
Abstract
As the What Matters To You (WMTY) movement spreads across the globe, countless clinicians have been inspired to ask their patients its eponymous question: what matters to you? Still, some clinicians remain apprehensive about asking what matters, worried that it can open a Pandora's box of problems too big for any one person to solve. This paper argues that embracing the spirit and skills of motivational interviewing (MI) can help and provides practical recommendations for navigating the synergistic uses of MI and WMTY.
Keywords
Introduction
It was more than a decade ago that Maureen Bisognano's keynote address at the Institute for Healthcare Improvement (IHI) Forum sparked a person-centered care movement. In it, the former IHI CEO challenged the healthcare community to shift from asking “What's the matter?” to asking, “What matters to you?”. 1
The What Matters to You (WMTY) movement has since spread like wildfire, being embraced by health and care providers in more than 50 countries. Each month, a core group of multinational volunteers hosts an open meeting where a growing network of over 300 global WMTY enthusiasts share their organization's implementation stories and experiences. In this forum, multiple intercontinental collaborations have been born, resulting in joint learning, resource development, and publications. The group has curated a WMTY website where robust international resources—including a WMTY implementation toolkit, videos, tools, case studies, and publications—are available to facilitate the movement's spread and guide the local implementation efforts of healthcare organizations and providers. Since June 2014, there has even been an annual international What Matters to You Day, with celebrations across the globe commemorating the movement's growing power and momentum.
What Matters To You empowers healthcare stakeholders to ask, listen, and do what matters. In its simplicity, WMTY shifts the power in any given situation to the person who knows best: patients, staff, or community members. In doing so, WMTY disrupts outdated and paternalistic models of care and collaboration, forging a better, person-centered future. 2
What Matters To You has now been applied in various clinical and community contexts with much success. Identified as one of five practices with potential to improve physician presence and enhance meaningful connection with patients, 3 WMTY has been shown time and again to be an effective strategy for elucidating patient and care giver priorities across a dynamic spectrum of care,4-10 engaging patients in their healthcare experiences, 11 and improving patient and caregiver outcomes and experiences.10,11 Likewise, WMTY can increase joy in work among clinicians and staff by addressing actionable sources of burnout that pervasively strain the healthcare system. Asking staff what matters to them is regarded as a core component of the IHI's Joy in Work framework, which implores health system leaders to identify and address actionable “pebbles” in staff members’ “shoes” using implementation science. 12 Moreover, asking, listening, and doing what matters for older adults is one of the “four M's” (what matters, medication, mentation, mobility) of the John Hartford Foundation's Age Friendly Care Systems model, aligning with the recently-approved Center for Medicare and Medicaid Services Age-Friendly Hospital measure. Looking ahead, researchers are now working to develop measures to evaluate the multidimensional effects of WMTY, in an effort to quantify its positive impacts on healthcare and inform innovative payment models.
As WMTY adherents ourselves, we have seen firsthand that the movement's benefits are not theoretical, but empiric. As clinicians and researchers, we ask patients and communities what matters and apply what we learn to guide health equity program development and research. Our health system, Montefiore Medical Center, has integrated WMTY within its novel community-based participatory research model designed to center community voices in health system decision-making, particularly as it pertains to health equity initiatives and research.13-16 Our research has, in turn, demonstrated that asking and listening to WMTY can build trust and power meaningful, bi-directional community engagement that results not only in person-centered thinking, but also person-centered solutioning.13-16
Yet, although many clinicians recognize the utility of WMTY, some may still be reluctant to ask the question, apprehensive that doing so will open a Pandora's box that they are ill-equipped to address. This feeling of overwhelm may be particularly poignant in healthcare settings where the constrains on providers’ time and resources—and, thus, the prevalence of burnout—is high.
For example, any given primary care provider may feel comfortable counseling a patient with poorly controlled diabetes about the importance of eating healthy. However, fewer may feel similarly equipped to address the underlying social determinants of health that a patient may be facing—burdens which can often only be uncovered by asking about what truly matters. Suddenly, the 30-second educational speech this physician might have otherwise given about the virtues of fresh produce and home-cooked meals would rightfully feel out of touch with their patient's reality.
This situation is not uncommon. In truth, we may all sometimes ask what matters, only to learn that there is little, if anything that we as individuals can do, given the constraints on our own time, resources, and power. What are clinicians to do then?
Actionable Insights
The spirit and skills of motivational interviewing (MI) can help. Like WMTY, MI is a person-centered, evidence-based, guiding communication style that helps move people toward behavior change. 17 Motivational interviewing is predicated upon an underlying “helping attitude” toward another person, “with four interlocking elements” that are foundational to its spirit: Compassion, Acceptance, Partnership and Evocation or Empowerment (CAPE). These MI spirit elements can be remembered using the acronym CAPE. Just like a superhero cape may instantly inspire a child wearing it to fly, so too may CAPE help patients feel empowered to make changes themselves.
What matters to you aligns with CAPE spirit elements. It is an inherently evocative and empowering question that cuts through the noise to unearth patients’ most pressing priorities. In doing so, it creates conditions for clinicians to respond empathetically, demonstrating their compassion and acceptance. Likewise, as clinicians move from asking and listening to doing what matters, they embody the spirit of partnership by addressing patient's needs whenever possible and acknowledging them when not.
Moreover, if the spirit of MI creates the nurturing conditions to move people toward change, the core skills of MI provide the mechanics to facilitate change conversations. These skills can be remembered by the widely-used acronym OARS: Open ended questions, Affirmations, Reflections, and Summaries. 17 An inherently open-ended question, WMTY can chart clinicians toward effective relationship building when asked from the heart. Then, as WMTY conversations unfold, the dovetailing strategies of affirmations and reflections can help ensure that patients feel seen, heard, and understood. In this way, employing motivational skills when asking WMTY prepares clinicians to meet their patients where they are.
Practical Recommendations
Affirmations and reflective listening statements, in particular, can help clinicians navigate conversations around complex biopsychosocial stressors and initiate dialogues about how to address them. Recalling the previous example of someone with poorly controlled diabetes experiencing food insecurity, a clinician who may instinctively feel overwhelmed by the prospect of solving a patient's food insecurity need only remember that listening itself can be the first step to doing what matters. Consider the following vignette: Marie Halpern is a 50-year-old-woman with poorly controlled diabetes. During her last visit, you increased her medications and provided nutritional counseling. Today, her HbA1c remains high and you suspect medication non-adherence. You decide to start the visit by asking Ms. Halpern what matters.
“It's great to see you, Ms. Halpern. Tell me, what matters most to you today?”
Already, Ms. Halpern has the floor to discuss what is truly important to her, without judgement. Note that clinicians do not need to use these exact words of WMTY. The “what matters” question can be phrased in a variety of ways as long as it leaves room for the patient to freely express their own priorities; for example, “What is most important to you today? or “What are your goals and how can I help you achieve them?”. Getting back to the dialogue, Ms. Halpern may respond: “Well, doctor, I’ve been taking my medications every day, but I just can't seem to eat healthier. There is just too much on my plate.” There are two possible MI skills that a clinician can naturally incorporate into their response. The first is the use of an affirmation and the second is the use of a reflective listening statement. Affirmations aim to convey acceptance and compassion for the patient while acknowledging their inner strengths. In contrast to praise, affirmations begin with “you” rather than “I” to keep the focus on the patient, rather than centering the clinician. An appropriate MI-adherent affirmation might be: “You have insight into the importance of eating healthy.” In just a few words, this effectively affirms the patient's understanding of their condition and commitment to improving their disease control, conveying that the clinician sees the patient. This crucial step enables further evocation and partnership. Empowered, the patient may continue to share: “I do. I know that eating right is important, but with everything going on at work and at home, it feels too difficult most days.” At this point, the clinician can use reflective listening for clarification, bringing to light what the patient may be thinking or feeling under the surface. For example, an MI-adherent reflective listening statement might endeavor to unearth a challenge: “It sounds like you are really struggling with work-life balance.” Another might reflect an emotion: “You have been really stressed lately.” In either case, the provider aims to name the elephant in the room in order to deepen their understanding of the patient's situation and priorities. It is crucial to note that effective reflective listening incorporates both the spirit (CAPE) and skills (OARS) of MI. The spirit of MI creates a safe space, such that if a reflective listening statement is off-base, the patient feels comfortable clarifying what they are really struggling with. For example, the patient might respond by saying, “Actually doctor, balance is not really the issue. It is just that finances are really tight right now and I’m struggling to put any food on the table for my kids, let alone healthy food.” If they had they never asked what matters, the clinician may have erroneously labeled this patient as “non-adherent” or “difficult.” Instead, equipped with this new knowledge, the clinician is now poised to come alongside the patient as a solutioning partner. If the clinician worked in a health system such as ours, where we are prioritizing upstream strategies to address social determinants of health needs, they could connect Ms. Halpern to a community health worker to navigate her to a social service program or a local food pantry.
18
However, even if the clinician doesn't have the capacity to bridge a patient to needed social services, a reflective listening statement such as “You have a lot going on right now. I can understand why prioritizing a healthy diet is just not realistic right now” can help meet the patient where they are. This response demonstrates compassion and understanding, and is, in itself, “doing” what matters. An additional, annotated vignette included in Appendix 1 provides another example that illustrates how blending WMTY and MI can guide the compassionate development of person-centered solutions.
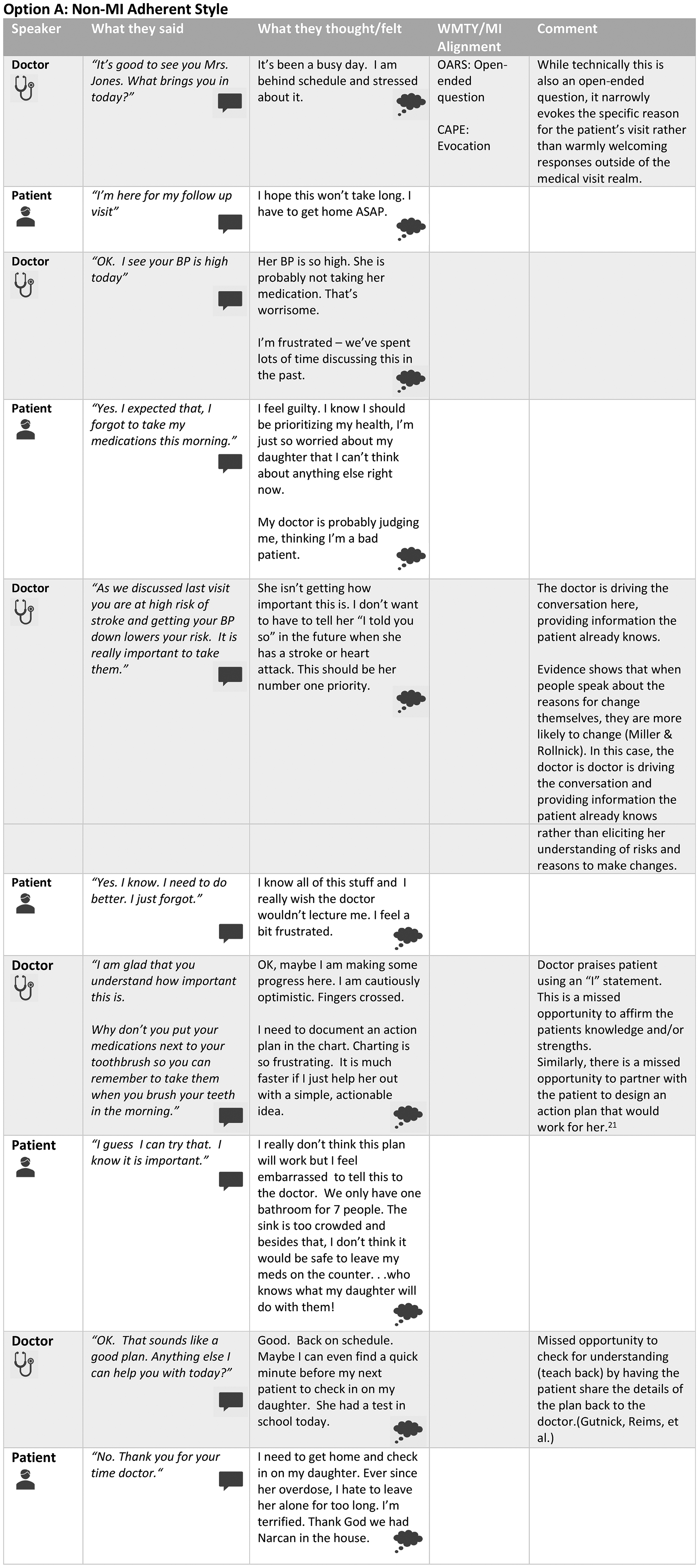
Clinical vignettes illustrating motivational interviewing (MI)-adherent versus non-MI adherent interviews of a single patient. Clinical vignette: Susan Jones is a 50-year-old woman with poorly controlled hypertension. Her blood pressure today is 150/90. You suspect nonadherence with her medications
The synergies between MI and WMTY are increasingly being explored in the literature. For example, a new MI-based model developed by a group of MI trainers including co-author Dr Gutnick, is leveraging WMTY to help move vaccine-hesitant patients toward vaccine motivation. After establishing rapport, the model recommends “understanding what matters to patients: their concerns, beliefs, and fears about the vaccine,” positing that the synergistic use of WMTY and MI can foster trust, create conditions for patients to discuss their reservations openly and honestly, and ultimately unearth addressable drivers of health inequity. 19
Conclusion
As the WMTY movement continues to spread around the world, healthcare organizations and providers would benefit from recognizing the movement's alignment with MI. Healthcare organizations should uplift the practice of MI among WMTY-engaged personnel, offering MI skill-building trainings to those who need or want it. Likewise, healthcare providers should feel confident that the spirit and skills of MI can help them navigate any Pandora's box that WMTY may open. After all, asking and listening with compassion and acceptance are always the necessary first steps in doing what matters.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251317041 - Supplemental material for Motivational Interviewing is “Doing” What Matters: Integrating Motivational Interviewing Spirit and Skills into What Matters to You? Conversations
Supplemental material, sj-docx-1-jpx-10.1177_23743735251317041 for Motivational Interviewing is “Doing” What Matters: Integrating Motivational Interviewing Spirit and Skills into What Matters to You? Conversations by Damara Gutnick and Sarah McNeilly in Journal of Patient Experience
Footnotes
Acknowledgments
The authors acknowledge the What Matters to You Movement, and Maureen Bisognano in particular.
Authors Contribution
DG conceptualized the paper. DG and SM contributed equally to drafting and editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.