
Abstract
Community-based healthcare delivery systems frequently lack cancer-specific survivorship support services. This leads to a burden of unmet needs that is magnified in rural areas. Using sequential mixed methods we assessed unmet needs among rural cancer survivors diagnosed between 2015 and 2021. The Supportive Care Needs Survey (SCNS) assessed 5 domains; Physical and Daily Living, Psychological, Support and Supportive Services, Sexual, and Health Information. Needs were analyzed across domains by cancer type. Survey respondents were recruited for qualitative interviews to identify care gaps. Three hundred and sixty two surveys were analyzed. Participants were 85% White (n = 349) 65% (n = 234) female and averaged 2.03 years beyond cancer diagnosis. Nearly half (49.5%) of respondents reported unmet needs, predominantly in physical, psychological, and health information domains. Needs differed by stage of disease. Eleven interviews identified care gap themes regarding; Finding Support and Supportive Services and Health Information regarding Care Delivery and Continuity of Care. Patients experience persistent unmet needs after a cancer diagnosis across multiple functional domains. Access to community-based support services and health information is lacking. Community based resources are needed to improve access to care for long-term cancer survivors.
Introduction
There are currently 17 million cancer survivors in the United States (US) today, a number that will nearly double in the next two decades. 1 Cancer and cancer treatment-related side effects adversely impact a majority of individuals during treatment, however persistent late effects can lead to distress and disability over the remaining lifespan for nearly 70% of survivors, negatively affecting participation in work, life roles, and activities of daily living (ADLs).2,3 The adverse sequelae from cancer and its treatments may impact multiple body systems and functions 4 including; cognition and memory,5,6 psychological functioning, 7 cardiovascular 8 and pulmonary, 9 musculoskeletal,10,11 and sensory/motor functions.12,13
Supportive care services such as social work, rehabilitation, nutrition, and behavioral health provide interventions that address the needs of cancer survivors and may reduce functional morbidity. 14 While services are commonly available in comprehensive cancer care settings, once patients conclude treatment and resume routine healthcare follow up in their community, specialized support services are lacking. 15 This is especially true in rural areas of the US, where access to supportive care providers with expertise in oncology is limited.16,17
Nearly 46 million individuals live in rural areas, as classified by the US Department of Agriculture Rural Urban Continuum Codes, and West Virginia is the third most rural state in the US. 18 Rural cancer survivors are disproportionately affected by a lack of community-based support services to manage their ongoing health needs after treatment.19,20 Further, support needs are magnified by sociodemographic factors prevalent in rural regions such as poverty, low health literacy, and poor health behaviors.18,21 Unmet needs lead to more medical visits, increased use of emergency care, and greater use of pharmacological interventions.22,23 The combination of these issues has led to urgent calls for developing better long-term survivorship care centered in the communities where patients live and work.24,25
Developing community-based survivorship care services requires a methodical approach to evaluate local community resources and patient needs and to address resource development tailored to local needs. 26 The aim of this research project was to understand the perspectives of patients, caregivers, and primary care professionals across the state of WV regarding the delivery of rural cancer survivorship care and to characterize unmet needs among individuals with cancer. The purpose of this manuscript is to share patient and caregiver perspectives on supportive care needs and care gaps as experienced in the rural state of West Virginia (WV).
Methods
The WV Cancer Survivors Needs Assessment Project assessed the perspectives of patients, caregivers, and primary care professionals (PCPs) regarding the delivery of rural cancer survivorship care using sequential mixed methods to survey and then interview eligible participants regarding unmet needs and gaps in survivorship care delivery. Our work was informed by Taplin et al.'s 27 multilevel framework for improving cancer-related health outcomes across the cancer care continuum, specifically focused on understanding patient-level, caregiver-level, and primary care professional-level perspectives on cancer survivorship care in the context of the patient's local community environment. This project was approved by the Institutional Review Board of West Virginia University (protocol # 1911779665). This manuscript presents findings from the patient and caregiver analysis only, PCP findings will be reported elsewhere.
Needs Assessment Survey Tool
The short-form Supportive Care Needs Survey (SCNS), a 34-item multidimensional survey tool uses a 5-point Likert scale to assess the extent of survivors’ unmet needs across five domains: Psychological, Physical and Daily Living, Patient Care and Support, Health System and Information, and Sexuality. 28 Residents of WV with a cancer diagnosis between 2015 and 2021 were invited to participate in this survey as were their caregivers, defined as any individual who participated in the patient's care. Participant demographics including gender, time since cancer diagnosis, race, ethnicity, education level, cancer stage and type were collected alongside the SCNS. Respondents self-identified as a patient or caregiver. The survey was populated in a HIPAA compliant Qualtrics database with a QR code generated.
Recruitment
A paper survey, including the QR code, and postage-paid return envelope were mailed to two thousand individuals with a cancer diagnosis from January 1, 2015 to December 31, 2021 as identified by the West Virginia Department of Health and Human Resources Tumor Registrar. To avoid multiple responses, instructions for participants asked them to either use the QR code or return the mailed paper survey. As an incentive, all survey respondents were given the option to enter a $50 gift card drawing. The drawing was conducted by the study PI at the close of the survey and 20 survey respondents were randomly selected to receive gift cards. Additionally, all respondents had the option to volunteer to participate in a 1:1 semi-structured interview, which offered a further $50 incentive for those who completed interviews. Since individuals are considered cancer survivors from the point of diagnosis, there were no exclusion criteria based on the treatment continuum of care. Any patient, at any point in their care continuum could participate.
Data Collection
Surveys returned by mail were hand-entered into Qualtrics. Survey responses were collected over six months. Individuals who volunteered for 1:1 interviews were contacted by the study coordinator to schedule a 30-min session. Interviews were exploratory and used a phenomenological approach to understand the participants lived experiences with survivorship care delivery. 29 The interview guide is provided as supplemental material. All interviews were conducted using the Zoom platform (DB, NS), recorded, and transcribed. Transcripts were reviewed for accuracy (MR, EB) and emergent themes were identified across two co-author teams (NS, MR and DB, EB).
Analysis
Patient and caregiver survey responses were analyzed separately. Missing data was handled by review of surveys. If >50% of the SCNS questions were incomplete or if all demographic data were missing, the survey was excluded.
Descriptive analyses were performed to summarize demographic and SCNS data, including frequencies, means, and standard deviations. SCNS subscales were analyzed across the total sample and compared by cancer type and stage. For analysis, the 5-point Likert Scale was collapsed into 2 categories: (1) No Need (1- Not applicable, and 2- Satisfied) and (2) Some Need (3- Low, 4- Moderate, 5- High). Frequency of needs across the subscales by disease types is reported and between group comparisons were analyzed by Chi-Square.
Between group comparisons were conducted based on education level by subscale using a Kruskal Wallis test and score differences between cancer stages were analyzed by subscales and by type of cancer also using Kruskal Wallis.
Thematic analysis of interview transcripts was conducted using an inductive descriptive phenomenological approach. 29 Contextualized themes of care gaps were identified and coded across interviews by one of the two study teams with discrepancies being resolved by the full author team. Content coverage of themes across interviewees was calculated using NVivo software and thematic quotes were collected. A second round of coding was conducted to identify contextual subthemes within each major theme.
Results
Four hundred and thirty-seven survey responses were received (21.8% rate of return). After removal of duplicates and incomplete responses, 362 patient surveys and 18 caregiver surveys were analyzed (18.9% response rate). Fifty-three responses were removed as incomplete mail in surveys. Four duplicate responses, identified in the electronic dataset, by individuals who completed the survey twice and self-identified for the incentive drawing were excluded. Forty-two (9.6%) responses were received electronically and the remaining surveys were received as mailed paper copies.
Patient Survey Results
The demographics for patient respondents are provided in Table 1 for the full group and by those reporting unmet needs. Respondents were an average of 2.03 years (SD ± 1.4, range <1-6 years) from cancer diagnosis. The majority of respondents were White (96.4%, n = 349) and 65% (n = 234) were women. One-hundred and fifty (41.4%) respondents reported high school as their highest level of education. Distribution across cancer stages demonstrates a slight negative skew (−0.177) towards higher stage respondents. The most common cancer diagnosis reflected by respondents were Breast (24.4%), Lung (13.9%), and Hematologic (13%). Notably 44.4% of respondents had advanced (stage III or IV) cancer.
Participants Descriptive Analysis by Overall SCNS and Moderate to High Needs Score (chi Square).

*statistical difference (p ≤ .05)
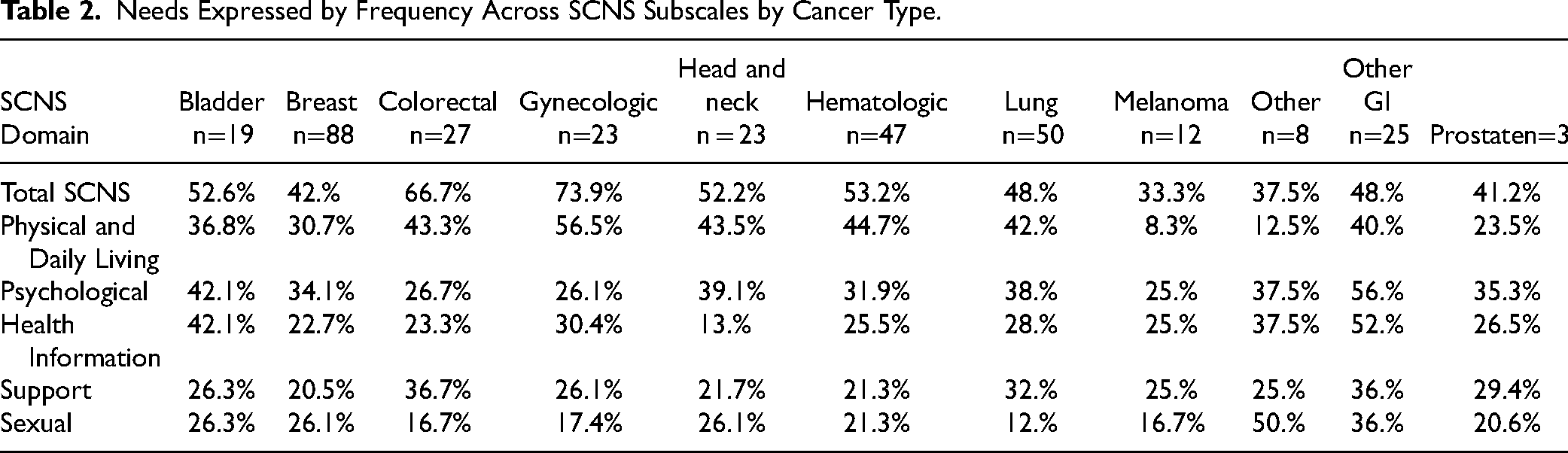
Overall, 49.5% (n = 179) of participants reported unmet needs on the SCNS most commonly in the domains of Physical and Daily Living (36.8%), Psychological (35.3%), and Health System and Information (27.4%). Frequency of unmet needs within each survey domain across cancer type is outlined in Table 2. Respondents with gynecologic and colorectal cancers ranked the highest needs scores across the 11 cancer types analyzed.
Needs Expressed by Frequency Across SCNS Subscales by Cancer Type.
Pairwise comparisons of unmet needs between stage, with adjusted p-values on Kruskal-Wallis tests, indicated significant differences between stage 0 and IV (P = .020), stage I and III (P = .0151), stage I and IV (P = .000) and stage II and IV (P = .006). (Table 3) Pairwise comparisons of unmet needs between education level with adjusted p-values on Kruskal-Wallis tests did not identify significant differences.
Unmet Needs Across Survey Domains by Disease Stage.

Abbreviation: SCNS, Survivorship Care Needs Survey.
Caregiver Survey Results
Eighteen respondents, 3 males and 15 (83.3%) females identified as caregivers and reported an average of 1.1 years since the time of diagnosis. All caregivers self-identified as White, and of Non-Hispanic ethnicity. Nine (50%) reported their highest level of education as high school. Six caregivers identified the stage of cancer to be Stage III or higher, 9 reported cancer stage as unknown. Descriptively, caregivers reported unmet needs are highest in the Psychological domain (72.2%) followed by Physical and Daily Living (38.9%) and Health System and Information (16.7%).
Qualitative Results
Forty-five individuals volunteered to participate in an interview, and all were contacted to schedule. Eleven interviews were conducted, 3 males, 8 females, averaging 1.3 years from diagnosis, the remaining 34 individuals did not respond to outreach to schedule an interview. Four content themes involving care gaps were identified (Table 4).
Frequency of Care gap Themes Identified Across Participant Interviews with Representative Quotes Based on Subtheme or Context.

Abbreviation: P, Participant.
The theme of Finding Support and Supportive Services was identified with 100% coverage across all interviews: specifically regarding support for care coordination, finding supportive services in a timely fashion, and finding local services. (Table 4) I just felt like there wasn't really any kind of support for my family…to know how to support me better…and I think if there was something that they could have went to, to learn a little bit more about what to expect and how they could help, I think that would've been helpful. (participant 11)
Many participants shared insights on how a family member or friend filled support care gaps. “we’ve had a lot of help from our children and even our in-laws, I have a grand-daughter-in-law…she helps with bills and things like that to make sure that it is all right, and the kids have helped with the finances and with driving me everywhere.” (participant 1)
Two participants reported having a case manager or navigator that coordinated care and connected them to support services.
The theme of Health Information Regarding Care Delivery and Continuity of Care was expressed with 100% coverage across all interviews. None of our participants reported receiving a survivorship care plan and most were uncertain about who to contact when problems arose, specifically as they transitioned from cancer care providers to primary care. (Table 4)
The theme of unmet needs in Health Information Regarding Symptoms and Symptom Management was reported across 90.9% of interviews. “…you don’t know what to do when things don’t get better. They say it will get better…you won’t be so tired, your fingers won’t tingle as much…but when it didn’t get better, and my (primary) doctor didn’t know what to do…does anyone even really know what I should do?” (participant 3)
Comments regarding Symptom Management reflected common and persistent issues that were routinely disabling, specifically persistent physical effects like fatigue, “brain fog”, lack of interest in participating in social roles, and lack of confidence to get through a task in the community, like grocery shopping, without help. In general, participants expressed surprise at the persistence of treatment-related physical symptoms and frustration with the lack of information shared about the risk for symptom persistence. Participants noted that information provided for symptom management was frequently inadequate, failed to help them develop realistic expectations about treatment, was difficult to understand, and was not easy to access.
In addition to distance traveled, two subthemes emerged regarding Geographic barriers, as expressed in 80.1% of interviews. First, the issue of repeated travel for supportive care services was a barrier to obtaining support. “It was one thing to have all that drive when I needed to get treatments, but then, ‘oh, come back to see our pain doctor, or our dietician…’ No way I could do it…and I couldn’t ask my husband to just turn around and keep driving me for all of these extra things…” (participant 6)
Second, the lack of broadband connectivity at the participant's residence limited access to supportive services outside of their communities. “…they wanted to call on a facetime and email me stuff and I was like I can’t do that, I’m not capable of that, I don’t have an internet here, I don’t even have a TV.” (participant 4)
Qualitative themes, subthemes, and exemplar quotes are outlined in Table 4 with full qualitative data provided as a supplemental document.
Discussion
Our findings highlight the unmet needs reported by cancer survivors living in rural WV and the gaps they experience in receiving supportive care. Survey respondents were on average 2 years beyond their cancer diagnosis and nearly 50% identified unmet needs on the SCNS, suggesting that needs related to cancer or cancer treatment sequelae can be persistent and multi-dimensional. This is supported by previous research citing long-term and late effects of cancer and cancer treatments.12,30,31 Insights gained from qualitative interviews provided context that the lack of local, community-based services and absence of health information regarding continuity of care may be drivers of unmet needs for individuals living beyond cancer treatment. This is concerning from a population health perspective, as the number of cancer survivors is expected to nearly double, to 28 M, by 2040 1 suggesting a growing morbidity burden and an escalating need for patients to access supportive services.
Beyond characterizing the magnitude of unmet need, our findings provide insight to the specific domains of needs that rural cancer survivors experience. The highest burden of unmet needs was reported in the domains of Physical and Daily Living, Psychological, and Health Information and Systems, these domains were also related to the topic themes identified through the qualitative interviews. However, in discussion with interviewees, there was a dominant theme of unmet needs regarding supportive care and support services. Interestingly, the interviewees overwhelmingly identified the lack of community-based services but also shared that their personal network of family or friends helped them overcome this care gap. This is an important point for consideration and suggests that care gaps in support services, such as transportation, largely exist but that individuals are relying on their own family and friends to provide these services. This is supported by past research which identified the lack of support services, like transportation, as a significant barriers to care, 32 sometimes resulting in patients not pursuing support services. 16
Interview findings agreed with survey responses that unmet needs in the Physical, and Psychological domains persisted beyond treatment. Long-term, unmet physical and psychological needs among cancer survivors are identified as contributing to poor quality of life and disruptive to patients returning to high levels of participation in life roles. 24 Interviewees provided context that needs were magnified by the fact that they could not find local support services to address these issues. Supportive services are characterized as “indispensable” in oncology care 33 and high quality, long-term survivorship programs are being developed to address these needs,14,34,35 however, most cancer survivorship programs are associated with cancer treatment centers and hospital systems making access a challenge for individuals who reside far from the cancer center. Even when community-based support services exist, they frequently are not tailored to the unique needs of individuals with cancer, creating a care gap.
The care gaps identified by our respondents are not unique to West Virginia, but evidence suggests they may be wide-spread across rural areas in the US.16,36 Provider density in rural areas means that healthcare professionals with experience in physical and psychological oncology supportive care are unlikely to be in the communities where rural survivors reside. 37 A recent analysis of oncology board certified physical therapists found low density across the central and rural areas of the US. 17 Additionally, the knowledge and skills of primary care professionals regarding the physical and psychological needs of individuals with cancer is remarkably low 38 suggesting that even in care settings close to the individual's home, they are unlikely to get evidence-informed information or interventions to meet their greatest needs. 39 Considering that physical and psychological needs were the highest experienced by our study population, and others, 35 this is a remarkable care gap in our rural communities.
Survey results also identified unmet needs in the domain of Health Information and Systems, further substantiating past findings regarding this gap.36,40,41 Interviewees provided important context around this need identifying that they lacked information about care planning and care delivery beyond active cancer treatment and did not fully understand their follow-up care plan nor who to contact regarding persistent unmet needs. Cancer patient navigators play an important role in providing care coordination during active, medically guided treatment, 42 however there is commonly no community-based point of contact to coordinate support services close to home after treatment completion. 43 Navigators in cancer care delivery can be healthcare professionals or lay persons who help to support the individual through the trajectory of cancer care.44,45 Navigators are effective to improve care gaps, specifically regarding health information and the complexities of the healthcare system. Evidence suggests that navigators are also effective to connect healthcare systems in primary care settings with community-based resources and should be considered to alleviate this care gap for individuals with cancer.46,47
Many interviewees reported that long distance travel for cancer treatment was burdensome but necessary. However, their tolerance to repeated travel for supportive services was diminished and many expressed frustrations that services were not available closer to home. Looking to community-based chronic disease management models 48 may be a path forward to promote a cohesive, guideline-driven approach to survivorship care. 49 Chronic care models are based on similar principles of addressing needs across functional domains but will require tailoring incorporate current cancer survivorship guidelines and checklists for survivorship care. 50
Our survey findings demonstrate differences in unmet needs by cancer type and by stage of disease suggesting that a one-size-fits-all approach to survivorship care is inadequate. 51 Medically-focused interventions such as continued cancer screening and evaluation for recurrence of disease 52 must expand to include assessment of psychological, social, sexual, and physical needs, recognizing that these needs may be met by providers outside of a medical clinic, such as a dietician, an exercise professional, or a community health worker.53,54 Encouraging multidisciplinary clinics 54 that include medical and community services is an opportunity, especially in rural areas where community providers are trusted by patients and more accessible to them.
These results guide us to potential priority areas for knowledge and skill development among the primary care and public health workforce and suggest areas of emphasis for resource and capacity building through local policy changes in rural regions. 26 Community-based survivorship programs improve compliance with evidence-based follow-up recommendations, positively influence patient self-management skills, and enhance the function and quality of life of survivors. 55 However, these programs currently lack standardization and role delineation across health care disciplines39,56 and are mostly centered around large health systems. 57 Developing community-based survivorship programs will require an assessment of existing community resources to determine optimal ways to implement survivorship care pathways 58 and expand workforce skills 59 so that evidence-based care can be provided. 38
Limitations
Although our survey responses represented communities across the state of WV, the response rate of <20% should lead to caution in extrapolating findings to all rural areas. Further, our qualitative themes were derived using inductive approaches across a small group of participants and require more robust, prospective analysis to contextualize care gaps and inform resource development within specific communities.
The cultural context and norms in rural Appalachia have been characterized and only very narrowly differentiate from US rural culture. 60 While cancer care delivery challenges in WV do not differ greatly from rest of rural America, 37 cultural context may vary across populations. Local cultural context including mistrust, health literacy, and perceptions of healthcare providers intent may have influenced our respondents. 60 Therefore, contextual analysis of community and population preferences is warranted when considering these results.
Conclusion
Across all types of cancer, nearly 1/2 of patients on average two years from their cancer diagnosis reported unmet need across multiple domains. A general lack of supportive care services and an absence of health information to inform patients on their care plan and follow-up care suggests a more robust supportive care system at the community level is needed. Cancer-specific community-based support services and workforce knowledge regarding cancer survivors long-term follow up is needed. These findings provide insight to the lived experiences of patients and caregivers and should inform community-based, cancer-specific resource development, facilitate educational initiatives, and catalyze future research.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735241239865 - Supplemental material for Unmet Needs and Care Delivery Gaps Among Rural Cancer Survivors
Supplemental material, sj-docx-1-jpx-10.1177_23743735241239865 for Unmet Needs and Care Delivery Gaps Among Rural Cancer Survivors by Nicole L Stout, Dannell Boatman, Madeline Rice, Emelia Branham, Meadow Miller and Rachel Salyer in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735241239865 - Supplemental material for Unmet Needs and Care Delivery Gaps Among Rural Cancer Survivors
Supplemental material, sj-docx-2-jpx-10.1177_23743735241239865 for Unmet Needs and Care Delivery Gaps Among Rural Cancer Survivors by Nicole L Stout, Dannell Boatman, Madeline Rice, Emelia Branham, Meadow Miller and Rachel Salyer in Journal of Patient Experience
Footnotes
Author Contributions
Concept development NS, DB
Study methods development and data collection, NS, DB, MM, MR, EB
Data analysis NS, RS, MR, EB
Manuscript development NS, DB, MR, EB
Figures and tables NS, RS
Final review and approval of manuscript, all authors
Declaration of Conflicting of Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NS: Speakers honoraria from Medbridge Inc, GreatSeminars LLC
DB, MR, EB, MM, RS: none
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by National Institutes of General Medical Sciences, (grant number U54GM104942). The project described, and the results presented are the opinion of the authors and do not represent the official views of the NIH.
Ethical Approval
This project was approved by the Institutional Review Board of West Virginia University (protocol # 1911779665).
Statement of Informed Consent
Survey respondents provided written consent if responding on paper versions, e-consent if responding to the electronic survey.
Participants in qualitative interviews provided verbal consent at the start of their recorded interviews.
Statement of Human Rights
No experimental procedures were performed on study participants. All study procedures were conducted in compliance with the Declaration of Helsinki principles.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.