
Abstract
Access to specialist Parkinson's disease (PD) services is limited in rural Australia. This study aimed to describe patient experiences of a novel health care model for PD introduced into a rural Australian health center. The program provided specialist PD services, which included a Parkinson's specialist nurse based at the center and a metropolitan-based Parkinson's specialist neurologist who used telehealth to consult remotely with the program's patients. Patient experiences of the program were captured using the Patient-Centered Questionnaire for PD. Scores included the overall patient-centered score (OPS, range 0-3), subscale experience scores (SES, range 0-3), and quality improvement scores (QIS, range 0-9). The mean (SD) OPS for 52 participants was 1.9 (0.5), a moderate patient-centeredness experience. Most subscale experiences were rated highly, including empathy and Parkinson's expertise (mean 2.4, SD 0.6) and accessibility of health care (mean 2.3, SD 0.8). Experience of provision of tailored information was poorly rated (mean 1.3, SD 0.6). Overall, patient needs were met by this program. Trialing the program at other rural health centers is now required.
Keywords
Key Points
Access to specialist Parkinson's disease (PD) services is limited in rural Australia.
A novel PD program was established in an Australian rural health service.
PD-specific services included a PD specialist nurse and telehealth consultations with a metropolitan-based neurologist.
A survey of attendees’ experiences of this PD program found that overall they had positive healthcare experiences and their needs were met.
Introduction
Parkinson's disease (PD) is a chronic, incurable, neurodegenerative condition that is characterized by complexity in its symptomatology, cumulative morbidities over the lifetime of the individual and by additional age-related co-morbidities because of the high prevalence in the elderly age group. There is much debate about the service delivery models most appropriate to manage the condition.1,2 Integrated multidisciplinary care, led by a PD specialist neurologist, has general agreement within the PD global communities for managing the varied impact motor and nonmotor symptoms have on the individual's function and quality of life.1–3
Specialist PD teams with healthcare professionals from a range of disciplines are not widely available in Australia.4–6 Several key PD centers exist in Australian capital cities, but these are primarily based on a medical model and at most provide nursing support with limited specialist clinical expertise in allied health disciplines. In rural and regional communities, even this level of urban medical expertise is rarely available.4–6 People with PD living in rural Australian communities face multiple challenges when needing to access health care, such as large travel distances and travel costs, and the limited availability of health service providers. The small number of people with PD living in any rural community and the large distances between rural communities and health services can challenge the sustainability of PD specialist services. 7 People with PD in rural settings are, therefore, at risk of receiving inadequate care, especially as their health needs and preferences change over time. These barriers to PD specialist services in rural Australian communities can result in poor health outcomes and a poor quality of life. 8
New models of health care are needed to address the barriers that limit access to specialist PD services in rural Australia. Most attempts at improving rural care for people with PD in Australia have focused on a nursing model in which a specialist trained nurse is located at a rural site and oversees and assists the local PD community. 9 The Parkinson's nurse specialist does, however, need to work in conjunction with a PD specialist neurologist to ensure quality health care is provided, there is continuity of care, the patient's changing needs are managed expertly and ongoing education and support is available for the nurse.
The use of telehealth has accelerated in Australia in recent times with greater government funding, especially during the COVID-19 pandemic. 10 Telehealth is suited to chronic diseases, such as PD, where a re-assessment face to face is not needed at every consultation. With PD, many of the symptoms can be assessed visually along with input from the patient and carer. Telehealth has been shown to deliver effective care to people with PD and to be acceptable to both patients and health professionals.11,12 Telehealth overcomes many of the barriers to receiving good health care in rural and remote communities, such as travel distances and time. 13
When an Australian rural community health center's PD program was forced to discontinue due to the COVID-19 pandemic travel restrictions placed on the visiting metropolitan-based PD neurologist, the decision was made to re-model it. The new PD program provided face-to-face sessions with a PD nurse and telehealth consultations with the metropolitan-based neurologist.
This study aimed to describe the healthcare experiences of people with Parkinson's who attended this novel Parkinson's program introduced at an Australian rural health service.
Overview of a Novel PD Program in Rural Australia
Prior to the pandemic, a metropolitan-based neurologist, supported by a locally based Parkinson's specialist nurse, had provided regular in-person consultations and treatments at a rural community health center. The COVID-19 pandemic forced the program to change. The re-modeled program had the same PD nurse coordinate services and provide in-person consultations with clients of the health service. The nurse had expertise in medication adjustments, test dose assessments, initiation and administration of liquid Sinemet, experience in deep brain stimulation (DBS) programing as well as Duodopa education, problem solving and maintenance. Telehealth consultations were provided weekly at 2 rural medical locations with 6 monthly in-person visits by the same neurologist. The Parkinson's nurse coordinated the telehealth consultations with the client present and assisted with examinations, explained treatment plans, and provided information and ongoing support to patients and carers. A shared electronic medical record enabled communication between the specialist, the nurse, the general practitioner, and relevant allied health staff involved in each client's care. The nurse also provided in-person visits to clients as required. The core features of the rural Parkinson's program are summarized in Table 1.
Description of the Rural Model of Parkinson's Care.

Methods
Participants
Participants were eligible for the study if they had a diagnosis of idiopathic PD or Parkinsonism, had attended the new rural-based PD program within 12 months from the commencement of the study, and, where English was not their first language, had sufficient proficiency to understand the questions and respond.
Participants were deemed to have provided informed consent if they returned the completed questionnaire and marked the consent box in the Agreement to Participate section of the questionnaire. The relevant Human Research Ethics Committee (HREC) assessed this project as being exempt from HREC review and approved it as a Quality Assurance and Evaluation Activity.
Recruitment Process
Purposive sampling was used to recruit participants. All active clients of the new rural Parkinson's program were contacted by the neurologist by telephone, who explained the purpose of the evaluation and the process involved. All clients who were eligible and who agreed to participate were then sent a copy of the questionnaire by administrative staff. No participant identification data was entered into the questionnaire. Participants returned the completed deidentified questionnaire in a provided stamped, self-addressed envelope.
Outcomes
The questionnaire was designed to be self-administered. Participants were informed that the questions were to be answered by themselves, but they could ask a caregiver or family member for assistance if needed.
Standard demographic information was collected, as well as self-ratings of physical health and mental health. A number of PD-specific validated measures were also used to describe the population in regard to the Parkinson's condition. These included the self-rated impairment measure the Hoehn and Yahr staging tool, 14 the Parkinson's health related quality of life questionnaire (PDQ-39) 15 and the MDS-Unified PD rating scale (MDS-UPDRS) Part II to measure the impact of Parkinson's on motor activities of daily living. 16
The prime evaluation tool was the Patient-Centered Questionnaire for PD (PCQ-PD), which was initially developed in the Netherlands and validated with a Dutch-speaking population. 17 The questionnaire was translated into English by the developers and later validated with an English-speaking Northern American population. 18 Key constructs of patient-centeredness as defined by the Picker Institute 19 and the World Health Organization (WHO) 20 formed the basis for the PCQ-PD questions. The PCQ-PD includes questions regarding the needs associated with in-patient and out-patient care as well as the disciplines typically providing care. 17 Outcome scores for the PCQ-PD included the overall patient-centeredness score (OPS, range 0-3), the 6 subscale experience scores (SES, range 0-3) and the quality improvement scores (QIS, range 0-9). 17 A range of healthcare experiences rated by the participants were used to determine the OPS and SES. The lower the scores for the OPS and SES, the poorer the experience. Participants were asked to rate the importance of 44 aspects of health care. The rating score was used to calculate the quality improvement score for each of the 44 items. 17 A score of 0 was a low improvement priority, and a score of 9 was a high improvement priority.
Participants’ experiences of telehealth and of the program were also included in the questionnaire. The telehealth experience questionnaire 21 utilized 15 questions, each offering one out of a possible 5-point Likert-based scale for response, ranging from strongly agree to strongly disagree.
A service quality questionnaire was also included to examine the clients’ experiences of the program relating to the structure of the clinic and how it ran on a day-to-day basis. The questionnaire was based on the Gronroos 22 quality service model and included 10 questions, each offering one out of a possible 5-point Likert-based scale for response, ranging from strongly agree to strongly disagree. 22
Analysis
Demographic data, scores from the PD measures, and healthcare experiences were described using descriptive statistics.
Results
Demographic and Clinical Characteristics
Seventy-nine clients of the new rural Parkinson's program were contacted by phone to determine their interest in participating in the study, of whom 71 agreed to the questionnaire being mailed to them. Questionnaires were returned by 54 clients (response rate 76%), of whom 2 were excluded. One client was excluded because they were unable to complete the questionnaire, and the other because they had not attended the service in the last 12 months. The demographics and clinical characteristics of the 52 participants are reported in Table 2. These older (age mean 76.7, SD 8.2 years), mainly male (34, 67%) participants had mild to moderate bilateral disease (HY mean 2.6, SD 1.2). The majority of participants (45, 88%) rated their healthcare experience as good to excellent. Physical health was rated good to excellent by 30 (59%) and mental health was rated good to excellent by 35 (69%). The MDS-UPDRS part II mean score indicated moderate disability. 23 The quality of life was decreased below what would be expected for the disease duration.
Demographic and Clinical Characteristics.

Abbreviations: TAFE, technical and further education; HY, Hoehn and Yahr; MDS-UPDRS, Movement Disorders Society Unified Parkinson's Disease Rating Scale; PDQ-39, Parkinson's Disease Questionnaire-39.
All data reported as mean (SD) unless stated otherwise. Valid percentage reported if data is missing.
a Data missing.
Overall OPS and SES
Scores for the OPS and 6 SES are reported in Table 3. The mean OPS was 1.9 (SD 0.5), which indicated patient-centeredness experience was moderate for this group. The experiences most highly rated were empathy and PD expertise (mean 2.4, SD 0.6), accessibility of health care (mean 2.3, SD 0.8) and continuity and collaboration (mean 2.2, SD 0.7). The experience of provision of tailored information was poorly rated (mean 1.3, SD 0.6) and involvement in decision making and emotional support were given an average rating (mean 1.60, SD 0.7 and 1.8, SD 1.0, respectively).
Overall Patient-Centeredness Scores (OPS) and Subscale Experience Scores (SES) for All 6 Subscales.

Abbreviations: OPS, overall patient-centeredness scores; SES, subscale experience scores.
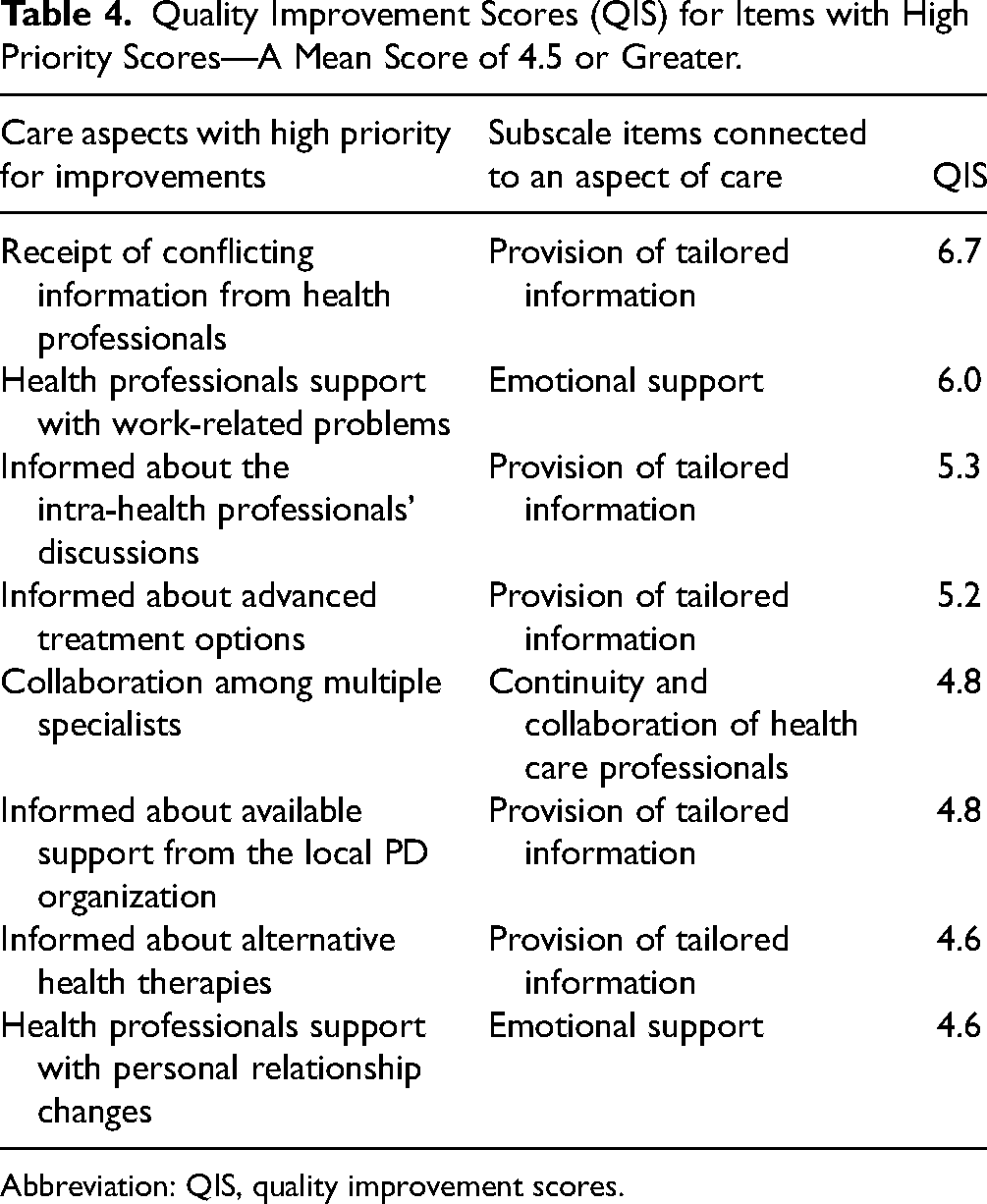
Priority items for improvement with a score > 4 were 8 in total. These items are detailed in Table 4. The improvement items related to the provision of tailored health information, better communication, and increased emotional support in specific areas of work and relationships.
Quality Improvement Scores (QIS) for Items with High Priority Scores—A Mean Score of 4.5 or Greater.
Abbreviation: QIS, quality improvement scores.
Telehealth Experiences
The clients’ telehealth experiences were overall positive in all areas covered by the questionnaire (Supplemental Figure 1). The following number (%) of participants expressed their satisfaction (rated as strongly agree or agree) with each of the 15 questions: (1) ease of talking with their healthcare provider 38 (75%); (2) ease of hearing their healthcare provider 43 (86%); (3) healthcare provider understanding their condition 43 (90%); (4) see healthcare provider as good as in person 42 (82%); (5) no assistance needed using the system 32 (68%); (6) feel comfortable communicating 43 (86%); (7) healthcare provided was consistent 44 (88%); (8) better access to services 33(67%); (9) saves travel time 46 (92%); (10) receive adequate attention 42 (84%); (11) healthcare needs are met 36 (75%); (12) meet more frequently 30 (60%); (13) telemedicine is acceptable 38 (76%); (14) will use services again 39 (80%); and (15) satisfied with quality of service 37 (76%).
Similarly, the quality of the service provided by the clinic was highly acceptable without exceptions (Supplemental Figure 2).
Discussion
The rural-based Parkinson's program presented in this report is indeed unique as it combines the expertise of a metropolitan-based PD specialist neurologist with that of a PD specialist nurse based at a rural health center. This hybrid approach overcomes the difficulties of providing a PD program in a rural community. The healthcare experiences of the participants showed patient-centeredness to be moderate, similar to findings from prior studies that also used the PCQ-PD.17,18,24 A prior study that reported on the healthcare experiences of Australians with PD also found that experiences of accessibility of health care and empathy and PD expertise were rated highly overall. 24 Poor experience sub scores were evident in both this current and the prior Australian study for provision of tailored information and the involvement in decision making. 24
This current study showed the overall patient-centeredness scores to be moderate (mean 1.94, SD 0.5), similar to findings from prior studies that used the PCQ-PD.17,18,24 The patient-centeredness score of a Dutch PD sample was moderate (mean 1.69, SD 0.45) 17 as was that of a North American sample (mean 2.09, SD 0.44) 18 and an Australian sample (mean 1.8, SD 0.5). 24 This current study did not compare patient experiences of the prior model with those of this new hybrid model. This needs further exploration, as does the investigation of confounding factors impacting on the participants’ experiences of this new model.
The quality of health care received is dependent on several factors, including access to accurate and relevant information. Participants in this current study reported having a poor experience of receiving tailored information, and they prioritized its improvement. Similar findings were reported by prior studies that used the same questionnaire.17,18,24 Participants in this current study prioritized the improvement of several aspects of care related to tailored information, such as improved consistency of the information provided by health professionals and being better informed about what health professionals discussed together about their care. They also wanted to be better informed about advanced treatment options and alternative health therapies. These findings can help health services to better target the information needs of patients.
The experience of involvement in shared decision making was also rated poorly in this current study, similar to prior findings. 24 People with PD want to be involved in the clinical decision making, however, often fail to do so because of various barriers. 25 As shared decision making is important to patients with PD, healthcare services need to be aware of the barriers to participation in it. Interestingly, healthcare aspects connected to involvement in clinical decision making were not given a high priority for improvement, the reasons for which were not explored. Further research is warranted to explore why patients may not prioritize its improvement.
This current study did not explore why participants rated poorly or highly their experiences of the various aspects of their care. Future qualitative research using interviews or focus groups would provide an in-depth understanding of their experiences which would assist health services to better target the needs of patients thereby deliver quality patient-centered care.
Australian models of PD health care adopted in regional and rural centers for people living with PD have mostly involved nurse-led specialist care, however reporting on their outcomes is limited. A report on a program led by a specialist PD nurse in a rural Australian community found that participants had positive healthcare experiences. 26 There was an outreach neurologist clinic held for 6 months in this community; however, the interplay between the clinic and PD nurse was not reported, limiting the comparison with this current study. A 2-site case study reported on PD services provided by two PD specialist nurses working at separate Australian regional centers in Australia. 27 One nurse worked as a sole practitioner with limited resources and limited access to other health professionals; however, this care model was viewed as unsustainable. The other PD nurse also worked as a sole practitioner but within the local health district alongside a multidisciplinary clinical team with access to health service processes that enabled effective management of patient loads. This model of care was seen as preferable. The nurse's scope of practice and access to service processes were similar to those of the PD nurse in this current study. Cost benefits have also been demonstrated for PD nurse services provided in regional Australia. 5 This current study did not investigate the cost-benefits of the new program, limiting comparisons between studies. Future research is needed to conduct a cost-benefit analysis of this novel PD care model.
Participants in this current study appeared satisfied with the telehealth arrangement, with strong agreement with 10 out of the 15 questions and the remaining 5 questions with just agreement. Similarly, the quality of service was also given a strong agreement across the 10 questions.
Limitations
This study does provide a model of care introduced into a rural health service that was acceptable to the majority of people who were registered with the program. However, generalizing the findings to the broader PD rural Australian population is limited due to the small sample size. Additional research involving a larger sample size is needed to confirm and extend the generalizability of the findings before introducing this model more broadly.
There was potential for selection bias and for participants to feel coerced into consenting to the study because the program's neurologist, one of the study's authors, recruited them. To minimize selection bias, all clients of the program were invited to participate. To avoid unintentional coercion, the neurologist did not distribute questionnaires, nor know who participated. Administrative staff not known to participants mailed the deidentifed questionnaire to eligible recruits, and all completed questionnaires were returned to them. The questionnaire also included a plain language statement for participants that explained that participation was voluntary and that their responses could not be linked to them.
Practical Implications
The establishment of similar hybrid approaches would necessitate the collaboration of a major metropolitan center, with Parkinson's specialists, with a rural community health center with capacity to provide multidisciplinary services. Besides the specific requirements of the model the key elements would be consistency of the care team, regular telehealth clinics, bi-annual face-to-face visits by the Parkinson's specialist and that the PD specialist nurse be adequately trained in medical and surgical aspects of Parkinson's care as well as rehabilitative approaches to enable appropriate referrals.
Conclusion
Findings from this current study provide support for a model of care that can provide PD specialist services across regional and rural health services in Australia, where resources are limited. While further research is required, we believe that such a model of care can be readily reproduced based on the hub-and-spoke arrangement presented.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251346590 - Supplemental material for A Rural Health Model for Parkinson's Care: The Clients’ Perspective
Supplemental material, sj-docx-1-jpx-10.1177_23743735251346590 for A Rural Health Model for Parkinson's Care: The Clients’ Perspective by Robert Iansek, Mary Danoudis and Melissa Ceely in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735251346590 - Supplemental material for A Rural Health Model for Parkinson's Care: The Clients’ Perspective
Supplemental material, sj-docx-2-jpx-10.1177_23743735251346590 for A Rural Health Model for Parkinson's Care: The Clients’ Perspective by Robert Iansek, Mary Danoudis and Melissa Ceely in Journal of Patient Experience
Footnotes
Acknowledgments
We are grateful to all participants who gave their time and support to this study. We thank the administrative staff who assisted in the distribution of the questionnaires.
Authors Contributions
RI was responsible for the conception and design of the study, analysis and interpretation of the data, and drafting of the article. MD was responsible for the acquisition, analysis, and interpretation of the data and drafting of the article. MC was responsible for the acquisition of the data and assistance with drafting of the article.
Data Availability
Data supporting this study are available from the corresponding author upon reasonable request.
Declaration of Conflicts of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The relevant Human Research Ethics Committee (HREC) assessed this project as being exempt from HREC review and approved it as a Quality Assurance and Evaluation Activity.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent to Participate
All participants provided consent. Participants were deemed to have provided informed consent if they returned the completed questionnaire and marked the consent box in the Agreement to Participate section of the questionnaire.
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.