
Abstract
While studies have evaluated the utility of telehealth in replacing in-person clinical encounters, there is a dearth of literature examining the quality of patient-physician communication with telehealth encounters. Accordingly, this study assessed the feasibility of using virtual cardiology clinical encounters to examine patient-physician interaction, communication, and perceptions of the clinical encounter. Telemedicine cardiology clinical encounters were audio- and video-recorded following the encounter, patients, and cardiologists completed an electronic survey to assess perceptions of the encounter. Qualitative analysis of the communication and statistical analysis of the survey data was conducted, providing descriptive data. The study included 11 patient-physician dyads; all patients were non-Hispanic White. Cardiologists were more racially and ethnically diverse (63% Asian). Most patients agreed telemedicine was comparable to in-person encounters (85.7%), with all cardiologists reporting that patients appeared satisfied with the encounter. We utilized an assessment tool to examine patient-physician communication in the recorded virtual encounters. This study suggests examining patient-physician communication using virtual clinical encounters is feasible, although there are barriers that need addressing for larger studies.
Keywords
Introduction
Effective communication between patients and their clinicians is essential to sustain a successful, trusting patient-physician relationship. 1 Delivering patient-centered care requires a fundamental understanding of the person beyond their medical condition, encompassing experiences, values, and preferences. 2 Good patient-physician communication has been associated with improved health outcomes, fewer malpractice complaints, improved medication adherence, and reduced healthcare costs.2–4 Additionally, tailored training in communication skills yields improved patient satisfaction and outcomes. 5 However, there is a notable contrast between physicians' and patients’ perceptions regarding communication; in fact, the majority of physicians thought their communication skills with patients were effective, while only 21% of patients were satisfied with the communication with their doctors. 6 Evaluation of patients’ satisfaction in communication has consistently emphasized the desire for improved communication with physicians. 4
As the dynamics of healthcare delivery continue to shift, the depth of patient-physician interaction and overall quality of care have been impacted. 5 Some of these changes have led clinicians to experience reduced satisfaction, a diminished focus on patient care, and potentially elevated risks of burnout and malpractice, which can ultimately contribute to negative perceptions of patients.6–9 Consequently, patients find themselves playing a diminished role in the relationship, experiencing a sense of disconnection, frustration, and even self-blame.10,11
Digital transformations such as patient portals, remote monitoring at home, and telemedicine have aimed to enhance communication between patients and health professionals, provide patients with the means for self-care, facilitate self-education, and thus foster patient-centered healthcare.10–13 Comparisons of synchronous video consultations to in-person encounters find the majority of patients express satisfaction with the quality of healthcare they received through telemedicine as well as a strong willingness for future engagement in telemedicine visits.13–15
The importance of assessing effective communication skills in doctor-patient relationships has been emphasized throughout medical education as well as postgraduate clinical practice. 16 However, clinicians may not be equipped to adapt these skills to telemedicine encounters and may have concerns about the efficacy of telemedicine. While there has been a focus on evaluating patients’ perception of telehealth visits, 17 little has been done to objectively examine patient-clinician communication during telehealth visits. This study sought to assess patient-provider communication during cardiology telemedicine clinical encounters (Tables 1 and 2).
Patient Demographics and Perceptions Regarding Telehealth Visit.

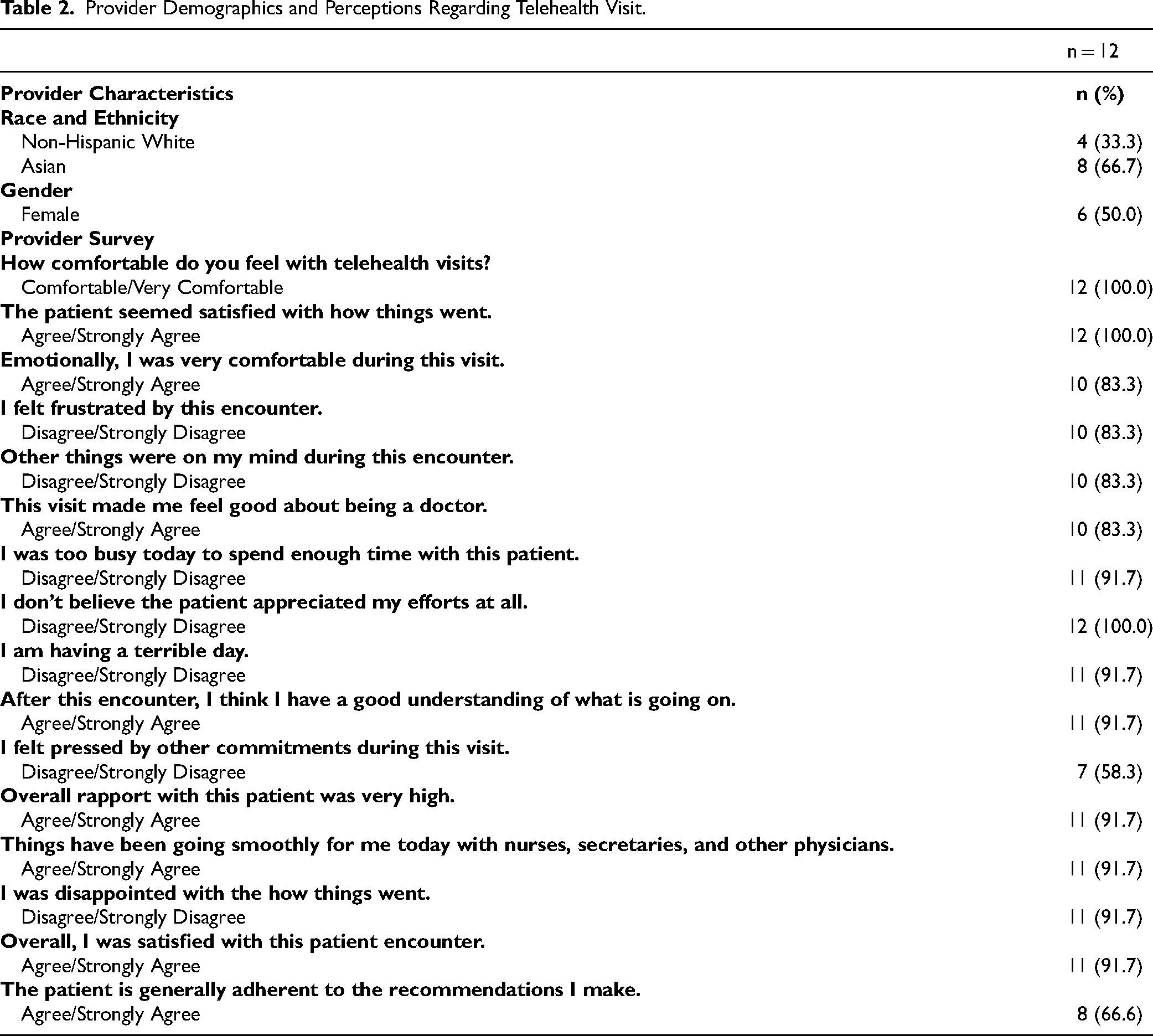
Provider Demographics and Perceptions Regarding Telehealth Visit.
Methods
The Mayo Clinic Institutional Review Board approved this study (#22-010489). Participating cardiologists were selected based on the monthly telemedicine visit volume at the Mayo Clinic Department of Cardiovascular Medicine. Any cardiologist with more than 5 telemedicine visits per month was approached by the study team to introduce the study. If the cardiologist expressed interest, they were recruited by the study team. Participants with upcoming telemedicine visits scheduled with one of the consented physicians were phoned by the study coordinator and asked to participate in the study. A notification email was sent to the practicing physician upon consent, and a reminder email was sent the day prior and the day of the appointment. A video recording of the telemedicine visit was performed. Following the visit, the physicians and patients completed an electronic survey to assess perceptions of the clinical encounter (Appendix Tables A1 and A2). The patients and physicians received weekly reminders to complete the survey for 3 weeks. The survey data and Calgary-Cambridge Global Consultation Rating Scale (CC-GCRS) data were collected and managed using the HIPAA-compliant Research Electronic Data Capture System (REDCap) hosted at Mayo Clinic Arizona.
Study Procedures
Before assessing clinical encounters, an understanding of the microskills was necessary, as the scoring system was based on the analyst's ability to identify microskills. To examine barriers and opportunities to improve the study, the core study team met weekly for debriefs and recorded meeting minutes. The study team also had a debrief at the end of data collection to identify barriers encountered during the study.
CC-GCRS and Assessments
The Global Consultation Rating Scale (CC-GCRS) is an assessment tool used to evaluate a physician's competency in communicating with patients during clinical encounters. The CC-GCRS evaluates effective patient-physician communication skills and to present an evidence-based structure for its analysis and teaching. 3 The scale covers 9 domains: initiating the session, gathering information, building a relationship, providing structure, providing the correct information, aiding accurate recall and understanding, achieving a shared understanding, planning shared decision making, and closure. The assessment scores adopted a modified scoring convention provided by Iversen et al, 18 for the demonstrated microskills.
Appendix Table 3 represents the codebook with the overview of criteria for scoring based on the items in CC-GCRS. The item that assessed the nonverbal communication between the cardiologists and the patients was eliminated due to the difficulty in assessing nonverbal communication between 2 other people via video. The scores ranged from 0 to 44.
Perceptions of the Encounter
Following the visit, cardiologists and patients completed an electronic survey adapted from previously validated instruments to examine their perception of the encounter (see Appendix Table 2). The patient survey (27 total questions) included questions from Rose et al focusing on digital health and included 3 scales: overall satisfaction (eg, my virtual visit made it easy to get the care I needed), comfort and ease using virtual technology (eg, I was comfortable using my virtual platform), patient-clinician engagement (eg, my online health care provider was interested in me as a person), with good psychometric properties (Cronbach's alpha 0.89-0.93). Additional items were included to assess technology equity (eg, “I have access to a smart mobile device or a laptop computer”; “I am proficient at using smart devices”). The survey for cardiologists (21 total questions) included questions from the Patient Satisfaction Scale (Shore and Frank, 1986) (eg, “The patient seemed satisfied with how things went”; “I helped this patient today”) which also demonstrated good psychometric properties (Tables 3 and 4). 19
CC-GCRS Scores.

Modified scoring convention from Iversen et al, 2020.
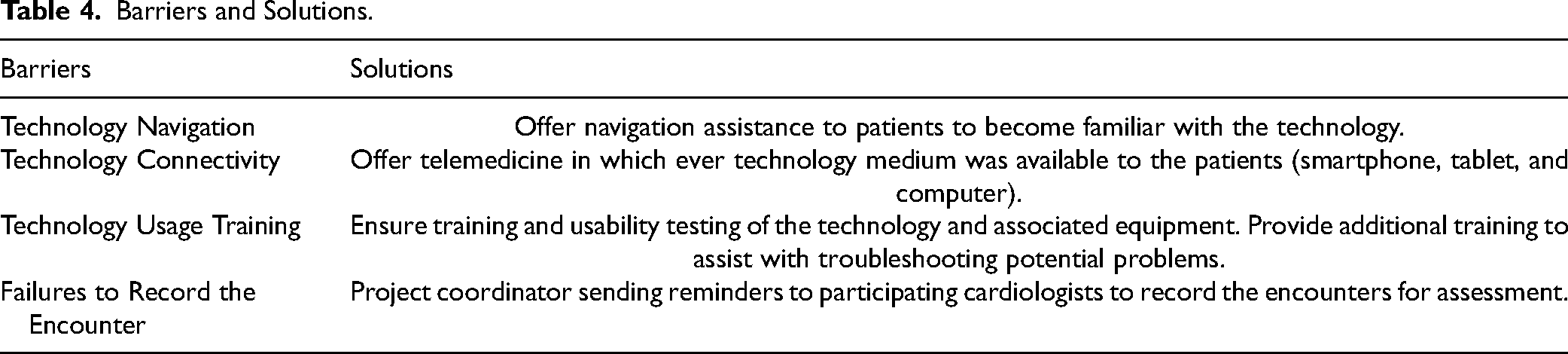
Barriers and Solutions.
Statistical Analysis
The qualitative analyst assessed patient-clinician communication using the existing coding systems described above. Following the assessment, the analyst conducted several rounds of active listening. The analyses included field notes of individual ideas and observations, other relevant ideas, and concepts. The analyst then identified significant statements within each encounter, which was instrumental in the development of the codes. Coding was done directly from the recordings without transcription. The themes that emerged from the encounters were the combination of field notes, brief codes, and observations, and the exerts that best fit those themes.
Survey data and CC-GCRS data were stored using REDCap hosted at Mayo Clinic (Harris et al, 2009). 20 Descriptive data is provided from the analyses of patient and clinician surveys, including overall patient and clinician perceptions of their encounters. All analyses were conducted using R version 4.0.3 or later (R Core Team, 2021).
Results
There were 11 patient-physician dyads included in the study. Of 21 clinicians contacted, 45% expressed interest in the project, and among these, 30% consented to participate. Of the 100 patients approached to participate, 24 (24%) patients consented. Six patients withdrew from the study: the first 4 patients due to recording issues at the beginning of the study, one patient due to the visit no longer being a telemedicine visit, and the last patient because the patient needed to reschedule outside the study timeline. All 11 patients were non-Hispanic White with a mean age of 57 years of age (SD = 15); with 6 (55%) identifying as female. Of the 11 cardiologists, 4 (33%) were non-Hispanic White, with 8 (67%) identifying as Asian, with 6 (50%) identifying as female.
Patient and Cardiologist Perceptions
Of the 11 patients, 7 (63%) completed the patient survey. Of those, 6 (86%) did not have a previous in-person visit with the cardiologist caring for them during the telemedicine visit. Five (71%) connected for the visit using a mobile device. Six (86%) agreed or strongly agreed that the telemedicine visit made it easy to get the care they needed, and the same proportion agreed or strongly agreed the telemedicine visit was as good as an in-person visit for their health concern and saved them time The overall perception of the telemedicine visit was positive: the technology was easy to use (n = 10; 90.9% strongly agreed), patients felt comfortable using the patient portal (n = 9; 81.8%), it was easy to see (n = 8; 72.7%) and hear the cardiologist (n = 9; 81.8%), and patients felt the cardiologist understood their health concerns (n = 9; 81.8%; Table 1). There were 8 cardiologists that responded to the survey. Of those who responded, all reported being comfortable or very comfortable with telemedicine visits and agreed or strongly agreed the patient seemed satisfied with how the visit went. Seven (88%) agreed or strongly agreed the patient had a good understanding of what was going on after the encounter, that overall rapport with the patient was high, and that they were satisfied with the patient encounter. A high proportion agreed or strongly agreed they were emotionally comfortable during the visit (n = 6, 75%) and disagreed or strongly disagreed that they felt frustrated by the encounter (n = 7, 86%). All respondents disagreed or strongly disagreed that they were too busy to spend enough time with the patient, and 4 (50%) disagreed or strongly disagreed they felt pressed by other commitments during the visit (Table 1).
Calgary-Cambridge Global Consultation Scale
The mean scores for each domain (with a potential range from 0 to 4, with higher scores indicating more skill) included initiating the session (3.72), identifying the problem (4.00), exploring the problem (4.00), gathering the patient's perspective (4.00), developing rapport (3.09), providing structure (3.63), providing the correct information for the individual patient (4.00), aiding accurate recall and understanding (3.18), achieved a shared understanding (3.81), planning shared decision making (4.00), and closure (4.00).
Telemedicine Encounters
The length of the 11 encounters varied from 6 to 84 min (median = 53.0 min; IQR = 27.8 min). Although there was variation in the length of encounters, conversations with the cardiologists allowed time for patients to ask questions and give their perspectives on integral parts of their individual patient histories, which became an essential part of the telemedicine encounter. The following excerpts from the telemedicine encounters allow the natural flow of conversation between the cardiologists and patients. Three of the major themes that were flushed from the telemedicine encounters were (1) patient-centered communication, (2) patient engagement, and (3) health literacy. Telemedicine encounter exerts that best fit the themes that have been selected.
Patient-Centered Communication
Patient-centered communication was apparent during the telemedicine encounters, with the participating cardiologists allowing the patients the opportunity to drive the conversation and respond to questions, without the cardiologist leading or interrupting the conversation.
An example of patient-centered communication between the cardiologist and the patient is as follows: Cardiologist: “I would like to make sure we go over all the questions that you have, so maybe we’ll start with that?” Patient: “I have so many questions. The first is maybe just a procedural thing. I was wondering if you got the renal and carotid ultrasounds that were done in the hospital last November. I have so many questions I want to ask you, that I have them in categories, and then I flagged the ones that were most important.” Cardiologist: “Awesome, so how about you give me kind of a sense of what the categories are, go through them, I’ll probably have to ask you some questions as well, then we’ll meet in the middle.” Patient: “Ok, well so there are 3 categories: treatment and testing, odd symptoms I have that I want to see are related, then I have just a random set of questions.”
Effective Patient Engagement
Patient engagement was recognized during the encounters in the form of early and continuous integration of the patient's understanding or perspectives on their individual health.
21
An example of patient engagement between the cardiologist and the patient is as follows: Cardiologist: “Are you physically active? What do you do on a weekly basis?” Patient: “Well I walk. I do weights, I do some stretching, yoga, I swim a little bit.” Cardiologist: “You try and do something active most days of the week?” Patient: “Yeah, I would say almost 7 days a week. I went on a statin, 10 mg, and I went off for 6 months, and my doctor thought that I wouldn’t see a benefit and I just went back on it. When I came to Mayo, the doctor told me to go back on it. I’m interested in getting your advice on it cause I’ve done some studying and reading about statins, including this book that says that cholesterol isn’t the villain that everyone thinks it is.” Patient: “When I switched a plant-based diet, inevitably a low-fat diet. I actually started cutting out and cutting back on oil and things like that. I’m just wondering if I should be concerned about healthy oils. I’m pretty disciplined in my diet, so I know that if there is something that I should be tweaking, I will do it.”
High Health Literacy
In each of the notes from the encounters, the analyst noted that there was clear use of medical jargon by the cardiologists. However, the analyst also noted that this was acceptable due to the unsolicited use of medical jargon by each of the patients that assisted them in recall and understanding of their individual conditions. The patients within this study were very knowledgeable of their individual conditions and could ask and answer questions utilizing complex language. The high levels of health literacy exhibited by the patients during the telemedicine encounters were a mixture of understanding individual health and healthcare needs, using the health information to participate in the healthcare system, and maintaining a working relationship with the cardiologist during the telemedicine encounter.
22
Examples of high health literacy during the telemedicine encounters were as follows: Patient: “How to I increase my LDL? How do I increase that HDL particle size?” Cardiologist: “I know that they have you on Coumadin, how long do they plan on keeping you on that?” Patient: “They said at least 6 months, so that would bring us up to March. I know the one in my heart (blood clot) is gone now, and tomorrow I’m actually getting an updated ultrasound on the one in my femoral artery.” Cardiology: “With your family history and everything I was wondering had you been worked up for hypercoagulable state?” Patient: “My clots they mentioned were a side effect of the ECMO, cause they were exactly where they thought they’d be.”
Discussion
Based on the assessment scores of the encounters, the clinicians were found to be utilizing a considerable patient-centered approach with patients. The patient-centeredness observed included respecting and responding to the patient’s care requirements, preferences, and beliefs in the clinical decision-making process, which are recognized values by the National Academy of Medicine. 23 Health literacy embodies the social and cognitive skills that establish the motivation and ability of individuals to acquire access to, understand, and use health information in ways that encourage and maintain good health. 24 Although there were some instances where medical jargon was used, the patient population was highly health literate and engaged, showing no confusion with the use of medical jargon, often driving the conversations reciprocating medical jargon during the telemedicine encounters.
Patient-centered communication is embraced as being vital to quality healthcare that centers patients’ preferences and values, and is associated with adherence to healthy lifestyles, improved clinical outcomes, better quality of life, and reduced rates of undesirable affects. 25 The investigative team also noted the patients’ understanding of their health history and condition, along with the communication skills to verbally address comments, make suggestions, and ask questions allowed them to be active participants in the treatment and management of their conditions. That 2-way dialogue observed between the patients and cardiologists is essential for the cardiologists to be responsive to their patients’ health concerns. 23 There is widespread agreement that patient engagement should be meaningful and impactful, and has been frequently used interchangeably with patient involvement, patient activation, and even patient-centered care. 26 When clinicians communicate in a patient-centered way, it fosters patient engagement in the information the patient and provider bring to the encounter and allows both parties to reach a shared understanding. 27
Limitations
There were several limitations in this study. The first limitation was the observed 45% response rate and 30% consenting rate among cardiologists. Retention also proved challenging despite patients and cardiologists receiving surveys immediately following the encounter electronically, along with automated reminders. Relatedly, patients and cardiologists do not reflect the demographics of the United States, and this study was conducted at a single institution, all limiting generalizability. In addition, there was the potential for selection bias, with those patients and clinicians most comfortable with technology perhaps being more likely to participate. The high levels of health literacy noted may also reflect selection bias. Future studies should consider how best to obtain a representative sample of patients (and clinicians) with varied technological expertise and health literacy. The completion rate for the surveys and recordings could also be improved. To successfully conduct this study on a larger scale, more time would be necessary to inform and consent cardiologists as well as more training and information will be needed for physicians to record and share recordings.
Future Directions
The investigative team is currently developing a more robust study that will address barriers to effective communication during telemedicine encounters for more diverse patient populations (race, ethnicity, age, SES, and primary language). Understanding how diverse patients interact and respond to physicians and other clinicians during telemedicine encounters will allow the study team to analyze the patient encounters at multiple points to determine the quality of communication between clinicians and patient populations with varying levels of communication styles and health literacy. This study will allow the investigative team to examine potential differences in patient-clinician relationships by patient demographics while minimizing the Hawthorne effect.
Conclusions
This study examined the feasibility of evaluating patient-centered patient-physician communication with experienced cardiologists during telemedicine visits. Telemedicine added a level of complexity to creating and maintaining patient-centeredness but had little impact on the participating patients’ satisfaction with the telemedicine visits. While this was a small feasibility study, the results uncovered and reinforced the added value of having engaged, highly health-literate patients as a benefit to effective patient-centered communication.
Footnotes
Authors’ Contributions
All authors contributed to the preparation of the manuscript and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Mayo Clinic Office of Research Equity Inclusion and Diversity.
Ethical Approval
Not applicable.
Statement of Animal and Human Rights
All procedures in this study were conducted in accordance with the Mayo Clinic Institutional Review Board (22-101489) approved protocols.
Statement of Informed Consent
Informed consent for patient information to be published in this article was obtained under the Mayo Clinic Institutional Review Board (22-010489) approved protocols.