
Abstract
This qualitative study sought to answer three questions: What is it like to live with rotator cuff tendinopathy? What are the barriers and facilitators of a healthy lifestyle with an aging shoulder? And, what are the outcomes that matter most to people seeking care for rotator cuff tendinopathy? Patients diagnosed with rotator cuff tendinopathy participated in group discussions using semi-structured guides that focus on diagnosis, daily experiences living with rotator cuff tendinopathy, goals, concerns, and clinical care experiences. A hybrid of initial inductive coding of themes and subsequent deductive consideration of these themes within the capability, comfort, and calm framework was utilized. Themes associated with rotator cuff tendinopathy were less restful sleep, difficulty with work and life transitions, loss of baseline abilities, and limitation in social roles in the capability realm; physical pain, despair, and loneliness in the comfort realm; and lack of direction or progress and feeling uncared for in the calm realm. Barriers identified included: the sense that rotator cuff tendinopathy is something correctable rather than age-associated and the sense that painful activities will make the tendinopathy worse (common misconceptions); tenuous relationships and limited trust with clinicians; loss of hope; and a sense that care is directionless. What matters most to a person seeking specialty care for shoulder pain are feeling that they are getting effective care and not being dismissed; maintaining meaningful activity and life roles; and replacing despair and frustration with hope and progress. Anticipating these needs may facilitate the design of more effective care models.
Keywords
Introduction
This qualitative study focuses on the daily experience of living with rotator cuff tendinopathy (RCT). When patients with a similar condition share their experience with each other in small groups (a so-called “experience group”) (1) the discussions often unearth things patients do not tell their doctor. Musculoskeletal specialists stand to benefit from this information because understanding what matters most to a person seeking care is a key aspect of a therapeutic relationship and helps ensure that care strategies work toward patient goals. Knowledge derived from qualitative research can help clinicians identify and address common gaps in care for people with RCT, informing new approaches that achieve better outcomes and experience.
Shoulder pain is common and increases in incidence as people age. RCT is, by far, the most common reason a person with upper limb pain seeks care (2). Two different theories exist regarding the pathophysiology of RCT: 1. Expected age- and gene-related thinning of the rotator cuff tendons; and 2. Impingement of the tendon between the humerus and scapula (acromion and coracoid) with overhead activity. Current evidence favors the former (3,4).
Although some people have acute defects after an injury, most defects occur over time, unrelated to injury or activity. Most thinning and defects cause few symptoms. By age 80 more than 60% of people have rotator cuff pathology on imaging (3,5,6).
Rotator cuff defects can get large enough to limit active motion. The largest defects are associated with rotator cuff arthropathy, a form of shoulder arthritis. To date, we do not know the factors associated with an increase in defect size (3). The ability of exercises (7), injections (8), and surgery (9–11) to alleviate symptoms or change the natural history of the pathology is still open to debate (3).
The current understanding of the experience of living with RCT is primarily derived from studies that use questionnaires (patient-reported outcome measures) to quantify the illness experience. From these studies, we know that an individual's experience of this disease often does not correspond with the pathophysiology (12). For instance, tendon defects tend to enlarge slowly over time, but symptoms often resolve (13,14). New pain can cause RCT to seem like a new problem when the asymptomatic shoulder has comparable degeneration (15,16), which is consistent with the known tendency for humans to misinterpret new symptoms as representing new pathology (17). Even if the pathology is not worsening, painful movement may feel harmful as embodied in the well-studied unhelpful thoughts of kinesiophobia and catastrophic thinking, creating or reinforcing a sense of vulnerability (18). Stress, distress, and misconceptions—more so than measures of pathophysiology—are often the factors most strongly associated with variation in symptoms intensity and activity intolerance (18). These aspects of human illness often go unaddressed in patient–clinician interactions.
To better understand the experience of people seeking care for RCT, we invited people with RCT to discuss their symptoms in groups to answer the following questions: What are patient perspectives on living with RCT? What are the barriers and facilitators of a healthy lifestyle (experiencing capability, comfortable, and calm) with an aging shoulder? What are the outcomes that matter most to people seeking care for RCT?
Methods
This study was approved by our Institutional Review Board. Experience Group sessions are a qualitative research method designed to gather insight on the health outcomes that matter most to patients who share specific medical and life circumstances and the gaps or obstacles that may impede the achievement of those outcomes. The group sessions are designed to collect information on 3 dimensions of health: capability (ability to function and do the things that are important to the patient), comfort (reduction of physical or mental suffering), and calm (reduction of stress, chaos, and inconvenience from the process of receiving medical treatment) (19).
Each 60- to 90-min session brings together <10 people who share similar medical circumstances to have a conversation about their daily experiences living with their health condition, as well as their goals, hopes, and concerns. During the session, 2 experienced and trained male PhD facilitators encouraged participants to discuss their experiences both inside and, in particular, outside the clinical setting. This focus on lived experience fosters insight into the successes and the challenges faced in situations that are less observable by clinicians. The interviewers are not known to the participants and have little knowledge of RCT.
Each experience group session uses a semi-structured interview guide organized around specific discussion topics, which are posed to the participants as open-ended questions. This established methodology seeks to encourage conversation among the participants, including previously unarticulated issues of concern. Facilitation focuses on enabling participants to self-select the issues, experiences, and moments of importance to them. Facilitators took notes during the sessions. Each group's conversation was audio-recorded and transcribed verbatim. Participants did not review the transcripts or provide feedback on the findings.
Purposive sampling was used to recruit patients diagnosed with RCT who visited our unit within the prior year. The protocol allowed us to use billing records to identify patients and contact them. All identifiable health information was on password-protected servers. Nineteen people were contacted by phone and agreed to participate in the research. Three sessions were conducted in person, in a conference room, in English (a 5-person, 4-person, and 7-person group). Additionally, 3 people whose primary language was Spanish participated (a 2-person group and a 1-on-1 interview). No one other than the facilitators and participants was present. The mean age of the 10 women and 9 men was 54 years with a range from 31 to 75 years. Six participants identified as Latino/Hispanic, 8 as white, and 2 as black or African American, and 3 did not offer a racial or ethnic identification. One patient had prior surgery for shoulder pain. All participants were compensated with a grocery store gift card. There were no repeat interviews. After 19 people participated the facilitators agreed that data saturation had been reached with no new themes arising.
Analysis
Interview transcripts underwent thematic coding separately by 2 researchers using NVivo (QSR International; Melbourne, Australia), a qualitative data analysis software. Throughout the coding process, themes were cross-checked and compared for differences and similarities. After the initial round of inductive thematic coding, the data went through the second round of analysis in which we organized outcomes and insights about unmet needs and obstacles using the previously mentioned framework of capability, comfort, and calm.
Results
Outcome Themes
The following themes were identified in the experience of living with RCT (see Tables 1-3 for representative patient comments).
Representative Quotes.

Representative Quotes: Gaps in Care.
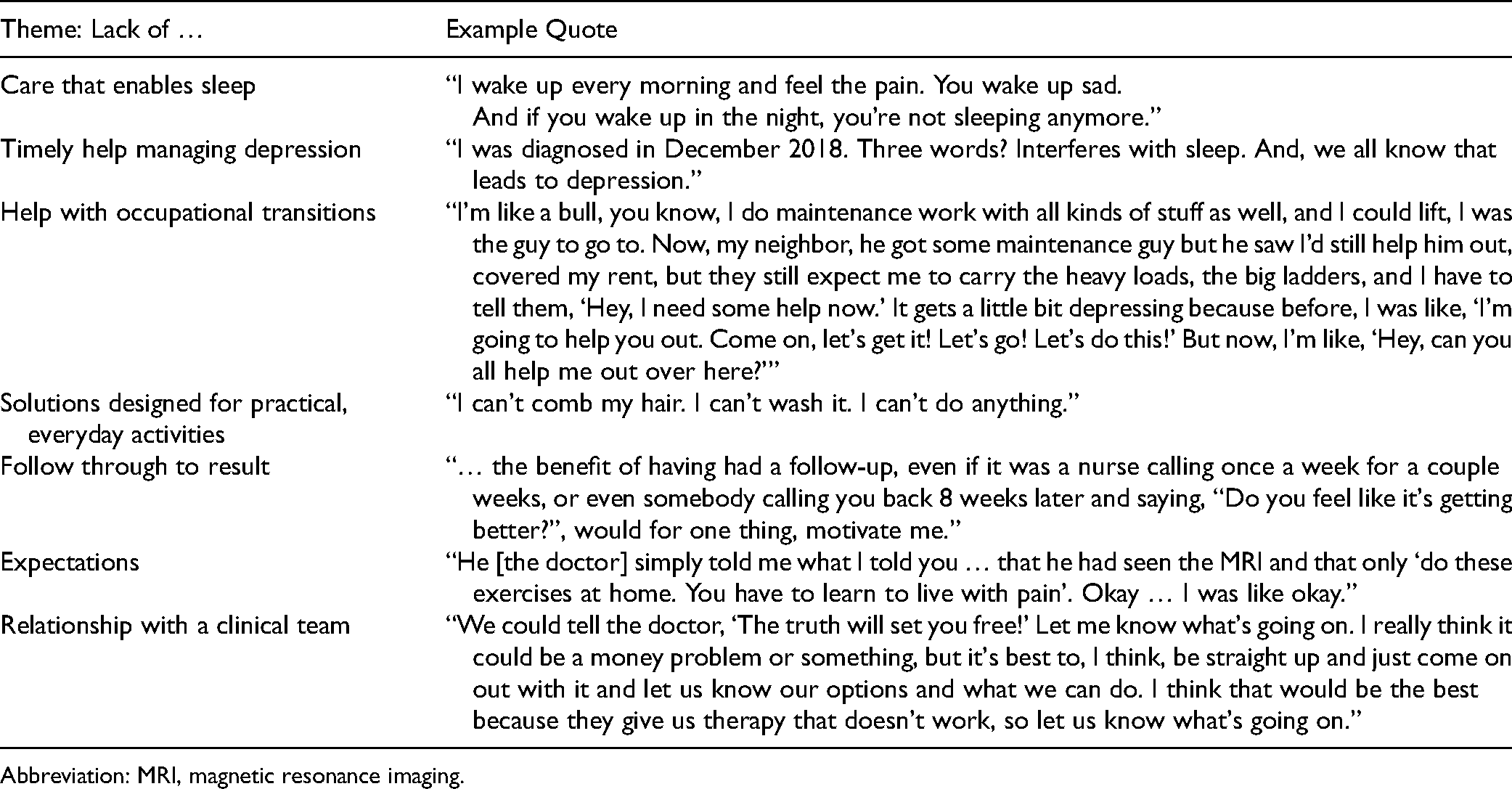
Abbreviation: MRI, magnetic resonance imaging.
Capability (Table 1)
One theme that emerged was a desire to get back to regular sleep patterns. RCT is known for being more painful when people are recumbent. Participants related that the condition was particularly problematic when trying to sleep.
A second theme was finding suitable work. RCT is part of the age-related bodily changes that can make it difficult to earn a living in a labor occupation after age 50. Participants talk about fears and frustrations regarding how they would support themselves and their families.
The third theme was regaining identity, both at home and at work. Participants expressed the desire to be able to do the things they perceived as core to who they were prior to the shoulder pain. People who self-identified as “construction worker,” “athlete,” or “handy person” expressed a sense of despair in the loss of flexibility, agility, strength, and comfort that can come with age in general and RCT in particular.
The fourth theme in participant comments was difficulty engaging in meaningful activities with loved ones, such as playing with grandchildren, engaging in sports, and helping with home projects. Avoidance of these activities contributed to feeling disconnected, isolated, or alone.
Comfort (Table 1)
Two themes were placed within the comfort domain. First, many participants reported that their shoulder problem made them feel down, fatigued, hopeless, and lost. They long to get their prior energy back and want to be able to look to the future with hope.
Second, people voiced frustration with the pain associated with treatment, particularly exercises often used in treating rotator cuff disorders to strengthen the muscles of the shoulder girdle. These exercises can be painful, which may feel unhealthy. Participants reported feeling less healthy as their days were filled with more painful activities as well as the achy aftermath of those exercises. For many, the pain seems to signal a lack of progress in treatment, adding to a sense of futility and suffering.
Calm (Table 1)
Patients with RCT seek care that has clear health goals. Clinician explanation of changes as “age-appropriate” sounds to many participants like they are being cast aside as they grow older. Participants also reported that having their pain explained as a normal aspect of aging seems to trivialize the problem. In addition, the focus on exercises as treatment makes many individuals feel that they are being blamed for not doing enough, especially given that exercise does not yield immediate alleviation of symptoms.
Many participants reported placing hope on imaging to identify a problem that could be fixed with injection or surgery. Some participants expressed feeling neglected or mistreated if clinicians do not order imaging.
Barriers to Health
An analysis highlighted the challenges that keep people from achieving the health outcomes they seek (Table 2). A key theme is that RCT can seem related to an event rather than an ongoing change in the body, so participants can feel frustrated with a perceived lack of recovery. Participants expressed that painful daily activities and exercises meant to help can feel like they are adding to the damage. People often feel they are not getting the attention and care they need.
Representative Quotes: Barriers to Health.

Abbreviation: MRI, magnetic resonance imaging.
Gaps in Care
Some people with RCT said the care they received did not provide adequate support for restful sleep, practical everyday activities, and occupational transitions (Table 3).
Discussion
Effective care is founded on an understanding of patient experience and priorities. Gathering people to talk about an illness they share can elucidate what outcomes they most desire from their care and what needs remain unmet in achieving those outcomes, directing clinical teams to potential improvements that often include better coordination and collaboration. The themes identified may not be the typical topics of discussion in musculoskeletal specialty visits: worthiness, life roles, and hope.
The decrements in health associated with RCT took the form of less restful sleep, difficulty with work and life transitions, loss of baseline abilities, and limitation in social roles in the capability realm; physical pain, despair, and loneliness in the comfort realm; and lack of direction or progress and feeling uncared for in the calm realm. Attentive specialists tend to organize care formulaically: establish the diagnosis, institute a treatment, assess, and consider another treatment. Specialists may prioritize the next set of exercises, medicines, and surgeries that can palliate or alter the natural history of the disease. The results of this study suggest that the people they treat are thinking more narratively. They are living a story—in variable degrees of pain, isolation, and despair. This suggests new approaches for teams that care for people with RCT such as allowing people to tell their story (narrative medicine (1)), empathic noticing and legitimizing (relationship building), and guiding rather than directing people to healthier ways to think, feel, and behave with this illness (motivational interviewing techniques).
The identified barriers to health among people who seek care for RCT—including cognitive bias (e.g., “hurt equals harm”) contributing to misdirected hope (i.e., “I need to get the problem fixed”); tenuous relationships and limited trust; and loss of hope and direction—suggest a need for more effective communication and care strategies. During specialty care, planned and practiced communication strategies can help people understand and accommodate RCT. It may help to explain the problem in increments, separated by time, giving people adequate time to absorb and reflect on the information that is unexpected and counterintuitive. For instance, a first visit might describe the anatomy and age-associated changes. Patients might be given something to read or watch to build their understanding and gently correct common misconceptions. If they feel ready, they could be taught a few simple exercises to do on their own. The care needs to be warm and feel continuous. Another check-in a few days later, by phone, video, or in person, could allow people to ask questions, express emotions about what they are learning about their body, and confirm that (painful) exercises are helpful rather than further damaging. At each point of contact, the ways that people manage RCT successfully could be reviewed as the patient shows curiosity. Based on learnings from our participants, this type of gradual, relationship-building care has the potential to ease people's sense of frustration connected to an overall limited understanding of the condition and limited expectations for the future.
Easier access to specialty expertise via asynchronous text, email, or medical record-based communication portals, and synchronous chat, audio, or video check-ins might also help. Increasing the number of ways to access specialty care and making communication more convenient for patients might help them to feel more cared for. An increased number of touchpoints with clinicians might help to improve the patient–clinician relationship, and trust in particular, which is often lacking based on the experiences documented herein. This points to the opportunity for interdisciplinary, team-based care. A shoulder team member, such as a physical therapist, health coach, or social worker could be introduced at the first visit and then keep in touch with the patient regularly to support progress.
Given the prevalence of RCT, it is likely that many people manage without specialty care. For people that are searching the internet about their sore shoulder, experts can make accurate, reassuring, and hopeful information easy to find. Expert information can be crafted to facilitate the process of adjusting to an aging shoulder. One key element is to explain RCT in a way that makes it easier to reorient common misconceptions about pain. Non-specialists may share some of these misconceptions, and specialists can be more deliberate about helping non-specialists gain a more healthful understanding of the aging shoulder. Clinicians will benefit from anticipating what matters to a person seeking specialty care for their injured shoulder.
The patient–clinician relationship deserves priority, given that validating despair and frustration, correcting common misconceptions, and guiding people away from tests and treatments that are unlikely to improve health are learned skills that most surgeons have not sought or practiced. Traditional management of RCT might reinforce existing gaps in care if surgeons and care teams assume that alleviation of pain will address all the outcomes people seek, such as restful sleep, normal daily activities, and occupational transitions. People with pain from RCT are learning how to manage their aging body. They need support, guidance, and planning to age gracefully, evolving their identity to match their body. Specialists may not be trained to address these aspects of human health. Employing other team members—such as social workers, psychologists, and physical therapists trained in techniques for guiding people to healthier thoughts—could help people feel better and do more, while allowing clinicians to focus on the things that they are trained to do, enhancing the joy in their work. Plus, as long as the team has a sufficient volume of patients, the per-patient cost is lower when the specialist's time and expertise are leveraged through team members.
Limitations of this research include our use of a group of people with the time and motivation to participate. In particular, we had relatively few Spanish speakers, so additional experience group sessions might highlight further themes. Because this is qualitative data, we cannot determine the prevalence of these themes and sentiments or their relative influence among all patients seeking care for RCT. However, while our participants’ life situations might not be representative of all patients seeking care for RCT, their sentiments and experiences seem to represent common themes, as they are consistent with experience from clinical practice and evidence from other sources (3,5,7,9).
A strong patient–clinician relationship also has potential to help patients make sense of pain. As noted above, people seeking care for RCT often misperceive their condition. A new pain may feel like an injury; a gradual onset of pain might feel like accumulating damage. The realization that pain is due to a gradual onset condition that is age-appropriate can be counterintuitive. A strong therapeutic relationship—one that includes trust, common understanding, and engagement—can help patients develop healthy thoughts (e.g., “Even though this hurts, I can get through it”), an adaptive mindset, and a supportive environment—all of which can limit symptom intensity and activity intolerance as one ages (12,20,21).
The patient perspective brings to the fore the importance of mental and social health. Formulaic biomedical approaches such as the stepladder of pills, shots, exercises, and surgery may not adequately address the despair, loss of identity, loneliness, and aimlessness that also represent health opportunities. There is experimental evidence that biomedical interventions such as corticosteroid injection and subacromial decompression may not outperform simulated injection and surgery (placebos) (8,9,22). There are also questions about the potential for benefit from surgery to address tendon thinning or small tendon defects in the rotator cuff as well as large defects with associated muscle deficiency (3). On the other hand, there is growing evidence that genuine, trusting patient–clinician relationships; connectedness, meaning and purpose in daily life; and healthy thoughts and emotions help people accommodate age, disease, and injury while reducing symptoms and limitations (the so-called placebo or meaning effect (23–25)). Understanding patients’ perspectives can inform the design of services that improve care and better achieve these aims.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by our Institutional Review Board.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with our Institutional Review Board's (2018-04-0132) approved protocols.
Statement of Informed Consent
Verbal informed consent was obtained from the patients for their anonymized information to be published in this article.