
Abstract
Among 203 patients presenting for musculoskeletal specialty care between November 2023 and January 2024, we measured the relationship of openness to mindset exercises such as cognitive behavioral therapy (training the mind to default to healthier thoughts and feelings about bodily sensations) with levels of personal health agency accounting for other personal factors. Factors associated with greater openness to mindset exercises in linear regression included greater personal health agency (RC = 0.17), younger age (RC = −0.030), and 4-year college education (RC = 1.5). In a second linear regression, greater personal health agency was associated with older age (RC = 0.053), greater trust in the clinician (RC = 0.25), injury diagnosis (RC = 1.8), less distress regarding symptoms (RC = −0.25), less unhelpful thinking regarding symptoms (RC = −0.43), and retirement (RC = −1.7). In cluster analysis, we found that increasingly lower openness to mindset exercises was associated with increasingly worse levels of distress and unhelpful thoughts, lower personal health agency, and slightly varying social health and trust in clinician. The finding that greater responsibility for one's health, including openness to mindset exercises, corresponds with a healthy understanding and emotional response to bodily sensations, greater social security, and greater trust in the clinician directs specialists to prioritize building trust, gently reorienting common misconceptions about bodily sensations, and assistance with social stressors.
Keywords
Introduction
Background
Personal health agency is the degree to which a person regards health as an active process for which they are responsible and able to engage in. 1 Higher levels of personal health agency are associated with better adherence to treatment, higher likelihood of engaging in healthy behaviors, more positive healthcare experiences, and lower healthcare costs and utilization.2–5 A recent systematic review found weak-to-moderate associations between levels of personal health agency and mental health, social health, comfort, and capability among people seeking musculoskeletal specialty care. 6 However, those studies used agency measures that were developed in the context of conditions where treatments are disease-modifying (eg, diabetes, chronic heart disease), such as the Patient Activation Measure (PAM). 1 In those contexts, the concept of personal health agency is focused on themes such as treatment adherence, building healthy habits, and ability to seek care when appropriate. Musculoskeletal specialty care is often optional (discretionary) and sensitive to patient preferences. Personal musculoskeletal health agency might therefore be represented less by adherence to recommendations and more by confidence managing one's health independently. This is underlined by qualitative evidence reporting that patient perceptions of health agency covered a wide range of behaviors, skills, and beliefs that were not always captured by the PAM such as dealing with fluctuations in symptom intensity or collaboration with the clinician. 7 A recent factor analysis of items derived from legacy personal health agency measures determined a small number of items that are representative and potentially able to quantify health agency more accurately among patients seeking discretionary care (Agency for Navigating Challenges, Health Ownership, and Resilience [ANCHOR] measure; submitted).
Rationale
It is now well-established that variations in mental health (thoughts and feelings about bodily sensations such as feelings of worry or despair, and unhelpful thinking such as catastrophic thinking about pain or fear of painful movement) have notable associations with comfort and capability among patients seeking musculoskeletal specialty care.3–18 Qualitative research has demonstrated a relationship between patient involvement in decision making and willingness to engage with mental health services. 19 This suggests that a sense of ownership and responsibility for one's health may correspond with an openness to working toward a healthy understanding and emotional response to the body's sensations. Tactics for developing a healthier regard for bodily sensations often consist of specific exercises that help train the mind to default to healthier thoughts and emotions (mindset exercises). 20 Mindset exercises are generally organized around cognitive behavioral therapy principles 20 and have the potential to reduce levels of discomfort associated with musculoskeletal conditions.21–24 A better understanding of the factors associated with patient receptiveness to cultivating a healthier inner narrative regarding one's body and its sensations (mindset exercises) could aid the development, implementation, and adoption of comprehensive care strategies. If greater openness to mindset exercises is associated with greater health agency addressed in the context of musculoskeletal specialty care, then supporting an active approach toward one's health may become an integral part of comprehensive, whole person health strategies.
Questions
In a cross-sectional study of people seeking musculoskeletal specialty care, accounting for potential confounders, we asked: (a) Is there a relationship between openness to mindset exercises and the level of personal health agency among people seeking musculoskeletal specialty care? (b) What factors are associated with personal health agency?
Methods
Study Design and Setting
In this cross-sectional study, approved by our Institutional Review Board, all new and returning people seeking care for any musculoskeletal symptoms in 1 of the local musculoskeletal specialty care units in an urban area in the United States between November 2023 and January 2024 were invited to participate by an independent researcher (medical student researchers). Patients were deemed eligible when they were English or Spanish speaking and between 18 and 89 years old. Exclusion criteria included cognitive or other impairment precluding survey completion on a tablet. Participants provided verbal informed consent for data collection using Health Insurance and Portability Accounting Act compliant software (Research Electronic Data Capture [REDCap], Vanderbilt, TN and cloud-based file storage. All collected data were patient-reported. We did not record identifiable patient information.
Participants
We identified 211 eligible patients who agreed to participate, of which 96% (203 of 211) completed the primary outcome measure and were included in subsequent analyses. Most participants self-identified as white (60%), English speaking (90%), married or partnered (58%), employed (56%), had a 4-years college degree (34%) or graduate degree (28%), private insurance (46%), and were seeking care for an upper extremity problem (60%) (Table 1). There was an equal distribution of men (50%) and women (50%).
Demographics of Cohort.

SD, standard deviation; IQR, interquartile range.
Outcome Measure
The primary outcome was openness to mindset exercises and was measured using a patient-reported 11-point rating scale (0-10). Higher scores indicate greater receptiveness or willingness of patients to participate in mindset exercises. The secondary outcome was personal health agency and was measured using the 6-item Agency for Navigating Challenges, Health Ownership, and Resilience (ANCHOR) measure (submitted), in which statements were rated by patients on a scale from 0 (strongly disagree) to 4 (strongly agree). The answers to each item were then summed to generate a total score ranging from 0 to 24, with higher scores indicating greater personal health agency (more ownership and active approach toward one's health). The measure is internally validated in a prior study with excellent psychometric properties (root mean square error of approximation [RMSEA] = 0.033 and Cronbach alpha = .90).
Explanatory Variables
We measured demographics (gender, age, race, level of education, annual household income, marital status, and primary language), clinical information (traumatic pathophysiology or not), mental health, social health, and trust in clinician. Mental health was measured using 3-items that measure of feelings of distress (worry [anxiety] and despair [depression]) regarding musculoskeletal symptoms 25 and 3 items that measure unhelpful thoughts regarding musculoskeletal symptoms identified in a factor analysis of common measures of thoughts and feelings regarding painful sensations such as the Pain Catastrophizing Scale and Tampa Scale of Kinesiophobia. 25 Both 3-item measures displayed good psychometric properties in a prior study with standardized root mean square residual of 0.049 and 0.038 and Cronbach alpha of .95 and .90, respectively. 25 Higher scores indicate higher levels of distress and unhelpful thoughts regarding bodily sensations. Social health was measured using a new 9-item measure of quantified social health (Social Health Scale; SHS), 26 in which patients answered statements about their financial security and social support on a 5-point Likert scale resulting in a total score between 0 and 36 with higher scores indicating more disadvantaged social health. SHS displayed good psychometric properties in a prior study with RMSEA of 0.046 and Cronbach alpha ranging between .80 and .84 for each subdomain (financial security and social support). 26 Trust in the clinician was measured using the validated 7-item Trust and Experience with Clinician Scale (TRECS-7). 27 Higher scores indicate more trust and better experience with the clinician. TRECS-7 displayed excellent psychometric properties in a prior study with RMSEA of <0.001 and Cronbach alpha of .91. 27
Statistical Analysis
We performed descriptive statistics for all variables. We reported categorical variables as percentage (number), and continuous variables as mean (standard deviation) or median (interquartile range) depending on data distribution (normal and nonnormal, respectively).
Multivariable linear regression models were constructed to seek factors associated with (a) openness to mindset exercises and (b) personal health agency, using a forward variable selection method in which explanatory variables with the highest proportion of shared variance relative to the outcome (high semipartial R 2 ) were included using a stepwise approach until the model fit no longer improved (lower Akaike Information Criterion). Considering the relatively nonnormal distribution of openness to mindset exercises, we ran both multivariable linear regression as well as negative binomial regression models and chose the model with the best fit (multivariable linear regression). A forward selection method was used due to an increased risk for multicollinearity (intercorrelation) among various explanatory variables as determined by a spearman rank correlation matrix with personal health agency, feelings of distress regarding symptoms, unhelpful thoughts regarding symptoms, social health, and trust in clinician (Appendix 1). Multicollinearity is a phenomenon in which explanatory variables are intercorrelated to the extent that it can negatively affect parameter estimations and reproducibility of multivariable regression models. 28 Therefore, we opted to only include variables that were most relevant to the assessed outcome in order to reduce the risk of biased parameter estimates. As another, unplanned, statistical analysis intended to address the known collinearity of subjective personal health variables, 28 we performed a cluster analysis to identify groups of patients with comparable levels of (a) health agency, (b) feelings of distress, (c) unhelpful thoughts, (d) social health, and (e) trust in clinician. This approach allowed us to assess the mean differences in openness to mindset exercises between various statistical groupings (clusters) of patients with comparable characteristics (similar levels of the 5 variables above), essentially eliminating multicollinearity while still being able to take all intercorrelated variables into account. We used a k-means clustering algorithm and allowed for up to 20 clusters (statistical groupings of patients with comparable characteristics) to form. We then generated scree plots to determine the optimal number of clusters to retain using Yuan's “elbow” method, 29 which aims to minimize both the prediction error and the number of unique clusters. The cluster solution was then translated into a new variable representing the statistical groupings. We subsequently used a one-way ANOVA test to assess the mean differences in openness to mindset exercises between the identified statistical groupings. Descriptive statistics were also performed to describe the characteristics of the generated subgroups. All P-values below .05 were considered statistically significant.
An a priori sample size calculation determined that 201 observations would provide 80% statistical power to detect a small-to-medium effect size (Cohen's f2 = 0.10) in a multivariable linear regression model with 15 explanatory variables that explains as little as 9% of the variation in an outcome variable with an alpha set at 0.05.
Results
Factors Associated With Openness to Mindset Exercises
Accounting for potential confounders such as age, level of education and social health, we found that a greater openness to mindset exercises was associated moderately with greater health agency (regression coefficient [RC] = 0.17, P = .007), slightly with younger age (RC = −0.030, P = .025), and moderately with having a 4-year college degree (RC = 1.5, P = .017) (Table 2). The model accounted for 11% of the observed variation in openness to mindset exercises. Using cluster analysis, we identified 6 distinct subgroups of patients with increasingly worse levels of distress, unhelpful thinking, and health agency, and somewhat varying levels of social health and trust in clinician, that were generally associated with increasingly lower openness to mindset exercises (Table 3). Notably, higher trust in the clinician seemed to be associated with greater openness to mindset exercises, more so even than greater agency, except when higher trust in the clinician was accompanied by social health concerns and higher levels of unhelpful thinking.
Multivariable Linear Regression of Factors Associated With Openness to Mindset Exercises.
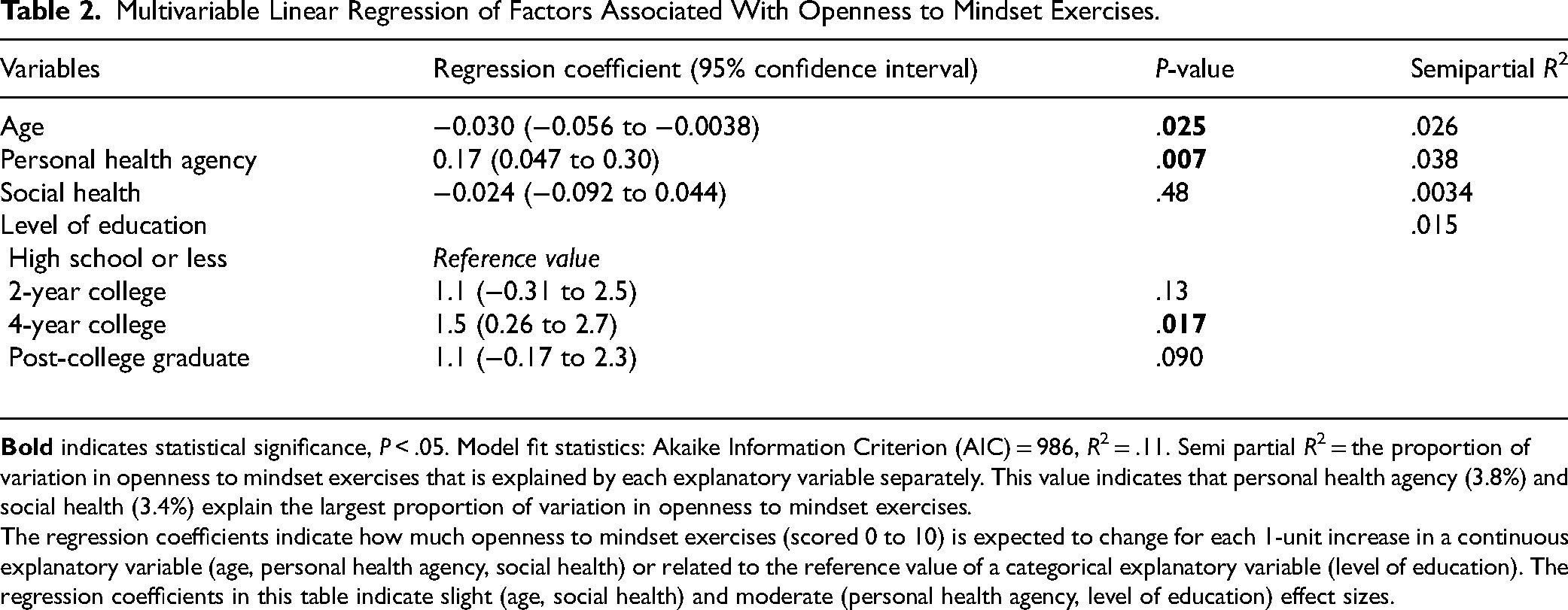
The regression coefficients indicate how much openness to mindset exercises (scored 0 to 10) is expected to change for each 1-unit increase in a continuous explanatory variable (age, personal health agency, social health) or related to the reference value of a categorical explanatory variable (level of education). The regression coefficients in this table indicate slight (age, social health) and moderate (personal health agency, level of education) effect sizes.
Descriptive Statistics of the Subgroups Identified in Cluster Analysis, Including the Mean Differences in Openness to Mindset Exercises.

*P = .034. Z scores indicate the number of standard deviations the group is separated from the mean of the cohort. Green colors indicate more favorable scores (lower levels of distress/unhelpful thoughts/social disadvantage and higher levels of trust/personal health agency), the gray color indicates a relatively neutral score, and red colors indicate less favorable scores (higher levels of distress/unhelpful thoughts/social disadvantage and lower levels of trust/personal health agency).
Factors Associated With Health Agency
Accounting for potential confounders such as age, employment status, and social health, we found that greater health agency was associated slightly with older age (RC = 0.053, P = .001), moderately with more trust in the clinician (RC = 0.25, P < .001), and moderately traumatic pathophysiology compared to degenerative pathophysiology (RC = 1.8, P < .001) (Table 4). Lower levels of health agency were associated moderately with higher levels of distress (RC = −0.25, P = .004), moderately with higher levels of unhelpful thinking (RC = −0.43, P < .001), and moderately with being retired compared to being employed (RC = −1.7, P = .006). The model accounted for 50% of the observed variation in personal health agency.
Multivariable Linear Regression of Factors Associated With Personal Health Agency.

The regression coefficients indicate how much personal health agency (scored 0 to 24) is expected to change for each 1-unit increase in a continuous explanatory variable (age, distress, unhelpful thinking, trust, social health) or related to the reference value of a categorical explanatory variable (trauma, employment). The regression coefficients in this table indicate slight (age) and moderate (distress, unhelpful thinking, trust, trauma, retired) effect sizes.
Discussion
Background, Rationale, and Findings
A better understanding of the factors associated with patient openness to mindset exercises and personal health agency could aid the development of comprehensive care strategies as well as strategies to improve patient engagement. In this cross-sectional study of people seeking musculoskeletal specialty care, we found that greater openness to mindset exercises was associated with greater personal health agency, younger age, and having a 4-year college degree. We also identified 6 clusters that demonstrated that personal subjective aspects of human illness tend to decrease in sync, and that less healthy mindsets were associated with less openness to mindset exercises even when balanced by greater trust in the clinician. Additionally, we found that lower levels of personal health agency were associated with younger age, lower trust in the clinician, nontraumatic pathophysiology, higher levels of distress and unhelpful thinking regarding symptoms, and being retired.
Limitations
This study must be viewed in the light of several limitations. First, we used cluster analysis to manage collinearity by categorizing subjective measures that occur on a continuum (for instance, feelings of distress or unhelpful thoughts regarding symptoms). Although categorizing subjective measures has the potential to reinforce various forms of stigma by pointing out different classes of people, this approach allowed us to manage collinearity that would otherwise result in underrepresentation of important aspects of human illness behavior. We urge the reader to notice the flow of the statistical groupings where subjective measures seem to travel in tandem, representing the continuum of subjective measures, rather than the individual categories. Second, there are some remaining ceiling effects in the TRECS measure (8.2%; while TRECS is already 1 of the patient-reported experience measures with the lowest reported ceiling effect 27 ), and this may reflect that some people may not answer the questions forthrightly due to social desirability and other factors. For instance, 8 patients (group 5) had high levels of trust and low scores on mental health, social health, and health agency. It seems more likely that these ratings were not forthright as opposed to patients having a perfect experience with their clinician (as reflected by the highest possible TRECS score—given the evidence that patient-reported experience measures addressing varied aspects such as perceived empathy, communication effectiveness, satisfaction with care, and trust in the clinician are correlated 30 ). In general, the clusters suggest that higher levels of trust seem associated with healthier mindset and greater health agency. High ceiling effects are common among patient-reported experience measures and attempts to reduce ceiling effects using different rating systems,31,32 item response theory to select only the items with lowest ceiling effects (TRECS), 27 and accounting for social desirability 33 had limited effect. It could be that ceiling effects are an integral part—and problem—of patient-reported experience measures that cannot be fully remedied. Future studies may elaborate on the role of natural language processing to tackle ceiling effects. 34 Third, given that the regression model accounts for only 11% of the variation in receptiveness to mindset exercises, it is possible that there are other, potentially unmeasurable, factors associated with the remaining variation in receptiveness to mindset exercises. Alternatively, it may be that that the concept of “openness to mindset exercises” is complex and difficult to model statistically. Fourth, there is evidence that people do not answer questions about mental health forthrightly considering the notable floor effects (proportion of patients with lowest possible score) and hasty completion,35–37 perhaps due to mental health stigma. On the other hand, these floor effects have not hindered identifications of associations in this and prior studies. Fifth, these findings may best apply to patients in our setting. However, it seems likely that the association would be reproducible in other settings, considering we are measuring basic human traits and behaviors. Sixth, this study sought to address patient receptiveness to mindset exercises rather than the effectiveness of mindset exercises or education related to personal health agency. Future studies may elaborate on the effects of mindset exercises on levels of distress and unhelpful thoughts, personal health agency, and comfort and capability. Such studies may also explore the degree to which personal factors such as trust in the clinician and personal health agency may influence the effectiveness of mindset exercises. Last, we did not study the patient's prior experiences or attitude toward physical therapy although this could be interesting given that many physiotherapists contend that mindset exercises are a part of their treatment.38,39 There are various studies that reported considerable benefits to incorporating mindset exercises in physiotherapy to improve levels of comfort and capability.40–42 Future studies may elaborate on the effects that patient attitude toward physical therapy may have on the receptiveness to and effectiveness of mindset exercises.
Factors Associated With Openness to Mindset Exercises
The observation that greater openness to mindset exercises was moderately associated with greater personal health agency has face validity as both constructs reflect an active approach toward one's health. However, the effect size seems somewhat limited considering that personal health agency only accounted for 3.8% of the variation in openness to mindset exercises. Yet, it may still reflect that an integral part of ownership and responsibility for one's health (greater personal health agency) may be a determination to nurture the healthiest possible understanding and emotional response to one's bodily sensations. This is in line with qualitative evidence among 15 patients with brachial plexus injury that found that those who felt more engaged in decision-making were more open to mental health services. 19 There also is evidence among other specialties that greater personal health agency is associated with healthier behaviors and adaptive coping strategies.43–47 One qualitative study among 27 people with varying chronic conditions such as hypercholesterolemia, back pain, and arthritis found that people with higher levels of personal health agency regarded successful self-management as taking control (eg, actively seeking advice and information, engaging in discussions with care providers and challenging them) whereas those with lower levels of personal health agency regarded successful self-management more as compliance (eg, following doctor's advice or instructions). 47 Interestingly, those with higher levels of personal health agency were able to report more (detailed) coping strategies that helped them to manage stress, which was regarded as an important barrier to self-management. 47 It is notable that the clusters with higher levels of distress and unhelpful thinking regarding symptoms were generally associated with lower openness to mindset exercises. Patients who could benefit most from mindset exercises seem to be the least receptive, independent of their trust in the clinician. This is in line with evidence that less than half of those with notable symptoms of anxiety or depression seek care for their mental health,48–52 which may be, in part, due to lower levels of mental health literacy (ability to recognize, understand, and manage mental health problems)53,54; a construct that is also linked to (more severe) symptoms of anxiety and depression.53–55 Interestingly, trust in the clinician seemed to be associated with greater openness to mindset exercises except in the small subset of 8 patients in whom high levels of trust were paired with worse social health and higher levels of unhelpful thinking. There may be people that report high trust in the clinician but don’t experience it, which could explain the remaining ceiling effect in TRECS (8.2%) and other patient-reported experience measures.27,30,31,33 It might also be an example of high hopes for the surgeon to provide a quick fix solution to one's symptoms without the willingness to undertake—or understanding of the importance of—active participation in healthy behaviors that may take longer to show benefits. This attitude may also explain the poor adherence to exercises at the physical therapist with rates as low as 30%.56,57
The observation that younger age is slightly associated with greater openness to mindset exercises may point to a more open attitude toward talking about mental health among younger people, although the effect seems limited. The decreasing trend of mental health stigma (between 2006 and 2018) relatively independent of sociodemographic characteristics (indicating a broad shift) may substantiate this hypothesis. 58 Interestingly, older age was associated with greater mental health stigma while generations born 1987 to 2000 (and 1937-1946) were more likely to report a more open attitude toward mental health. There also is evidence that younger generations have a greater ability to distinguish normal thoughts and feelings from symptoms of depression or anxiety (mental health literacy)59,60 which may also influence their openness to mindset exercises.
Factors Associated With Health Agency
The observation that lower personal health agency was moderately associated with higher levels of distress and unhelpful thinking, although the proportion of variation explained by these mindset factors is somewhat limited (2.5% and 4.4%, respectively), suggests a potential association between unhelpful interpretation of sensations and passivity regarding one's health, which is in line with available evidence.45,46,61–63 Both unhelpful thinking and low health agency may be mediated by relatively high levels of cognitive fusion (regarding thoughts as facts; inflexible thinking), rumination, and experiential avoidance (general unwillingness to experience undesired sensations, thoughts, and feelings)—factors hypothesized as a foundation of vulnerability to distress. 64 Experiential avoidance—arguably the opposite of agency—may lead to less exposure to experiences that can help reorient unwanted thoughts and feelings. While experiential avoidance may reduce feelings of distress initially, it is associated with higher levels of distress over time.65–69 Regular physical activity, which has the potential to reorient experiential avoidance, can lead to lower levels of distress. 70 Surgeons may therefore decide to encourage people with greater feelings of distress or unhelpful thoughts regarding symptoms to participate in regular physical activity. It may also be helpful to elaborate on the patient's attitude and prior experiences related to exercises so that they can address patient perceived barriers to participate in regular physical activity (eg, fear or movement or misconceptions about pain indicating damage to the body).
The observation that greater personal health agency was moderately associated with greater trust in the clinician is interesting as one might plausibly expect the opposite. Namely, that patients with a higher level of trust in their clinician might have a greater tendency to pass responsibility for health to those clinicians (lower agency). However, it may be that greater trust in oneself (agency) and greater trust in others (trust in clinician) are related constructs both founded in effective self-management of cognitive heuristics and cognitive bias (healthier mindset; lower levels of distress or unhelpful thoughts). The finding that trust in the clinician explained the largest proportion of variation in personal health agency (7.5%), reiterates the importance of building a trusting patient-clinician relationship. 71 This is in line with available evidence emphasizing the strong bidirectional correlation between trust in the clinician and personal health agency.72,73 Interestingly, patients of primary care physicians who were more supportive of the patient's role in their self-management reported higher levels of personal health agency. 74 Future studies may elaborate on whether attempts to improve the patient-clinician relationship have potential to increase the patient's level of personal health agency. Such studies may also elaborate on whether the clinician's level of trust in the patient is associated with the patient's level of personal health agency and trust in the clinician.
The observation that traumatic pathophysiology was moderately associated with a higher level of personal health agency seems aligned with evidence that seeking care for degenerative and idiopathic conditions is often associated with a less healthy mindset (eg, higher levels of distress or unhelpful thoughts regarding symptoms),8,75 and may point to lower personal health agency as part of the less healthy mindset that might lead to greater care seeking. The trauma population might also be relatively more active (prior to injury) and potentially more motivated to recover due to the perception of being able to get back to similar levels of comfort and capability as prior to injury. These findings may indicate that people seeking care for degenerative and idiopathic conditions can benefit most from interventions focused on increasing the ability and confidence to manage one's own health.
Practical Application of the Findings
The findings of this study that openness to mindset exercises correlates with personal health agency, healthier thoughts and emotions, and more supportive circumstances direct us to be attuned for signs of passivity (“they will solve it”), magical thinking (“I don’t care how it works”), vulnerability, protectiveness, social disadvantage, worry and despair. These interrelationships suggest that care strategies designed to guide people toward an active role in their health may help address the personal and subjective aspects of health collectively. 74 To help illustrate these points, consider the specific example of rotator cuff tendinopathy, age-related changes in the shoulder tendons that most of us will develop within our lifetime.76–78 When strategizing management, rather than passive administration of a corticosteroid injection (slight, transient benefit over placebo injection 79 ) or prescription of exercises done at the office of a physical therapist (no better than independent exercises 80 ), we might educate people and encourage them to seek over-the-counter analgesics and make a habit of home exercises. An approach that fosters greater agency for one's health might also increase openness to cultivating the healthiest possible understanding of bodily sensations: “It is difficult getting old, but I can manage.” Alternatively, allowing people to remain the passive receiver of injections and “physical therapy” may reinforce an unhealthy dependency founded in less healthy mindsets that remain underappreciated and under addressed. A strategy that does not anticipate commonplace patient regard of health as passive and inscrutable, and is not prepared to creatively and intentionally reorient people toward an active, independent role in matter-of-fact approaches to their health, has the potential to limit people's accommodation of their aging body and their specific musculoskeletal condition. There are some published experiments of attempts to improve personal health agency,2,22,81 but more work is needed. One study randomized people in ongoing care for daily musculoskeletal pain to either receive an intervention consisting of four 90-min group sessions with a psychologist to encourage active engagement in health or to receive usual care, and found lower levels of depressive symptoms, greater overall health, and greater adherence to exercises in the intervention group, but no change in personal health agency (measured with PAM-13) at 12 months. 22 Another randomized controlled trial among 121 people with self-reported daily pain randomized patients to receive a group-based self-management course in cognitive and behavioral therapy with weekly 2.5-h sessions for 6 weeks or to receive a weekly low-impact group outdoor physical activity and found improvements in pain intensity and global health in both groups, but no differences between the groups in health agency (measured with PAM-13), pain intensity, symptoms of anxiety, symptoms of depression, and general health at 12 months. 81
Effective strategies should also anticipate common misconceptions and misinterpretations of the body's sensations (unhelpful thoughts) and feelings of distress regarding sensations. Specialists can consider using the brief 3-item measures intended to feel more relevant to patient used in this study 25 to screen for these factors while limiting patient burden. More importantly, specialists can be attuned for verbal and nonverbal signs of less healthy mindsets such as holding a body part protectively, withdrawing, grimacing, and involuntarily hindering movement (eg flexing the wrist while trying to make a fist).82,83 Important barriers for musculoskeletal surgeons to discuss mental health (and openness to mindset exercises) include a perceived lack of mental health resources, time pressure, lack of expertise or comfort in discussing mental health, and uncertainty about the appropriateness to discuss mental health. 84 However, most people seeking care for musculoskeletal symptoms actually want their mental health to be acknowledged, if not addressed, as part of their care plan. 84 Therefore, the most important strategy for specialists is to prioritize their relationship with the patient. To paraphrase the common saying, patients want to know you care before they’ll take interest in what you know. Trust is built through curiosity, genuine interest, admiration, and collaboration. 71 With trust it is safe to talk about stress, distress, and healthier ways to think about sensations. There is evidence that discussion of mental health is not associated with diminished patient experience. 85 Opening a discussion about the screening measures a patient completed prior to a visit can help make it comfortable to address mental health. 84 In such situations, surgeons may try to avoid stigmatizing (categorizing/othering) thoughts and language (ie, “catastrophizer,” “supratentorial”) and instead ascribe to neutral concepts and wording such as “the mind and the body work together,” “pain is part physical and part emotional” and other phrases tested for resonance with patients. 84 Care strategies focused on alleviating feelings of distress and unhelpful thoughts regarding symptoms have the potential to improve various aspects of health including personal health agency 63 and levels of comfort and capability.21–24
Conclusion
In this cross-sectional study of people seeking musculoskeletal specialty care, we found that greater openness to mindset exercises was associated with greater health agency, younger age, and having a 4-year college degree. These findings reflect that ownership and responsibility for one's health can help people work toward a healthy understanding and emotional response to their body's sensations. We also found that greater health agency was associated with older age, higher trust in the clinician, traumatic pathophysiology, lower levels of distress and unhelpful thinking, and not being retired. Notably, patients who could benefit most from mindset exercises (those with higher levels of distress and unhelpful thinking) seem to be the least receptive. These findings emphasize the potential benefits of a guiding rather than a directing approach in healthcare. Future studies can elaborate on whether musculoskeletal care strategies that emphasize guidance of patients toward greater agency, self-awareness, and self-management lead to better mental and physical health.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251376078 - Supplemental material for Greater Personal Health Agency Is Associated With Greater Patient Receptiveness to Mindset Exercises
Supplemental material, sj-docx-1-jpx-10.1177_23743735251376078 for Greater Personal Health Agency Is Associated With Greater Patient Receptiveness to Mindset Exercises by Niels Brinkman, Rebecca Ludden, Ali Azarpey, Job N. Doornberg, David Ring and Prakash Jayakumar in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved and waived for further review by our Institutional Review Board. Participants provided verbal informed consent for data collection.
Funding
This work was performed at the University of Texas at Austin, Austin, Texas, USA. We received no funding for the submitted work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.