
Abstract
During the COVID-19 pandemic, most cancer centers shifted from in-person to virtual cancer care to curb community spread and ensure care continuity. This qualitative descriptive study aimed to understand cancer patient-perceived risks related to COVID-19 and cancer treatment, as well as the patient-perceived and experienced value of virtual care. From June to August 2020, focus groups were conducted with patients under active management or observation for a diagnosed malignancy in Toronto, Canada. A thematic analysis of six focus groups found that most participants worried more about treatment delays than they did about COVID-19 infection. Despite some concern about COVID-19 exposure in the hospital, care delays contributed to increased anxiety among participants who already subscribed to strict safety measures in their everyday lives. Most participants accepted virtual care for some appointment types; however, preference for in-person care was found to sustain the humanistic and therapeutic aspects of cancer care that many participants valued. Nuances in the appropriateness and adequacy of virtual cancer care still need exploration. Preserving the humanistic aspects of care is of paramount importance.
Introduction
Cancer care entered uncharted territory when the novel coronavirus (COVID-19) rapidly spread in early 2020. Patients undergoing active cancer treatment, such as radiation and/or chemotherapy, were quickly identified as a group potentially vulnerable to the disease, especially those with additional risk factors such as older age, therapy-related immunosuppression, and other co-morbidities (1–3). For many cancer patients, treatment must be delivered in-person in cancer centers that are often in larger hospitals. For most, delaying or interrupting their care until after the COVID-19 crisis could lead to under-managed disease and worse outcomes (4). Yet, some patients feared exposure to COVID-19 in hospitals and were confused about symptoms and infection risk (5,6); some also experienced significant anxiety and reluctance to proceed with treatment (7,8). The extent to which cancer patients experienced the tension between potential exposure to COVID-19 and undergoing cancer treatment is not yet well understood.
The widespread adoption of virtual care (telemedicine) due to the pandemic was part of a public safety plan to both curb the spread of COVID-19 and maintain cancer care continuity in Ontario, Canada (9,10). In most cancer centers, telemedicine clinics were rapidly implemented without a comprehensive assessment of their impact on patient outcomes or experience. Previous debates about the value of virtual care were quickly bypassed by the urgency of the COVID-19 crisis and the absolute necessity to continue with some cancer treatments (10). Before COVID-19, only 20% of Ontario oncologists used telemedicine and did so only informally (10). Pre-pandemic research finds that patients view telemedicine as feasible and acceptable for cancer care ranging from prevention to surveillance (11–18). Since the pandemic onset, several survey-based studies have reported cancer patients’ general satisfaction with virtual care (19–22). However, we currently know little about cancer patient experiences with, and perspectives on, the rapid shift to this modality during COVID-19, and little about their perceptions of risk related to in-person cancer care during a global pandemic.
To better understand cancer patient experience and perspectives on ambulatory cancer treatment during the early period of the COVID-19 pandemic, we conducted an exploratory, qualitative study. Our specific objectives were to examine (i) patient-perceived risks related to COVID-19 and experiences with outpatient cancer treatment, and (ii) patient-perceived and experienced benefits and drawbacks of virtual cancer care. In exploring their experiences and views, we sought to identify ways to inform patient-centered clinical practice and support patients undergoing cancer treatment or surveillance during COVID-19.
Methods
Study Design and Setting
We conducted a qualitative description study using online focus groups (23). Qualitative description is a commonly used methodology in health care research whereby the primary goal is to gather and descriptively summarize major themes in the data as reported by participants. A qualitative approach was deemed appropriate to capture, in the patients’ own words, their experience of and views on cancer care during a pandemic. This approach aligns with a recent call to examine and evaluate the patient experience of virtual cancer care throughout the pandemic to optimize its future use (24).
The study was conducted at the Odette Cancer Center at Sunnybrook Health Sciences Center in Toronto, the second-largest Canadian cancer center and the sixth-largest in North America 5374. Our hospital treated the first presumptive case of COVID-19 in Ontario on January 25, 2020; this was the first reported case in Canada (25). Following a declared state of emergency on March 17, 2020, rapid changes to cancer care were adopted. The cancer center is physically located on the larger hospital campus and is attached by a tunnel to the main hospital. Screening for COVID-related symptoms was instituted at every hospital door; personal protective equipment precautions were more gradually put in place throughout the center. Numerous pandemic plans for the de-escalation and limitation of services were created at the institutional level. A number of cancer surgeries were delayed immediately. Visitors were completely restricted from the hospital requiring patients to attend in-person appointments alone. Where possible, cancer care providers were urged to move to virtual care. Provincially, new temporary physician compensation codes for telemedicine were instituted. The vast majority of telemedicine was via telephone with very few clinicians adopting video platforms due to the initial lack of institutional support.
Sampling and Recruitment
A purposive sampling strategy identified English-speaking individuals ≥18 years of age who were under active management or observation for a diagnosed malignancy (26). Care providers identified eligible individuals who were subsequently contacted by a study coordinator for informed consent. Participants were consented verbally and were instructed on using Zoom© video or audio for virtual focus groups. During a test session, the coordinator administered three questionnaires to collect information on self-reported digital literacy, computer proficiency, and COVID-19-related anxiety.
Data Collection and Analysis
Between June 24, 2020, and August 6, 2020, focus group data were collected. The groups were primarily organized by the intent of participants’ cancer treatment, either curative or non-curative, to maximize the likelihood of shared experience among them. Each session included three to five participants and was facilitated by an experienced moderator who was not known to participants. The moderator’s question guide was developed by the study team who have combined expertise in medical, hematological, and surgical oncology, quality improvement, and qualitative research methods. Semi-structured, open-ended questions were posed to elicit participants’ responses in two main domains of interest: perceived risks associated with COVID-19 and cancer treatment, and experience with virtual care. The questions also explored participants’ consumption of information about the community spread of COVID-19, risks, personal safety practices, and improvement opportunities for patient experience. Focus groups were audio-recorded and transcribed. Individual interviews were offered to participants who were unavailable during scheduled focus groups.
Data were analyzed iteratively and inductively using thematic analysis techniques (27). The first two transcripts were read and discussed among multiple team members to assess question-wording and identify salient ideas and developing themes. All transcripts were then iteratively coded by LGC using a constant comparative process to label recurring themes and sub-themes within the two primary research domains. Data collection and analysis continued to the point of thematic saturation when no new information was generated through participant discussion and no further themes were identified (26). Previous research demonstrates an adequate sample size to be around three focus groups of homogeneous participant groups after which the most prevalent themes on a given topic are identified (28). Because they were virtual, each of our focus groups was comprised of a smaller, more manageable size for the virtual platform than is typical for in-person focus groups. We therefore achieved saturation after six focus groups. Nvivo software was used for data management.
Results
Twenty-two individuals participated in six focus groups and two individual interviews. Thirteen participants were female, with a median participant age of 55.5 (ranging from 28 to 86 years) (Table 1). Twelve participants were under surveillance for their cancer while nine participants were undergoing active treatment. One participant was diagnosed with idiopathic thrombocytopenic purpura and was being treated in the cancer center. At the time of the study, 10 participants had experienced at least one telephone appointment with a member of their oncology team, one participant had experienced only video appointments and five participants had experienced both telephone and video appointments. Five participants had experienced telephone or video appointments with non-oncology health care providers. One participant had only in-person visits at the time of the study. Focus groups lasted on average 75 min.
Number of Participants (and as % of Total Participants) Falling Into Each Category is Indicated Above. Information About Living Distance was Gathered Verbally From Patients, While the Remaining Details Were Obtained From Patient Electronic Medical Records.

One participant was not diagnosed with cancer but was receiving care from the Cancer Centre. Thus, they are not included in this section of the table.
The participant who was not diagnosed with cancer was undergoing active treatment at the time of the study.
In pre-focus group questionnaires, nine participants (41%) reported having high anxiety of COVID-19 (i.e., “I am concerned about catching COVID-19”). Five participants (23%) self-reported low anxiety (i.e., “I am not concerned”) (Table 2). Among all participants, only one participant (4.5%) considered canceling in-person treatments. Participants mostly self-reported high digital literacy (Table 2). Computer proficiency levels were also high (online Supplemental table).
Number (and %) of Participants Falling Into Each Category is Indicated Above. All Details Were Obtained From Participants Verbally.

Both individuals listed television as an example in the “other” category.
Both individuals listed information technology personnel as an example in the “other” category.
Patient-Perceived Risks due to COVID-19 (Table 3)
Information About Risk
Most participants described getting their COVID-19 information from the television and internet, citing the news and public health as their main sources. They viewed general information about risks to immune-compromised people to apply to them. Many participants undergoing active treatment described having already subscribed to strict safety measures in their everyday lives before pandemic precautions were widely advised, explaining, for example, “When you’re a cancer patient, you have to be careful with everything that you do” (P22). While some increased preventative measures, such as having close family members isolate, most did not describe any increased perception of infection risk related to COVID-19. As one participant stated, “The risk level already of getting sick was high” (P15).
Supporting Quotes.
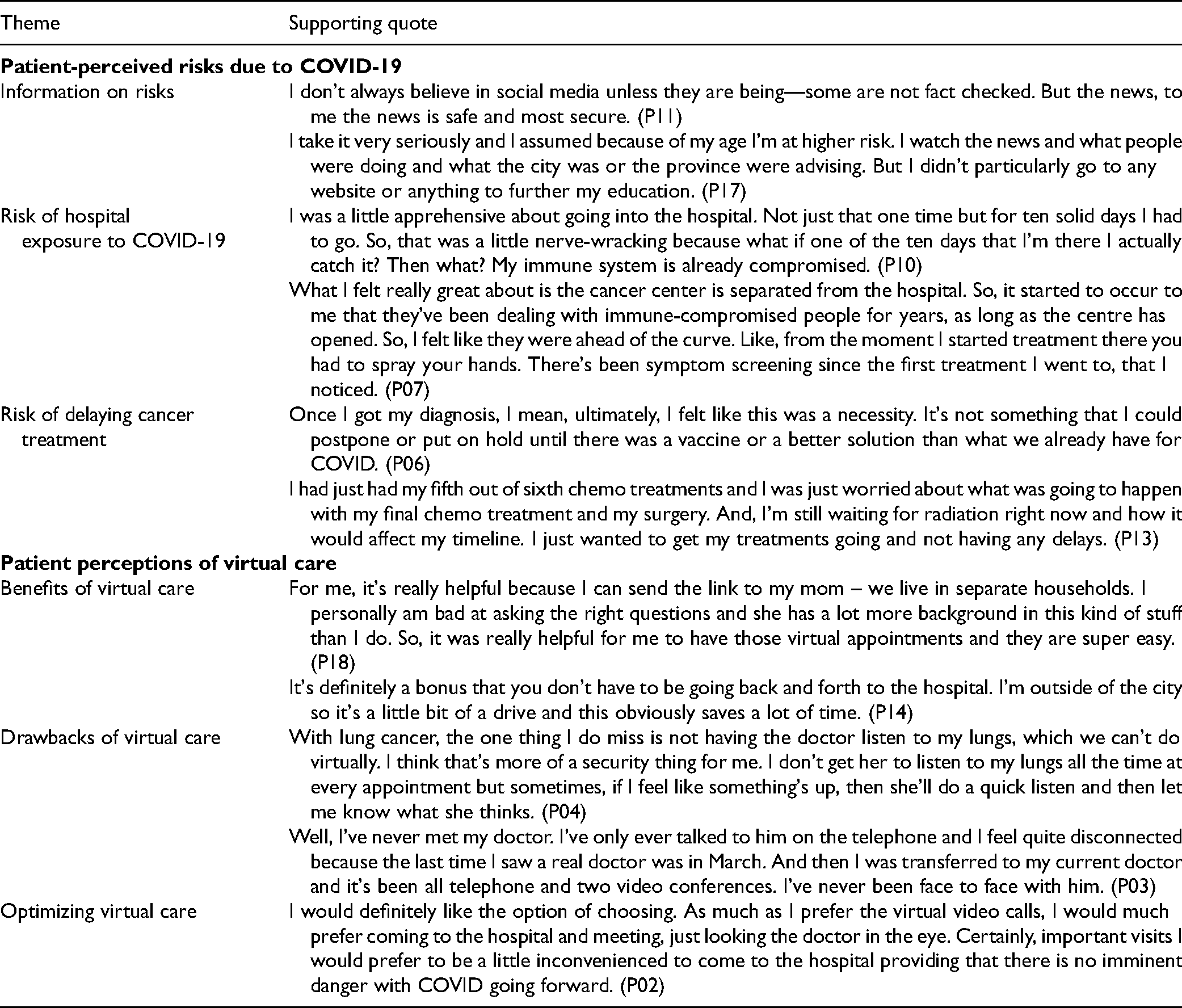
For most participants, no additional information was sought to further understand the potential risks of COVID-19 due to cancer treatment. However, a minority of participants received additional support and personalized information from their oncologist or family physician. They had specific concerns about exposure to COVID-19 in relation to household contacts, understanding symptoms, and workplace risks.
Risk of Hospital Exposure to COVID-19
Many participants expressed concern about the risk of COVID-19 exposure in the hospital. Heightened anxiety was described from March to May when public information about COVID-19 transmission remained unclear, and before COVID-19 symptom screening, mandatory masking and physical distancing measures were widely implemented. Many participants felt that outside of the cancer center there was much less attention to preventive infection control. Participants viewed the cancer center as a safer, more trusted space describing the specialized training of staff, established infection control procedures, and history of treating immuno-compromised patients as critical factors.
From June 2020 onward, increased safety measures were implemented across the hospital and consequently, most participants felt less worried about the risk of exposure during in-person visits. Among those under active treatment, they described “feeling safe” (P13), having “peace of mind” (P21), and “feeling protected” (P05) in the center. They held mixed views on restricting visitors to the center as some participants supported limiting entrance to patients only, while others felt supportive care partners should be allowed inside.
Risk of Delaying Cancer Treatment
Participants were generally more worried about delays to their cancer treatment than they were about contracting COVID-19. Most felt that given the precautions they were already taking, the risk of COVID-19 infection was lower than the risk associated with missed treatment. As explained by one participant, “I was not going to consider postponing any cancer treatments. For my cancer where I am, the risk of getting a virus and having a bad case is in my mind a lot lower than skipping some cancer treatments.” (P01) Treatment delays imposed by the cancer center were therefore of top concern to many participants. A few described increased anxiety as a result: “It felt that my cancer care just came to a dead end. And although I had telephone conversations with my doctor, I wasn't getting any treatment over the telephone. And I felt very anxious, and I think that COVID had a very big psychological impact on me and still has” (P03).
Patient Perceptions of Virtual Cancer Care (Table 3)
Benefits of Virtual Care
Participants described several benefits to virtual care that pertained mostly to its convenience, saving time, and money. Visit types that were viewed to be suited to virtual care included routine follow-up and monitoring, and discussion of unremarkable test results. Accordingly, participants described virtual appointments that worked well for a “status update” (P16) and when “it's not a big concern or it's nothing major” (P13). During the visitor restriction period, telemedicine enabled the inclusion of family members from the same or other households in appointments.
Participants’ virtual appointments were mostly positive experiences. They were viewed as easy to schedule and simple to connect. Most felt that providers were very patient during the call, never rushed through questions, and were respectful of scheduled appointment times. When participants had established relationships with their providers, they appreciated their efforts to connect at unscheduled times.
Drawbacks of Virtual Care
Notwithstanding the perceived convenience of virtual care, participants described numerous downsides. Several visit types were viewed to be incompatible—first time meetings with any provider, diagnosis and new treatment discussions, delivering significant test results, and any situation where a clinical exam is appropriate. For example, one participant seeking psychosocial support declined a first-time virtual visit with a psychologist, explaining, “I was looking so forward to finally sitting down with someone and talking. But virtually, I just didn't feel comfortable because I didn't have that relationship” (P13). Some participants felt that compared to in-person visits, doctors could not assess a patient's condition, in the same way, using telemedicine, for example, noting if they were pale or tired-looking. A few participants felt that they were more likely to forget to ask questions during virtual visits compared to in-person, and they viewed physicians as more difficult to reach by telephone for a follow-up question when this happened. Barriers to relationship building with the care team and accessing emotional support were two significant limitations of virtual care described. Some participants preferred in-person appointments even during COVID-19 as they fostered patient–provider relationships, preserved the “human component of the interaction” (P07), and reduced the anxiety associated with cancer treatment. As one participant explained with respect to their health care team, “Seeing them and seeing how pleasant and calm they were, they made me feel more confident and calm in all my treatments. So, if I had a choice, I would choose to see them for sure” (P08).
Optimizing Virtual Cancer Care
Many participants agreed that patient preference should be taken into consideration when offering virtual appointments because of varying degrees of comfort with technology, potential language or communication barriers, or the patient's preference to be face-to-face with their doctor. Variation in participants’ preferences for care reflected where they were at in their treatment trajectories; the nature of their relationships with their providers (i.e., how long they had been in their care); and the patient-perceived significance of the appointment. Participants suggested process improvements including routinely sharing links to virtual appointments with care partners and family physicians; providing technological support; ensuring easy access to providers in-between appointments for follow-up questions; and, creating a virtual library of resources unique to the cancer center. A virtual care preparation checklist was proposed that could be personalized by patients to set their expectations for the appointment, organize their information, and plan their questions. Several participants indicated cancer teams could routinely provide them with more specific information about protecting themselves and mitigating risks in their cancer care during COVID-19.
Discussion
As cancer care delivery is reorganized to mitigate the fallout of COVID-19, patient experience data are essential for ensuring high-quality patient-centered care. Using a qualitative approach, we have examined patient-perceived risks related to COVID-19 during cancer treatment, and patient experiences with virtual cancer care. A significant finding here is that individuals undergoing cancer treatment are more worried about treatment delays than they are about COVID-19 infection. Moreover, treatment delays may contribute to increased anxiety among cancer patients who generally viewed themselves to be taking the necessary precautions against infections, including COVID-19. While many participants reported anxiety about visiting the hospital, most felt supported by their cancer care providers and the cancer center's efforts to minimize COVID-19 exposure risk. A second major study finding is that although individuals undergoing cancer treatment are likely to be satisfied and accept the shift to virtual care for some appointment types, such as well follow-ups, many prefer being face-to-face with their providers. Despite the convenience of telemedicine, this preference for being in the cancer center was found to sustain the humanistic and therapeutic aspects of the patient–provider relationship that many participants valued and did not want to forego.
With the amount of epidemiologic information about COVID-19 circulating broadly, there is considerable risk for vulnerable patients to develop false beliefs about the threat of infection, potentially contributing to poor physical and mental health (29–31), and anxiety-driven treatment delays (32,33). However, we have found that although cancer patients experience some COVID-19 anxiety, this is not a barrier to continuing their in-person cancer care (34). Trust in the safety of the health system and the cancer center, as well as reassurance from their health care providers, were key to feeling safe to continue care. Despite this expressed sense of security, providers must weigh patient-perceived risks and suitability for virtual care against guidelines advocating treatment delays in their respective clinical settings (35–38). To further support patients, providers are encouraged to normalize the potential for increased anxiety around delayed cancer treatment and to identify opportunities for enhanced psychosocial support (39). Practical communication strategies regarding uncertainties related to cancer treatment and COVID-19 have been established, including Dhawan et al.’s adaptation of VitalTalk’s Naming, Understanding, Respecting, Supporting, and Exploring (NURSE) statements to guide clinicians in this regard (40).
Further, our findings suggest that while virtual care is technically possible and acceptable for individuals of all ages, cancer patients may worry about whether the empathic care that they rely on in-person can be delivered virtually. Considering the expansive use of telemedicine during the pandemic, providers must adopt strategies for achieving virtual empathy and ensuring the continuity of this supportive patient-centered care (41–43). Some such approaches for “digital empathy” and preserving relationship-centered care have been disseminated in response to COVID-19, emphasizing the shift in verbal and body language needed to achieve online rapport and trust (44–47). Further, techniques to establish an intentional “webside manner” may help to sustain the empathic connection so valued by patients described herein (46).
Study Limitations
While consistent with qualitative methodology, study findings may be limited in their generalizability due to the small study sample from one cancer center. These findings reflect the views and experiences of a diverse group of English-speaking adults undergoing cancer treatment who generally reported high levels of comfort with computers and technology, and moderate levels of COVID-19-related anxiety.
Conclusion
While COVID-19 poses an ongoing threat to public health and safety, patients undergoing cancer treatment worry more about disruptions to their cancer care. For most, virtual care is generally acceptable and possible at certain points in their cancer treatment trajectory but nuances in the appropriateness and adequacy of virtual care still need to be explored. Given the significance of empathy and support that patients experience in the cancer centers, attention to preserving the humanistic aspects of cancer care should be at the forefront of this virtual endeavor. Additional patient experience data exploring these experiences in-depth from both patients and providers will be essential to the design and implementation of a sustainable and effective virtual cancer care system.
Authors Note
All procedures in this study were conducted in accordance with the Sunnybrook Health Sciences Center research ethics committee's (ID #1635) approved protocols. Verbal informed consent was obtained from the patients for their anonymized information to be published in this article.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735211039328 - Supplemental material for Cancer Treatment During COVID-19: A Qualitative Analysis of Patient-Perceived Risks and Experiences with Virtual Care
Supplemental material, sj-docx-1-jpx-10.1177_23743735211039328 for Cancer Treatment During COVID-19: A Qualitative Analysis of Patient-Perceived Risks and Experiences with Virtual Care by Lesley Gotlib Conn, Houman Tahmasebi, Nicholas Meti, Frances C. Wright, Alia Thawer, Matthew Cheung and Simron Singh in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research, 2019 Novel Coronavirus (2019-nCoV) Rapid Research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.