
Abstract
Chemoradiotherapy treatment for glioblastoma causes acute and long-term toxicities, negatively impacting quality of life. Patients require evidence-based, yet understandable information regarding treatment-induced toxicities to increase preparedness for treatment. A repeat cross-sectional, qualitative design was used. Semi-structured interviews were conducted with glioblastoma patients and their caregivers at set timepoints: prior to (T1), during (T2), and post (T3) chemoradiotherapy. Interviews were recorded, transcribed verbatim, and thematically analyzed. In total, 19 patients and 12 caregivers were interviewed. Three main themes emerged. (1) Navigating information materials, (2) Lack of awareness and understanding of chemoradiotherapy-induced toxicities, (3) The actual experience and impact of chemoradiotherapy toxicities. There is a discrepancy between the treatment information materials provided and patient expectation and experience of toxicities during and after chemoradiotherapy. Current informational resources do not adequately prepare patients or caregivers for the reality of treatment-induced toxicities. Better tailored resources are needed as individual needs fluctuate across the treatment trajectory. Further cross-center investigation is required to understand how we best create a personalized information pathway for glioma patients.
Keywords
Introduction
Malignant primary brain tumors account for 3% of total UK cancer cases, with approximately 12 000 new cases in the UK/year, and roughly 80% of these are classified as diffuse gliomas. 1 Glioblastoma is the most common primary brain tumor in adults. 2 This diagnosis is usually fatal, offering a poor overall survival of 10-14 months after treatment and causes significant impact to quality of life.
Standard of care treatment includes initial surgical resection, which represents a delicate balance of maximizing the extent of resection and minimizing neurological deficit, followed by radiotherapy; a targeted treatment that delivers ionizing radiation with accuracy and precision, given with concomitant temozolomide (TMZ) and adjuvant TMZ. 3 Chemoradiotherapy is a critical component in the treatment of glioblastoma, although substantial acute and late toxicities must be carefully considered. 1 Despite a multi-modal treatment approach, local recurrence is almost universally expected. 4
Symptom burden can be extremely high in glioblastoma patients and can vary greatly across disease phases, 5 often including impaired cognitive function, confusion, and language difficulties. 6 Additionally, caregiver burden is high, which negatively impacts on caregivers’ ability to provide care and support.7–9 Caregivers require education and support, not only to better help the patient, but to also reduce their distress. 10 Tailoring information and education resources can enhance preparedness of expected toxicities, managing toxicities and how they may impact physically and psychologically. 11
In the context of glioblastoma, language barriers, cognitive difficulties, reduced health literacy, or limited numeracy12–14 can impact on patient and caregiver understanding, particularly burdensome factors. Moreover, patient understanding or retaining of health information is known to show some discrepancy with healthcare professional delivery of information, particularly in patient groups with cognitive deficits. 15
Standard information delivery involves word-heavy booklets regarding diagnosis, symptoms, and treatment options, which is supported by verbal information from clinical experts. Some variances between centers are inclusion of medical infographics, 16 educational videos created by healthcare delivery teams, 17 and telephone clinics. 18 In our center, only written information materials are used, supplied with verbal explanation. We aimed to review chemoradiotherapy-related resources before, during, and post-chemoradiotherapy and evaluate, to what extent, patient and caregiver informational needs are being met.
Material and Methods
Study Design
This single-center, prospective, repeat cross-sectional service evaluation adopted a qualitative methodology involving semi-structured interviews and thematic analysis, underpinned by a reflexive approach.19,20 As this project was classed as a non-research-based service evaluation, ethical approval was not a requirement. 21 However, we still followed good clinical practice guidelines, and the project was conducted in accordance with the 1964 Helsinki declaration and its later amendments. Caldicott approval for use of patient data was provided by our National Health Service (NHS) Trust Research and Innovation research governance team (Ref. AG 24-09-2020).
Setting and Recruitment
Between February 2020 and November 2022, patients eligible for radical chemoradiotherapy and their caregivers were recruited from Leeds Teaching Hospitals NHS Trust. Participants were invited to take part in semi-structured interviews either: prior to commencement of chemoradiotherapy (T1), 2-3 weeks since commencement of chemoradiotherapy (T2), or 6 weeks post-completion of chemoradiotherapy (T3). A different sample was recruited for each timepoint to analyze variation of experiences over time, while completing data collection within the study fieldwork timeframe of 6 months.
Patient eligibility criteria included: 1) a histologically confirmed primary WHO grade 4 glioma; 2) eligible for standard of care treatment; 3) ≥18 years; 4), able to understand and speak fluent English; 5) willing to take part in and attend a face-to-face interview. Caregiver eligibility criteria were 1) ≥18 years; 2) identified by patients as the primary person who provided support; 3) willing to take part in and attend a face-to-face interview. It was not a necessary requirement that one needed to consent for the other to be included. Participants were given verbal and written study information, and all provided written consent.
Sample
Purposive sampling was used to increase sample heterogeneity in terms of age, gender, and tumor location and to highlight potential differences in severity of treatment-related toxicities based on participant experience. We did not set an intended sample size but aimed to perform interviews until saturation began. Under the framework of thematic analysis, saturation denotes the point at which no further themes or patterns are discerned from the data. 22 The final sample size was 31 (19 patients; 12 caregivers).
Data Collection
Interview topic guides were developed based on findings from a retrospective audit which evaluated whether modern radiotherapy delivery techniques influence the severity of treatment-induced toxicities, 23 and with input from clinicians, experienced researchers, and patient representatives to cover: 1) the expectations and experience of presenting symptoms and treatment toxicities; 2) how toxicities impacted on quality of life; 3) whether the information provided met patient and caregiver needs. A full topic guide is presented in Supplementary File 1. A summary of key questions is presented in Figure 1. Interviews were performed by the lead researcher, who was involved in patient care, with supervision and support from an experienced researcher.
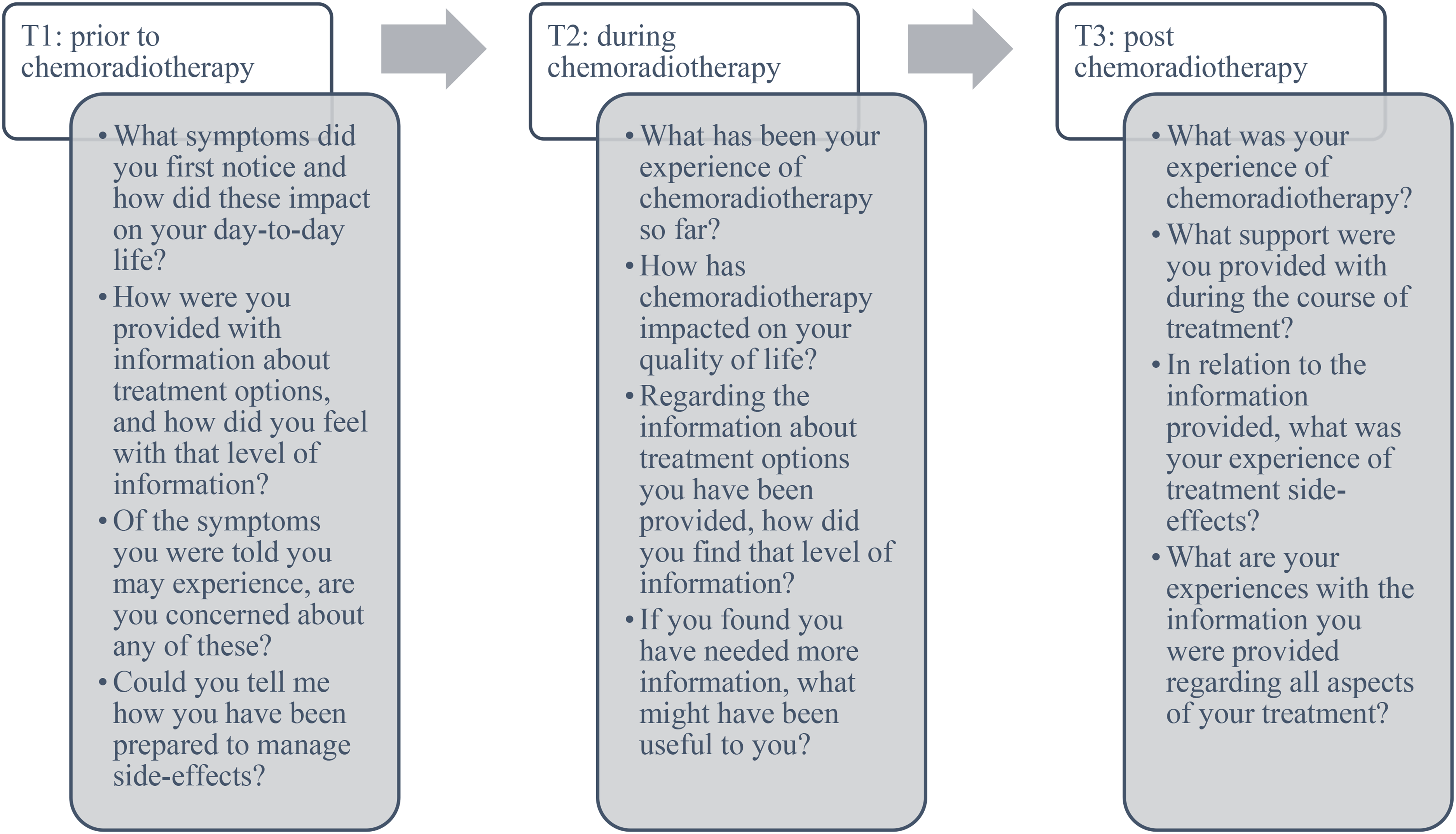
Summary of key interview questions asked at differing timepoints.
Analysis
Interviews were transcribed verbatim manually by the lead researcher and analyzed using a thematic analysis framework. 19 Familiarization with the data started at interview and transcription, after which the lead researcher read each transcript thoroughly. All transcripts were independently coded using an inductive approach to allow meaning to emerge from the raw data and to fully understand participant experience. An iterative process was followed whereby codes were assigned for the selected texts and categorized into themes and subthemes, while being constantly reviewed against the data.
To organize the data effectively, a codebook was created. A preliminary coding scheme was developed after identifying major themes. The second researcher independently verified the generated interpretations of the data after every three transcriptions had been coded.
A reflexive approach was followed to acknowledge the researchers’ active role in production of codes. Considering the different backgrounds of both researchers, the lead researcher has a radiographer background involved in clinical care, the second researcher has a psychology background, not involved in clinical care; this highlighted the researchers’ interpretations of meaning across the dataset. The researchers frequently met to discuss coding and to refine the codebook for the next transcripts. However, reaching consensus was not a required endpoint. 19
Results
In total, 19 patients with a confirmed diagnosis of glioblastoma and 12 caregivers were interviewed (n = 9/n = 5 prior to chemoradiotherapy, n = 5/n = 4 during chemoradiotherapy, n = 5/n = 3 post-chemoradiotherapy). Patients and caregivers were interviewed together when both consented. There were 12 male patients and 7 female patients; the median age was 61 (age range 32-79). Detailed participant characteristics can be found in Table 1.
Participant Characteristics.

TMZ, temozolomide.
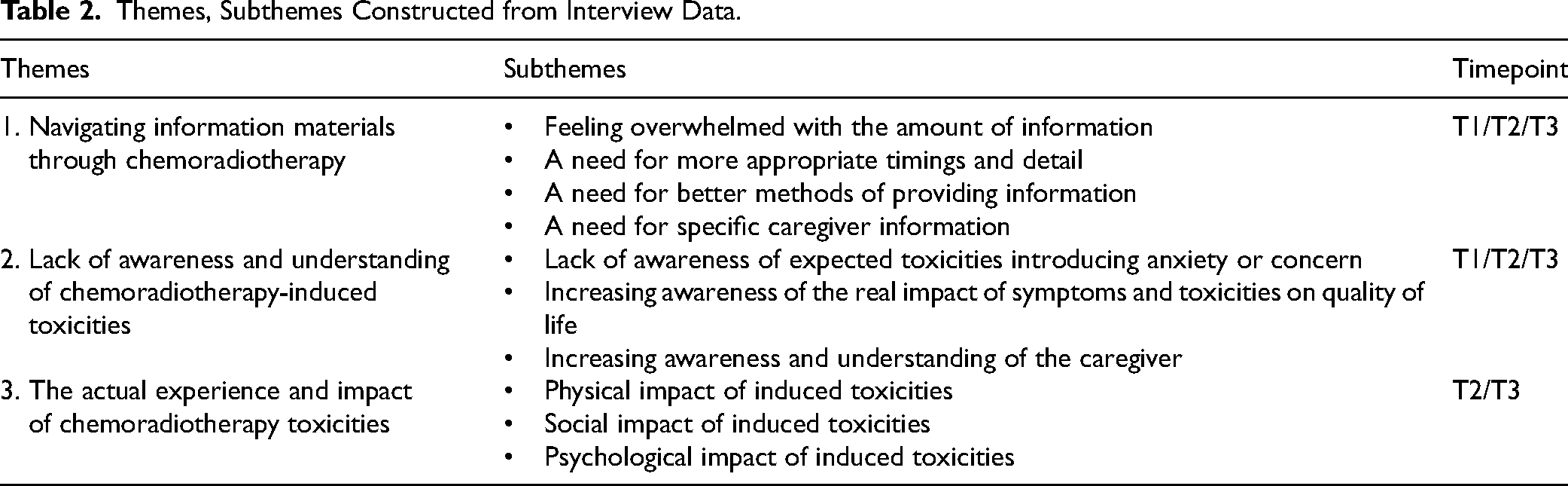
Interviews took on average 37 min (range 17-61 min). Three main themes emerged from the data and are described in Table 2. The variation of patient and caregiver experiences between timepoints is highlighted where applicable.
Themes, Subthemes Constructed from Interview Data.
Navigating Information Materials—T1/T2/T3
This theme was key for highlighting the difficulties patients and caregivers faced navigating through extensive information materials they were offered at the beginning of the treatment pathway. Generally, patients and caregivers expressed feeling overwhelmed with the level of generalized information offered. This information, which did not always fit with their symptomatic profile, caused increased anxiety. Patients wished for more tailored detail regarding probable treatment toxicities. This was noted across all successive timepoints, but particularly in relation to T1.
“…it is a lot of information; it is a lot to take in. I suppose it depends on the patient as well… some people might want to read every single word and then panic about it; others might want to go away and Google but that's- I think that's the worst thing you can do.” (Patient 8, male, 50, T1)
“…I’ve had numerous consultations and meetings with different doctors at different hospitals and sometimes information is given to you repeatedly, when you don’t necessarily need so much so quickly.” (Patient 13, male, 36, T2)
As changes in information seeking behaviors and personal experiences of treatment and treatment recovery vary, both patients and caregivers thought it would be highly useful to phase or layer tailored information at various timepoints throughout the disease course (T1/T2/T3). Providing personalized resources at differing stages of the treatment pathway, or as needed could improve patient understanding.
“It might be useful to know what you would expect to see at different times.” (Patient 18, female, 61, T3)
“To give information out different stages, that could be good, yeah. Just do an introductory one to start with and then more detailed one's going through that fit with their needs at that time.” (Female caregiver of patient 16, T3)
“You do sort of read them, put them to one side and you don't really think to pick them up again. And I think perhaps you also don't know what questions… to ask at that point.” (Female caregiver of patient 16, T3)
“I think to be honest with you, at the time there was so much going on and the shock of everything… we probably wouldn’t have remembered it anyway if they had of told us.” (Caregiver of patient 17, T3)
Lack of Awareness and Understanding of Chemoradiotherapy-Induced Toxicities—T1/T2/T3
Evident at all successive timepoints (T1/T2/T3), a lack of understanding and limited awareness regarding acute toxicity severity was something that all participants displayed. This in-turn, increased anxiety and negatively impacted on patient preparedness of expected toxicities.
“I’m a bit anxious about the radiotherapy starting next week, just because I don’t know what to expect… and I’d like to know. I’d love it for somebody to be able to tell me that you’ll feel this ill, on this week, for this length of time and then you’ll be alright (laughing)… it's that unknown… that's just causing a bit of anxiety.” (Patient 4, female, 40, T1)
Informational needs evolved along the disease trajectory due to acute location-specific side effects. During chemoradiotherapy (T2), participants found the detail provided in written materials to be generic and lacking information specific to their evolved needs and tumor location-specific toxicity profile.
“I didn't know what I would expect. There were a lot of side effects on the sheets that haven’t been relevant. It's the unknown that scares me more than anything else because I don't know what's going to come next.” (Patient 13, male, 36, T2)
Both patients and caregivers expressed a desire to be educated on the factors influencing treatment recovery as recovery length varied significantly between individual patients. Prior to chemoradiotherapy (T1), participants explained that they were given an estimated timeline of when treatment toxicities should likely subside. During the interviews, participants explained the variations they had had in terms of their recovery trajectories. Some experienced unexpected and adverse effects from chemoradiotherapy, which in some cases, prolonged their recovery time post follow-up (T3). In general, recovery time was longer than expected, which led patients to question why their acute effects were not improving: “…they said during the treatment that I could expect the symptoms to last beyond the end of the treatment date. But they said they would last for about 3, 4, 5 weeks after and I think in reality it was more like 8 weeks.” (Patient 18, female, 61, T3)
The Actual Experience and Impact of Chemoradiotherapy Toxicities—T2/T3
During chemoradiotherapy and into the follow-up phase (T2/T3), a lack of patient preparedness was evident, which is something that was not evident at the T1 phase. Patients stated that they would have appreciated some form of written or verbal information at T1 to increase their awareness of how chemoradiotherapy side effects would impact day-to-day life. Both patients and caregivers were not prepared for the real-life impact of treatment-induced side effects.
“…my ability to concentrate or focus on something for as long as I used to do, has gone.” (Patient 9, male, 58, T1)
“…that's one thing I didn’t expect… my tolerance levels have got… they’re not as good as they used to be – like I'll snap more now than I ever used to do, which I try to keep under wraps and little things will just set me off when they didn’t before.” (Patient 13, male, 36, T2) “I think the side effect information needs to be more prominent to be honest, I think they really do, especially with the sickness and the nausea and the- I think it needs to be more detailed.” (Patient 16, male, 70, T3)
“I find that the confusion symptoms do impact me every day.” (Patient 18, female, 61, T3)
“I’m having to be the nurse if you like, because I don’t think he’d manage it on his own really. You know this regime of the times and all that sort of thing…” (Caregiver of patient 12)
Discussion
Our study identified a need for improving education and information materials that are tailored to the individual patient diagnosed with glioblastoma. This is also relevant for their caregivers as they need more supported education. Findings are extremely pertinent to the progression of truly patient-centred information and support and is a key part of enhancing patient preparedness, patient satisfaction and reducing patient and caregiver anxiety.24–26
The main themes found were (1) Navigating information materials, (2) Lack of awareness and understanding of chemoradiotherapy-induced toxicities, (3) The actual experience and impact of chemoradiotherapy toxicities.
Navigating Information Materials
Evident at interviews prior to commencement of chemoradiotherapy, and consistent with other studies,27,28 we found that all participants referred to feeling overwhelmed when presented with a wall of information post-diagnosis. This made navigating through written information materials more difficult. While verbal information is easier to tailor, but this is not something patients, nor caregivers can continuously refer to which limits self-management and patient activation. Particularly for patients with cognitive difficulties, resources should be easily interpretable and manageable to comprehend. 29 Patients and caregivers in our study highlighted the importance of needing individualized support, considering their fluctuating needs, 30 to feel better prepared during and post-treatment. Providing phased, adaptable information and support, based on individualized need and preference, will aid navigation of information materials and should be a requirement for this patient population. 31 This may take the form of medical infographics, or educational videos.16,17 Better tailored information may lead to a reduction of emotional distress, improved quality of life, and could help promote self-care strategies during and after chemoradiotherapy treatment. 32
Lack of Awareness and Understanding of Chemoradiotherapy-Induced Toxicities
Our interviews performed at T1 (prior to) and T2 (during chemoradiotherapy) highlighted a lack of awareness and understanding surrounding the reality of chemoradiotherapy-induced toxicities and a concern with the lack of personalized detail provided in information resources. A possible avenue to achieving better individualized resources could be through utilizing electronic reporting of patient-centred outcomes (PROs) to tailor consultations throughout the treatment period. Reporting treatment side effects using PROs in eg, cancer populations, has demonstrated impact on empowerment, understanding, and self-management.33–36 Patient-reported adverse effects can also be directly linked to medical records, enabling better incorporation into daily clinical practice.37–39 As glioblastoma patient needs evolve and recovery trajectories vary significantly between individuals, PRO monitoring may improve individual insight and provide a better platform for patient and caregiver education delivery.
Lack of awareness and understanding (theme 2) cannot be seen in isolation from theme 1: navigating information materials. Better tailored and more accessible information provision using eg, combined audio-visual and multimedia approaches, will minimize patient and caregiver lack of awareness for the potential induced toxicities they may encounter. 40 Indeed, a recent systematic review concluded that use of technology to support patient knowledge, can increase satisfaction, reduce anxiety, support treatment decision-making, and foster a stronger alliance between patients and their healthcare providers. 41
The Actual Experience and Impact of Chemoradiotherapy Toxicities
During the post-chemoradiotherapy interviews, patients and caregivers were able to reflect on their entire treatment trajectory to date. We found significant mismatches between information resources provided at the beginning of the pathway and patient and caregiver everyday experiences of chemoradiotherapy toxicities.
This mismatch poses a difficult equipoise around timing of education—patients and caregivers want more (tailored) information, but they also do not want to receive too much at one time, and the appropriate timing can vary. Participants called for a more manageable and tailored approach to information provision (see Figure 2). As proposed, this could be facilitated using electronic patient self-reporting platforms to tailor information. 42 These tools can be integrated with oncology information systems using machine learning to streamline data collection and allow greater comparison across the data.39,43 As digital health becomes more pertinent in healthcare, integrating these systems into clinical practice offers a promising avenue for making healthcare more responsive and patient-centred. 44

Recommendations to consider implementing into clinical practice.
Caregiver educational needs were also highlighted as a concern in this theme. Caregivers felt unprepared for treatment-induced toxicities and how to care for their loved one. A discrepancy between patients’ description of symptoms and caregivers’ concerns about patient symptoms caused concern and could complicate care provision. These findings are consistent with previous literature highlighting different information needs between brain tumor patients and caregivers,33,45 as well as a high level of distress, unmet needs, and lack of support available to caregivers.24,46 Caregiver needs are frequently considered secondary to those of the patient, 47 yet, in recent years caregivers are becoming more recognized partners in providing patient care. 48 In line with other research,24,25,46 our study confirms that caregivers lack the confidence and information to help them provide the best possible patient care at home. Providing caregivers with appropriate information and support is a crucial step to meeting both patient and caregiver needs as we move to more personalized, self-supported care in the UK's NHS. Separate psycho-educational resources for caregivers may be considered which may improve quality of care (Figure 2).
Limitations
While this study holds strengths in the repeat cross-sectional design, and in-depth qualitative exploration of both patient and caregiver views, it has its limitations. While repeat cross-sectional interviews helped us look across the treatment pathway, we have not followed the same patients and caregivers over time which may mask individual patient and caregiver changes in information needs over time. A true longitudinal investigation would have been preferable.
We have not captured HCP views which can create a more balanced view of the information delivery process. Their perspectives can also contextualize subtleties in managing patients’ and caregivers’ complex information needs as noted in previous studies. 49 In line with other investigations, 23 expanding on this concept and incorporating HCP knowledge of chemoradiotherapy toxicity severity could have significant impact towards the understanding of individual short- and long-term outcomes. HCPs are pivotal in providing this expertise and could improve a deeper understanding of how to tailor information and support.
Moreover, this was a single-center study, hence our findings may not reflect practice at other centers, which may utilize other information resources. Finally, it is important to recognize that findings stem from explanatory analyses, which elucidate relationships between “predictive variables” and outcomes within a patient group. This differs significantly from making individual predictions in clinical practice. 50 Despite this caveat, our patient and caregiver interviews show that their informational needs were not consistently met, providing recommendations for future practice (Figure 2), and emphasizing opportunities to generate larger, cross-center data sets.
Conclusions
In this qualitative exploration, we highlight that there is no “one size fits all” approach. Yet, participants articulated that the written information materials, supplemented with verbal explanation, did not adequately meet their information needs. These needs vary between individual patients and caregivers across the chemoradiotherapy pathway, presenting a difficult challenge to the HCPs supporting them. Combining patient experience data with HCP input to improve advice and support for treatment-induced toxicities is critical to ensuring patients and caregivers feel adequately prepared. With the drive towards precision medicine, we advocate that information provision and mediums of delivery should follow suit.
Despite our study's limitations, our findings related to written and verbal information provision can be applied and generalized, in some respect, to all cancer patients with varying diagnoses and their caregivers. However, certain aspects relating to difficulty with information processing due to cognitive decline demonstrate specific needs of glioblastoma patients. We hope our findings can guide better tailored support strategies and educational packages and appropriate timing of information delivery across centers supporting glioblastoma patients.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251331770 - Supplemental material for Glioblastoma Patient and Caregiver Perspectives of Treatment Side-Effects and Information Provision
Supplemental material, sj-docx-1-jpx-10.1177_23743735251331770 for Glioblastoma Patient and Caregiver Perspectives of Treatment Side-Effects and Information Provision by Sharon Fernandez, Susan C Short and Florien Boele in Journal of Patient Experience
Footnotes
Acknowledgements
We would like to thank the patients and caregivers who have participated in our interview project and for sharing their time and insights. We acknowledge the support of Cancer Research UK, Leeds Radiotherapy Research Centre of Excellence.
Author Contributions
SF, SCS, and FB did conceptualization; SF, SCS, and FB did methodology. SF did investigation. SF wrote the original draft. SF, SCS, and FB did review and editing.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics
We confirm that Ethical Committee approval was sought where necessary and is acknowledged within the text of the submitted manuscript.
Consent
We confirm that guidelines on patient consent have been met and any details of informed consent obtained are indicated within the text of the submitted manuscript.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.