may reflect a desire to ensure telemedicine encounters remain private. Additionally, some patients with opioid use disorder have experienced challenges in in-person care settings that utilize strict requirements for medication compliance and punitive measures for missed appointments or positive drug screens. 17 As a result, real backgrounds and casual provider attire may help establish a more collaborative and less authoritative role for providers as partners in the patient's recovery journey.
A systematic review by Petrilli et al emphasized patient preferences for physician attire varied greatly by clinical care type and patient demographics and promoted the use of tailored strategies for provider attire to fit the treatment context. 18 A participatory co-design process with patients with opioid use disorder as designers could create a more simple, relaxed setting for patients with previous negative experiences in formal in-person care settings. 19 Additionally, using patients as designers in the creation and implementation of telemedicine care models could improve telemedicine for individuals who experience anxiety, shame, or fear accessing and utilizing in-person healthcare services. Future co-design research in this area is important to understand the unique preferences of patients in these populations. Patient input could be integrated into practical interventions such as the creation of a set of standards for virtual backgrounds in telemedicine treatment settings.
Limitations
This study examined the telemedicine design preferences of patients enrolled in treatment at a single practice operating across five US states, which may not reflect the preferences of patients residing in other geographic areas. The majority of participants were female who are more likely to utilize telemedicine for substance use disorder treatment compared to male patients. The preferences of our sample may differ from populations in other treatment settings with greater representation of male patients. Finally, over 90% of participants were White and given significant unmet need for opioid use disorder treatment among Black, Asian, American Indian, and Hispanic persons, future research to illuminate their telemedicine design preferences may support greater opportunities for future telemedicine engagement. 20
Conclusions
Individuals engaging in telemedicine treatment for opioid use disorder value an authentic personable virtual visit environment featuring real backgrounds and personalized provider attire. Ultimately, visually creating a welcoming, non-judgmental patient experience through attire and background selection represents a new opportunity for telemedicine providers to engage patients in care. Telemedicine providers should consider the specific psychosocial needs of their patient population and curate their virtual presentation during visits in recognition as an extension of patient-centered care. Involving patients as partners in telemedicine design could improve care for populations beyond those included in this study, and future research is needed to understand their patient preferences and translate them into actionable interventions.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251361584 - Supplemental material for Virtual Backgrounds, Clinician Attire, and Patient Experience Preferences Among Individuals Receiving Telemedicine Treatment for Opioid Use Disorder
Supplemental material, sj-docx-1-jpx-10.1177_23743735251361584 for Virtual Backgrounds, Clinician Attire, and Patient Experience Preferences Among Individuals Receiving Telemedicine Treatment for Opioid Use Disorder by Marlene C Lira, Lauren E Hendy, Amanda Olguin, Cynthia Jimes, Clare Mulford, Karisa Davis, Daniel Banks and M Justin Coffey in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735251361584 - Supplemental material for Virtual Backgrounds, Clinician Attire, and Patient Experience Preferences Among Individuals Receiving Telemedicine Treatment for Opioid Use Disorder
Supplemental material, sj-docx-2-jpx-10.1177_23743735251361584 for Virtual Backgrounds, Clinician Attire, and Patient Experience Preferences Among Individuals Receiving Telemedicine Treatment for Opioid Use Disorder by Marlene C Lira, Lauren E Hendy, Amanda Olguin, Cynthia Jimes, Clare Mulford, Karisa Davis, Daniel Banks and M Justin Coffey in Journal of Patient Experience
Footnotes
Acknowledgements
The authors would like to acknowledge Alaine Sepulveda and Jaclyn Jutras for their support organizing survey implementation and data collection.
Author Contributions
MCL contributed to conceptualization, methodology, data collection, formal analysis, writing—review and editing, funding acquisition, and supervision. LEH contributed to conceptualization, methodology, data collection, software, formal analysis, writing – original draft, and writing—review and editing. AO contributed to conceptualization, methodology, data collection, and writing—review and editing. CJ contributed to conceptualization, methodology, data collection, writing—review and editing, and funding acquisition. CM contributed to conceptualization, methodology, and writing—review and editing. KD contributed to conceptualization, methodology, data collection, and writing—review and editing. DB contributed to conceptualization, methodology, data collection, and writing—review and editing. MJC contributed to conceptualization, methodology, writing—review and editing, and funding acquisition.
Data Availability Statement
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of substance use-related research, supporting data is not available.
Declaration of Conflicting Interest
MJC and ML are equity owners in Workit Health. MJC receives author royalties from UpToDate and Medlink Neurology unrelated to this work. The remaining authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
This study was approved as human subjects research through an independent institutional review board (Solutions IRB #0432). All participants provided written informed consent prior to enrollment in the study
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Health Resources and Services Administration (HRSA), Department of Health and Human Services (HHS) provided financial support for programming described in this publication. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and decision to submit the manuscript for publication. The funder had a limited role in the review and approval of the manuscript. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of HRSA or HHS.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.