
Abstract
The Feeling Heard and Understood (FHU) scale evaluates communication between patients and healthcare providers to measure patient-centered care from the patient's perspective. This study aimed to develop a Japanese version of the FHU (FHU-J). Three researchers translated the original scale, and cognitive interviews with 10 hospitalized patients ensured face validity. The survey items were back-translated and approved by the original authors. Two web-based surveys were conducted one week apart to assess the FHU-J's internal consistency, concurrent validity, and test–retest reliability that targeted adults hospitalized for over a week in the past year. The first and second surveys included 608 and 255 respondents, respectively (50.4% men; mean age: 57.0). Surgery was the primary reason for admission (48.1%). The Cronbach α for the FHU-J was .93, and the intraclass correlation coefficient between the 2 responses was 0.54. Cronbach α and correlation coefficients demonstrated sufficient validity of the FHU-J, whereas the intraclass correlation coefficient indicated moderate reliability.
Keywords
Introduction
Patient-centered care adheres to and responds to an individual's preferences, needs, and values, ensuring that patient values guide all clinical decisions. 1 Patient-centered care has become a pervasive principle aimed at addressing communication, basic human needs, and other patient needs. 2 The implementation of patient-centered care is expected to increase patient satisfaction, alleviate symptom severity, reduce healthcare resource utilization, and lower healthcare costs.3,4 Healthcare providers must implement patient-centered communication and achieve a comprehensive understanding of their patients. 5
Many patients report dissatisfaction with the communication they receive from their healthcare providers. 6 Specifically, they describe feeling “silenced, ignored, or misunderstood” in their interactions, note insufficient communication regarding their prognosis or treatment options, or receive care that does not align with their preferences. 6 Such dissatisfaction can result from various factors, including inadequate or excessive information, inappropriate timing of information delivery, inconsistencies among healthcare providers, the use of medical jargon, and insufficient involvement in treatment decisions.7–9 These communication issues may heighten patients’ feelings of anxiety, confusion, and overwhelmingness and can ultimately affect their trust in and overall satisfaction with healthcare providers. Additionally, prior research has demonstrated that patient-centered communication positively influences patient engagement, health-related quality of life, perceived quality of services, and patient satisfaction among patients with cancer.10,11 Therefore, it is essential to evaluate the adequacy of patient–provider communication.
The Feeling Heard and Understood (FHU) Scale was developed in the United States to measure communication between patients and healthcare providers.6,12 This scale is a 4-item questionnaire that focuses on “listening and understanding” and includes components of patient-centered care. 1 Although the original study targeted patients receiving palliative care in an outpatient setting, the scale is applicable to all patients who require care. The majority of palliative care resources are currently used by patients with cancer, 13 but patient-centered care is not intended only for patients with cancer or those receiving palliative care and should begin in the diagnostic and treatment phases. 14 In addition, Japan lacks a scale to measure patient and healthcare provider communication through patient-reported outcomes, which makes it difficult to measure the outcomes of communication interventions that target outpatients.
This study aimed to develop the FHU-J, a Japanese version of the FHU, and to test its reliability and validity in patients with diverse diseases, not limited to those eligible for palliative care.
Methods
The Japanese version was developed according to COnsensus-based Standards for the selection of health Measurement Instruments. 15 Generally, the translation of a scale is performed on the same target as the original scale; however, in a recent study that has been reported, the target was expanded simultaneously with translation, 16 and we have used the same method.
Translation of the Japanese Version of the FHU Scale Items
The FHU was developed in the United States by Edelen et al to evaluate patient–provider communication from the patient's perspective. Permission to use and translate the scale was obtained from all the authors. Three Japanese researchers, including the primary author, translated the original questionnaire into Japanese and reviewed the content. To ensure face validity, cognitive interviews were conducted with 10 adult participants (aged 20-60 years) who were currently receiving outpatient care and had been hospitalized in the past. These participants were selected to align with the target population of the main survey: adults who had been hospitalized for at least one week in the past year. This approach was adopted to ensure that the scale items were understandable and relevant to individuals with recent inpatient experiences. Given our goal of developing a tool applicable across various clinical settings, we considered it important to capture a diverse range of medical experiences during the cognitive testing phase.
A hypothetical scale was used to confirm the respondents’ understanding of the items and concepts, and the wording was modified as needed. Inquiries were made to the original authors were asked about any questions that arose during revision. After these revisions, a translation company (Editage) back-translated the scale. The back-translation was confirmed and approved by the original authors. In the final Japanese version (Appendix 1), brief explanatory notes were added to questions 2 and 3 to improve the clarity for Japanese respondents. These notes were added to avoid potential ambiguity in phrases such as “the things I valued” and “understand me as a person.” Based on the findings of the cognitive interviews, these concepts were found to be somewhat abstract for some participants. Therefore, culturally and linguistically appropriate clarifications were included to support respondents’ understanding. These additions were carefully developed by the research team, approved by the original authors, and did not alter the meaning or intent of the original items.
Survey
Study Design
A cross-sectional survey was conducted using a self-administered Internet-based questionnaire, and its reliability was verified using the retest method.
Participants
The participants were aged 20 years or older, enrolled in an online research company (Cross Marketing, Inc.), and had been hospitalized for one week or more in the previous year. Patients who had been hospitalized for more than one week were selected because those receiving only outpatient care might have less need to feel “heard.” The retest questionnaire was sent to all the participants in the first survey and manually closed when the number of responses exceeded 250.
The sample sizes were determined as follows: Assuming a correlation coefficient of 0.45 between the existing scale and the FHU scale for concurrent validation, a total of 247 participants were required to achieve a 95% confidence interval (CI) of ±0.1. The reference value of 0.45 was based on the results of the original scale development study, 6 in which the FHU scale showed a correlation of approximately 0.45 with the Consumer Assessment of Healthcare Providers and Systems Clinician & Group Survey (CG-CAHPS) communication domain. Therefore, this value was considered as an appropriate estimate for calculating the sample size in the present study. The overall sample size was 600 respondents, which accounted for a 50% retest response rate and the possibility of invalid responses. The cross-marketing registered members consisted of survey-only participants who had enrolled through an open application process, with a total membership of approximately 5.41 million as of January 2022. The research company commissioned more than 300 academic research projects annually. Measures were taken to prevent dishonest responses by removing invalid registrants from the panel and checking for duplicate entries based on personal information.
Research Measurements
Japanese version of the Feeling Heard and Understood
The questions on FHU-J (Appendix 1) were as follows: (1) “I felt that staff, such as doctors and nurses, heard what I had to say and understood my situation.” (2) “I felt that staff, such as doctors and nurses, gave top priority to things I valued when consulting with me about future treatment and care.” (3) “I felt that the staff, such as doctors and nurses, were trying to understand me as a person instead of just looking at my illness.” (4) “I felt that staff, such as doctors and nurses, knew what I valued in my life.” The scale is a 5-point Likert scale ranging from “0: Disagree” to “4: Completely agree,” with higher scores indicating greater trust between the patient and the healthcare provider. The term “staff” was used to refer to all individuals involved in treatment and care, including doctors, nurses, caregivers, physical therapists, and nutritionists.
Consumer Assessment of Healthcare Providers and Systems Clinician & Group Survey
The CG-CAHPS was used to examine the concurrent survey validity. The CG-CAHPS is an instrument developed by the Agency for Healthcare Research and Quality to measure communication among healthcare providers. Its Japanese version has been tested for reliability and validity.17,18 This scale asks patients about their experiences with outpatient care in the past 6 months in 4 domains: consultation, communication with healthcare providers, coordination of care, and administrative staff. In this study, the 4 items in the domain of “communication with healthcare providers” were used with permission from the translator of the Japanese version. The items are measured on a 4-point Likert scale ranging from “never: one point” to “always: 4 points.” In addition, the word “doctor” in the original version was replaced by “staff, such as doctors and nurses” with the permission of the Japanese translator.
Concerns and problem-solving
To examine criterion-related validity, respondents were asked about the 4 aspects of holistic pain (physical pain, psychological pain, social pain, and spiritual pain) using a 5-point scale ranging from “not at all agree: 0” to “completely agree: 4.” The respondents were asked whether they “wanted to talk,” “were able to talk,” and “solved the problem” with their healthcare provider. Differences in the FHU-J scores were compared based on whether the problems were resolved.
Participant characteristics
The participant background information evaluated in this study included sex, age, marital status, presence of children, purpose of hospitalization, severity of illness and treatment, duration of doctor visits before hospitalization, number of hospitalizations in the same ward, duration after discharge, employment status, household income, educational background, and healthcare providers perceived as deeply interacting during hospitalization. Participants were asked multiple-choice questions regarding the healthcare providers who interacted deeply with them during hospitalization.
Survey Procedure
Internet surveys were conducted in December 2022, and retests were conducted one week after the initial survey. Given that individuals who experienced hospitalization were likely to be older adults, the survey company was instructed to ensure an even age distribution at the time of sampling to test the reliability and validity of the results across diverse participants.
Statistical Analysis
All of the participants were included in the analysis. The FHU-J was tested for ceiling and floor effects by calculating the distribution, mean, and standard deviation of each item. The Cronbach α coefficient was calculated to assess internal consistency. To examine concurrent validity, Pearson's correlation coefficient was calculated between the total score of the FHU-J scale and that of the CG-CAHPS. Intraclass correlation coefficients (ICCs) were calculated using the retest method to verify reliability, and we used ICC (A, 1). 19
Statistical analyses were performed using JMP Pro, version 16 (SAS Institute). Two-tailed P values of P < .05 were considered statistically significant.
Ethical Considerations
Individual privacy was ensured because personally identifiable information was managed by the survey company and not obtained by the researchers. Cross-Marketing Inc. is a privacy-mark-certified company that guarantees that the personal information of survey participants will not be provided to third parties without their consent. This study was approved by the Ethics Review Committee [details omitted from the double-anonymized peer review].
Results
Six hundred and eight participants responded to the initial survey, and 255 participants responded to the retest.
Participant Backgrounds and Situations During Hospitalization
Table 1 shows the study participants’ backgrounds and situations during hospitalization. The participants included 306 men (50%) and 302 women (50%), with a mean age ± standard deviation of 57.0 ± 16.8 years. The diseases that required hospitalization included musculoskeletal and connective tissue diseases (70 patients, 12%), gastrointestinal diseases (68 patients, 11%), and cardiovascular diseases (60 patients, 10%). Healthcare providers who were perceived as deeply interacting during hospitalization included nurses (515 participants, 85%), physicians (497 participants, 82%), and physical therapists (166 participants, 27%). The average number of healthcare providers who interacted deeply with participants was 2.2.
Participants Background.

Percentages are rounded off; therefore, some items do not total 100%.
Internal Consistency and Retest Reliability
Table 2 shows descriptive statistics, including the distribution, mean, standard deviation, and retest reliability of each item on the FHU-J scale. The mean ± standard deviation of the total score was 7.9 ± 4.0, and Cronbach α was 0.93 (95%CI: 0.92-0.94). The overall ICC was 0.54, and the item-specific ICCs ranged from 0.45 to 0.50.
Feeling Heard and Understood Japanese Response Results.
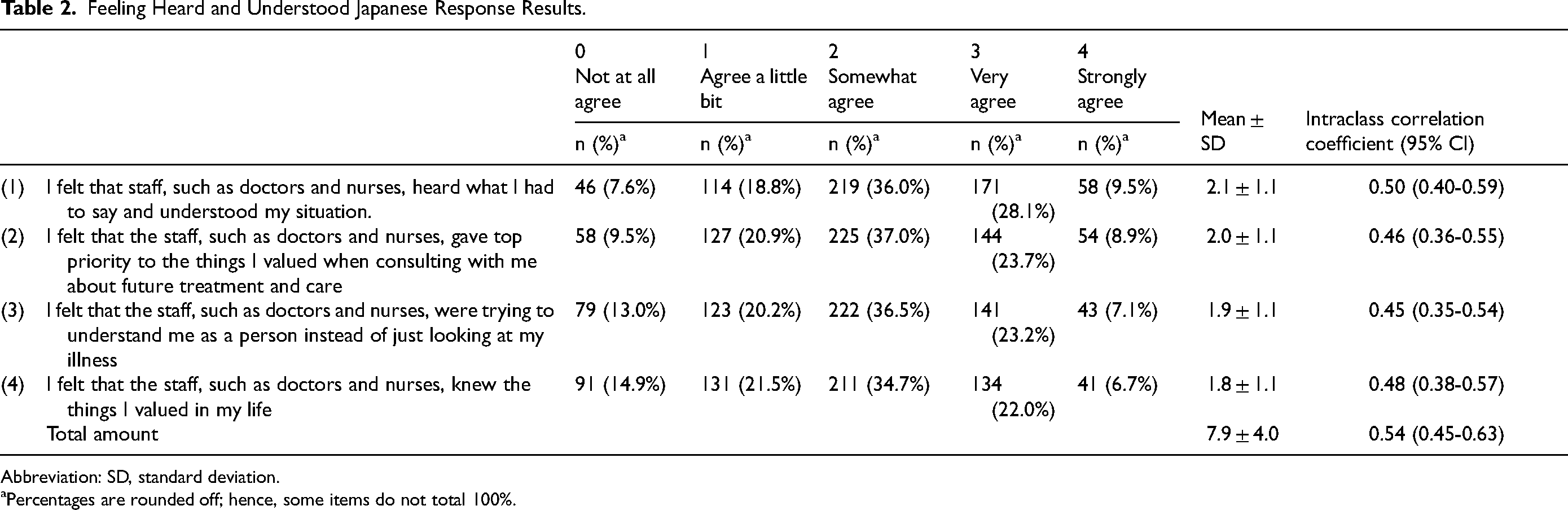
Abbreviation: SD, standard deviation.
Percentages are rounded off; hence, some items do not total 100%.
Mean Comparison of the FHU-J Total Scores by Background Factors
Table 3 shows items with statistically significant differences in the mean comparisons of FHU-J total scores based on background factors.
Comparison of the Total Feeling Heard and Understood (FHU) Japanese Scores by Background Factor.

Men had significantly higher mean total scores than women (effect size [ES] = 0.02, P = .01), and age significantly and positively correlated with total score (correlation coefficient (r) = 0.10, P = .01). Married participants had significantly higher total scores than unmarried participants (ES = 0.22, P = .04). By purpose of hospitalization, the total score was lower for patients with musculoskeletal and connective tissue disorders (ES = −0.18), psychological and behavioral disorders (ES = −0.36), and neurological disorders (ES = −0.50) compared with the scores for patients with cancer. The total score was also slightly higher for cardiovascular disorders (ES = 0.10, P = .006) than for cancer. Among healthcare providers who were perceived as deeply interacting during hospitalization, the total score was higher when participants perceived deep interactions with a doctor (ES = 0.43, P < .0001), caregiver (ES = 0.42, P = .004), or dietitian (ES = 0.27, P = .013).
Concurrent Validity
Pearson's correlation coefficient between the FHU-J scale total score and the total score of the “Communication with Healthcare Providers” domain of the CG-CAHPS was calculated to examine concurrent validity. The correlation coefficient was 0.67 (95%CI: 0.62-0.71, P < .0001).
Criterion Validity
Appendix 2 shows the distribution of responses to whether participants “wanted to talk to the healthcare providers,” “were able to talk to the healthcare providers,” or “solved the problem” regarding the following aspects: (1) physical pain, (2) psychological pain, (3) life after discharge, and (4) purpose in life and sense of values.
Table 4 shows the distribution of the total scores on the FHU-J scale for participants who indicated whether their problems were resolved, among those who desired to talk to healthcare providers. For each item, the FHU-J scale total score was statistically significantly higher for the group that answered “agree” or “completely agree” to the “problem was solved” item than for the group that answered “disagree” or “completely disagree.”
Distribution of Problem-Solving and Feeling Heard and Understood (FHU) Total Scores Among Those Who Wanted to Talk.

Fisher exact test.
Excludes those who answered undecided” to “the problem has been solved.”
Discussion
This study translated and tested the reliability and validity of the FHU-J. The main findings of this study are as follows. First, the scale presented excellent internal consistency, with a Cronbach α of 0.93. 20 Second, the test–retest reliability was moderate (ICC = 0.54), based on commonly accepted criteria. 21 Third, the FHU-J showed good concurrent validity, with a correlation coefficient of 0.67 between the FHU-J and CG-CAHPS communication domains. These results suggest that the FHU-J is a reliable and valid tool for assessing patient–provider communication from a patient's perspective.
The FHU-J scale also attained sufficient internal consistency and a moderate correlation with the “communication with the healthcare provider domain of the CG-CAHPS.” The correlation coefficient with the English CG-CAHPS in the original version of the FHU was 0.45, 6 showing a similar trend.
The test–retest reliability of the FHU-J scale (ICC = 0.54) was moderate and lower than that of the original version (ICC = 0.72), 6 and several factors can explain this discrepancy. First, participants in the current study were asked to recall their communication experiences during a hospitalization that occurred within the previous year, which may have introduced a recall bias and reduced the stability of their responses over time. By contrast, the original study administered the scale to patients who were actively receiving outpatient palliative care, a population for whom communication is an immediate and ongoing need. This may have potentially resulted in more consistent perceptions.6,12
Second, the present study targeted a broader and more heterogeneous population that included patients with varying diagnoses, severities, and reasons for hospitalization. These contextual differences may have led to a wider range of communication experiences and expectations, thereby affecting the consistency of the responses between the 2 time points.
Third, participants in this study were asked to rate their experiences with “staff such as doctors and nurses” as a general group, rather than responding in relation to a specific provider. This lack of specificity may have led participants to reflect on different individuals or professional roles across the 2 survey administrations, thus contributing to response variations. Defining the target provider, such as an attending physician or primary nurse, may help enhance the reliability of future research studies.
Finally, although the observed ICC was moderate, it was achieved despite the retrospective nature of the study and the diversity of the target population. This suggests that the FHU-J is sufficiently robust for general use, and its reliability may improve further when applied in real time or in patient populations with more consistent and ongoing communication needs, such as those receiving continuous or palliative care.
When comparing the mean total FHU-J scale score with the background factors, most variables did not have a statistically significant association, and for those that did, the ES was small. This limited association between background factors and FHU-J scores aligns with the findings of previous studies, including the original development studies,6,12 in which demographic background factors were not extensively analyzed because of the homogeneity of their study populations (palliative care patients). Westendorp et al reported that patient satisfaction and dissatisfaction with healthcare provider communication primarily depend on the quality and content of the interactions, rather than on demographic characteristics such as age, sex, or disease type. 9 Therefore, the FHU-J scale is considered suitable for assessing patient–provider communication without being substantially influenced by the patient demographic backgrounds.
Significant differences in the FHU scores were observed that depended on whether the patient interacted deeply with the physician, which suggests that the relationship between a patient and physician was strongly related to trust in healthcare providers. The physician–patient relationship, which is central to interpersonal interactions in quality healthcare, is particularly important for patient trust.22,23 Patients have a fundamental psychological need to feel acknowledged, respected, understood, seen, and heard by their healthcare providers. In particular, continuity of care, in which patients see the same physician consistently and receive full clinical and personal attention, is an essential factor.24,25 Furthermore, patients who feel more engaged with their physicians are more likely to develop a stronger sense of trust.
Conversely, there was no statistically significant difference in the total FHU-J scale score based on whether a patient interacted deeply with nurses or the rehabilitation staff. However, the absence of statistical significance does not necessarily indicate a lack of impact. Rather, this indicates that the null hypothesis cannot be rejected based on the current sample size and data. Certain job types may influence patient perceptions of communication; however, such effects may not have been detected because of insufficient statistical power or sample composition. Future studies with larger and more focused populations are required to examine these potential differences more precisely.
Second, the criterion-related validity in this study indicated that being able to talk led to the resolution of a patient's problem, which suggests that the ability to talk may have contributed to problem resolution. Conversely, it is also possible that the resolution of the problem influenced the subjective response of “being able to talk.”
The application of the FHU-J scale in Japan may be influenced by cultural and healthcare system factors that are unique to the Japanese context. For example, Japanese cultural norms often emphasize harmony and respect for authority, which can make patients less likely to express their concerns directly or challenge medical decisions. 26 This contrasts with Western contexts, in which patient autonomy and direct communication are encouraged more commonly. Consequently, Japanese patients might interpret the concept of “feeling heard and understood” differently, thus potentially affecting their responses on the FHU-J scale. 27
Additionally, the Japanese healthcare system is characterized by brief consultations and a high patient volume, which limits opportunities for in-depth patient–provider communication. 28 This systemic aspect may influence patient perceptions of being heard and understood, as measured by the FHU-J. Furthermore, the role of families in medical decision-making is more pronounced in Japan. Patients often prefer to involve family members in discussions and decisions regarding their care, which can affect their perceptions of communication with healthcare providers. 26 This familial involvement may not be fully captured by the FHU-J, which focuses on direct patient–provider interactions. These cultural and systemic factors should be considered when interpreting FHU-J scores and highlight the importance of contextualizing patient-centered communication assessments within specific cultural and healthcare settings.
In summary, the FHU-J scale is useful for assessing patient–medical staff communication. In the future, this scale can be applied regardless of disease or severity to identify patient-centered communication problems and evaluate medical staff ability to engage in patient-centered communication.
Limitations
This study had several limitations that should be kept in mind when interpreting our findings. First, because data were collected through an Internet-based survey, participants were limited to registered monitors of a research panel, which may have introduced a selection bias. Nonetheless, the sample included individuals from diverse age groups, educational backgrounds, and income levels, which suggest some degree of generalizability despite its online format.
Second, participants were asked to reflect on their communication experiences during hospitalization that occurred within the past year. This retrospective design may have introduced a recall bias, particularly for those whose hospitalizations occurred several months prior to the study. Furthermore, as the study did not restrict the type or severity of illness, some participants may have experienced relatively mild conditions and faced fewer communication-related challenges. These factors may have contributed to the observed moderate test–retest reliability.
Third, this study exclusively focused on inpatient experiences. It should be noted that communication in outpatient settings may differ significantly in both frequency and context from inpatient settings. Therefore, the generalizability of the findings to outpatient care or patients who were hospitalized for fewer than 7 days may be limited.
Finally, participants were asked to evaluate communication with “staff such as doctors and nurses,” which referred to all healthcare providers involved in their care. Since each participant may have interpreted this differently—some thinking of physicians, nurses, or therapists—variability in the respondents’ assumptions may have affected the consistency of the responses. This variation should be considered when interpreting our findings.
Conclusion
This study aimed to develop a Japanese version of the FHU (FHU-J) scale and to evaluate its reliability and validity among adults with recent hospitalization experiences. The results showed that the FHU-J had excellent internal consistency and moderate test–retest reliability. It also demonstrated good concurrent and criterion validity through correlations with the CG-CAHPS communication domain and associations with problem resolution in communication with healthcare providers.
These findings suggest that the FHU-J is a psychometrically sound tool that can be used to assess the quality of patient–provider communication from a patient's perspective. This scale may be applicable across a wide range of medical settings and is not limited to palliative care. Practically, the FHU-J can be used in quality improvement initiatives, patient experience surveys, and communication training for healthcare professionals.
Future research should explore the applicability of FHU-J to specific patient populations, including those receiving palliative care, and assess its impact on clinical outcomes and care quality.
Footnotes
Acknowledgments
This work was supported by Grants-in-Aid for Scientific Research(B) Grant Number 21H03230. The authors would like to express our sincere gratitude to Dr Edelen of the Behavioral & Policy Sciences Department, RAND Corporation, Boston, Massachusetts, USA, who developed the FHU scale, the members of the Department of Palliative Nursing, Tohoku University, for their valuable guidance and encouragement in carrying out this research and patients for their cooperation.
Authors’ Note
Any other identifying information related to the authors and/or their institutions, funders, approval committees, etc, that might compromise anonymity.
Author Contributions
All authors contributed to the conception and design of the study as well as to the critical revision of the manuscript. Miki Takahashi and Hideyuki Hirayama collected the data, conducted statistical analyses, and drafted the manuscript. All authors have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
This study was approved by the Ethics Review Committee of the Tohoku University Graduate School of Medicine (Reception No. 2022-1-153). Individual privacy was ensured by managing personally identifiable information through the survey company, which was not accessed by the researchers. Cross Marketing, Inc. is a privacy-mark-certified company that guarantees that the personal information of survey participants will not be disclosed to third parties without their consent.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Japan Society for the Promotion of Science through a Grant-in-Aid for Scientific Research (Issue No.: 21H03230).
Appendix 1. Feeling Heard and Understood Japanese Version
Feeling Heard and Understood Japanese Version
このアンケートは、患者様が「医療スタッフに話を聞いてもらえた、理解してもらえた」と感じているかをお尋ねするためのアンケートです。
それぞれもっとも当てはまるもの1つにチェックをおつけください。(それぞれ1つずつ)
⋇「スタッフ」とは、あなたの治療やケアに関わる医師や看護師、介護士、理学療法士、栄養士などを含む全ての人を指します。
そう 思わない
少し
いくらか
とても
まったく
1. 医師や看護師などのスタッフは、私の話をよく聞いてくれ、私の状況を理解してくれていると感じた。
0
1
2
3
4
2. 医師や看護師などのスタッフは、私に今後の治療やケアをどうするか相談する時、私の大切にしていることを最も優先してくれていると感じた。
0
1
2
3
4
3. 医師や看護師などのスタッフは、私の病気だけを見るのではなく、人として理解しようとしてくれていると感じた。
0
1
2
3
4
4. 医師や看護師などのスタッフは、私が毎日の生活の中で大切にしていることは何か分かってくれていると感じた。
0
1
2
3
4
Appendix 2. Resolution of the Problems You Had During Your Hospitalization

| 0 | 1 | 2 | 3 | 4 | ||
|---|---|---|---|---|---|---|
| Not at all. |
I do not think so. | Cannot say | I think so. | I do not think so. |
||
| n (%) | n (%) | n (%) | n (%) | n (%) | ||
| 1) Physical pain About |
I needed to talk to a medical professional. | 25 (4.1%) | 124 (20.4%) | 164 (27.0%) | 241 (39.6%) | 54 (8.9%) |
| I could talk to a medical professional. | 26 (4.3%) | 57 (9.4%) | 147 (24.2%) | 310 (51.0%) | 68 (11.2%) | |
| Problem solved. | 27 (4.4%) | 66 (10.9%) | 206 (33.9%) | 252 (41.4%) | 57 (9.4%) | |
| (2) Pain of Feeling About |
I needed to talk to a medical professional. | 41 (6.7%) | 147 (24.2%) | 182 (30.0%) | 173 (28.5%) | 65 (10.7%) |
| I could talk to a medical professional. | 44 (7.2%) | 93 (15.3%) | 203 (33.4%) | 215 (35.4%) | 53 (8.7%) | |
| Problem solved. | 37 (6.1%) | 84 (13.8%) | 234 (38.5%) | 200 (32.9%) | 53 (8.7%) | |
| 3) Life after discharge About |
I needed to talk to a medical professional. | 84 (13.8%) | 134 (22.0%) | 178 (29.3%) | 164 (27.0%) | 48 (7.9%) |
| I could talk to a medical professional. | 76 (12.5%) | 104 (17.1%) | 206 (33.9%) | 172 (28.3%) | 50 (8.2%) | |
| Problem solved. | 61 (10.0%) | 83 (13.7%) | 235 (38.7%) | 169 (27.8%) | 60 (9.9%) | |
| 4) Purpose in life and values About |
I needed to talk to a medical professional. | 114 (18.8%) | 160 (26.3%) | 199 (32.7%) | 95 (15.6%) | 40 (6.6%) |
| I could talk to a medical professional. | 99 (16.3%) | 152 (25.0%) | 220 (36.2%) | 100 (16.4%) | 37 (6.1%) | |
| Problem solved. | 85 (14.0%) | 113 (18.6%) | 249 (41.0%) | 106 (17.4%) | 55 (9.0%) |