
Abstract
Key Messages
Our review identified 9 diabetes registries. Although the 9 registries involved some degree of patient engagement, there were varying levels of engagement throughout. The purpose of patient registries aligned more with population health surveillance and clinical care, rather than building a diabetes community. Peer-reviewed literature to date highlights a paucity of patient engagement in patient registries for diabetes.
Introduction
Over 10% of Canadians are currently diagnosed with diabetes, including type 1, type 2, and gestational diabetes. 1 This number is projected to rise worldwide, reaching over 578 million by 2030. 2 As a tool for monitoring and surveillance, patient registries can be used to collect and store data relevant to patient outcomes. 3 Although there is no consistent definition of a patient registry, 4 a patient registry involves using an organized system to facilitate the collection of data on a specific population of individuals that can be used to evaluate certain outcomes to support a disclosed purpose (ie, research, policy, clinical, or other).5,6
There are currently hundreds of patient registries globally that contribute to and advance existing health systems. 7 In the diabetes community, patient registries have become more prevalent in recent decades. 8 Numerous countries have employed diabetes registries to survey the prevalence of diabetes and monitor access and quality of diabetes services. 3 In most cases, national diabetes registries recruit individuals directly through administrative health databases and/or electronic medical records (EMRs) via clinical healthcare settings, with some registries seeking individuals through physician referrals. 9 Similar to the limitations of patient registries globally, 10 most diabetes registries do not allow individual patients to access their information or inform their care. 9 Examples of such large diabetes registries include the Diabetes Collaborative Registry in the United States, the National Diabetes Register (NDR) in Sweden, the Diabetes-Patienten-Verlaufsdokumentation (DPV) in Germany, and the National Diabetes Services Scheme (NDSS) in Australia.
Of the 12 largest national diabetes registries identified in a recent systematic review, only the NDSS provides diabetes self-management support resources to registry participants.9,11 These support resources include practical help and guidance, diabetes health information, and subsidized diabetes products. 11 Providing self-management education and support for people living with diabetes is recommended,12,13 as self-management supports the optimization of diabetes control and the prevention of complications. 14 Additionally, only 3 registries provide an avenue to collect self-reported outcome measures (the Norweigan Diabetes Register for Adults [NDR-A], Swedish NDR, and German DPV), with the NDR-A purposefully recruiting participants to report on topical and timely concerns such as COVID and diabetes distress.9,15,16 The Swedish NDR, particularly, supports individuals to actively monitor their data, interact with healthcare providers, and participate in shared decision-making. 17 A similar trend is seen in pediatric diabetes registries, with the Swedish Childhood Diabetes Registry being one of the only registries to provide participants or their families access to their information. 17
Increased patient engagement within patient registries indicates the beginning of a shift to understand better and meet the needs of individuals with diabetes rather than monitoring clinical outcomes alone. 7 As described by Abelson et al, 18 patient engagement can be defined as a “meaningful and active collaboration in governance, priority setting, conducting research and knowledge translation” (p. 5). In alignment with goal-oriented care, patient engagement allows for data collection and monitoring within the registry to reflect what is most meaningful to patients. 10 Various frameworks have been developed to communicate levels of patient engagement, with one combined framework describing 3 levels of shared leadership between researchers and their patients. This engagement typology emphasizes a partnership between researchers and their patients in the exchange of information, consultation, or participation.18–20 Patient engagement continues to evolve 21 to provide individuals with diabetes with the ability to connect with peers, practice advocacy and self-expression, and share information. 22 Patient registries may offer an opportunity to merge the collection of clinical and self-reported data with patient engagement to share evidence-based information on diabetes management and facilitate positive connections with peers and the registry curators.
Considering the known utility and future opportunities of patient registries, we seek to understand what patient registries currently exist that emphasize patient engagement and are led or operated with the support of patient communities, rather than a database of patient-derived data only. We conducted a scoping review of peer-reviewed published literature to identify patient-focused (eg, patient-led, patient-operated, or patient-accessed) registries globally. We aimed to understand the goals, purpose, and context for diabetes registries defined as patient-focused and how patients are engaged with these registries.
Method
To begin to understand the ambiguity of the literature and the lack of definition of the term “registries,” we used a scoping review approach to understand the breadth of the literature on this topic. 23 A scoping review allowed us to conduct a broad literature view, include a variety of study designs, and explore the use of patient registries in multiple diabetes-related settings. We followed the PRISMA checklist for scoping reviews throughout our review. 24
Search Strategy
Broadsearch terms, databases, and strategies were developed in consultation with a research librarian (Appendix 1). We searched Pubmed, MEDLINE, Embase, and Emcare from inception to April 16, 2023. Results from the search were deduplicated, and citations were uploaded to a secure internet-based platform for screening (DistillerSR, Evidence Partners Inc., Ottawa, Canada). Eligible studies of any design/type had to be published in English in a peer-reviewed journal and meet the following criteria: (1) the population of interest is people with diabetes mellitus, including type 1 diabetes, type 2 diabetes, and/or gestational diabetes; and (2) the study describes a registry that is patient-focused (eg, patient-led, patient-operated, or patient-accessed). Studies where the registry was a main component of a trial (ie, used for recruitment or to support intervention delivery) or a secondary analysis were also included. Outcomes were not used to include or exclude studies. Studies were excluded if they described a physician-driven exclusively, and/or genetic database registry.
Literature Selection
A team of researchers conducted the screening and data extraction. A minimum of 2 reviewers were required to independently and in duplicate screen titles and abstracts of all potentially eligible studies. Articles marked for inclusion by either team member went on to full-text screening which was completed independently and in duplicate by 2 team members and required consensus for inclusion or exclusion. Conflicts were resolved through discussion with the lead researchers of this review. After confirmation of the included studies, we looked for related publications that met our search dates and inclusion criteria and grouped multiple publications that were based on the same study/intervention.
Data Extraction
We developed, piloted, and deployed standardized forms for data extraction which were housed in a web-based systematic review software program (DistillerSR). All authors provided feedback and approved the components of these forms. For each primary study, 1 team member extracted study characteristics (including the country of origin, healthcare setting, aim of study, aim of registry, sample size, study design, and registry methodology) and the patient, disease, and provider characteristics included in the studies. We applied the engagement framework by Abelson to understand the level of patient engagement occurring within each registry. 18 This typology describes an exchange of information, consultation, or participation between researchers and patients, with shared leadership occurring at each level of engagement. This framework is highlighted in Figure 1 and applied to each of the included studies. Two team members independently verified all extracted data and disagreements were resolved through discussion and/or third-party consultation.
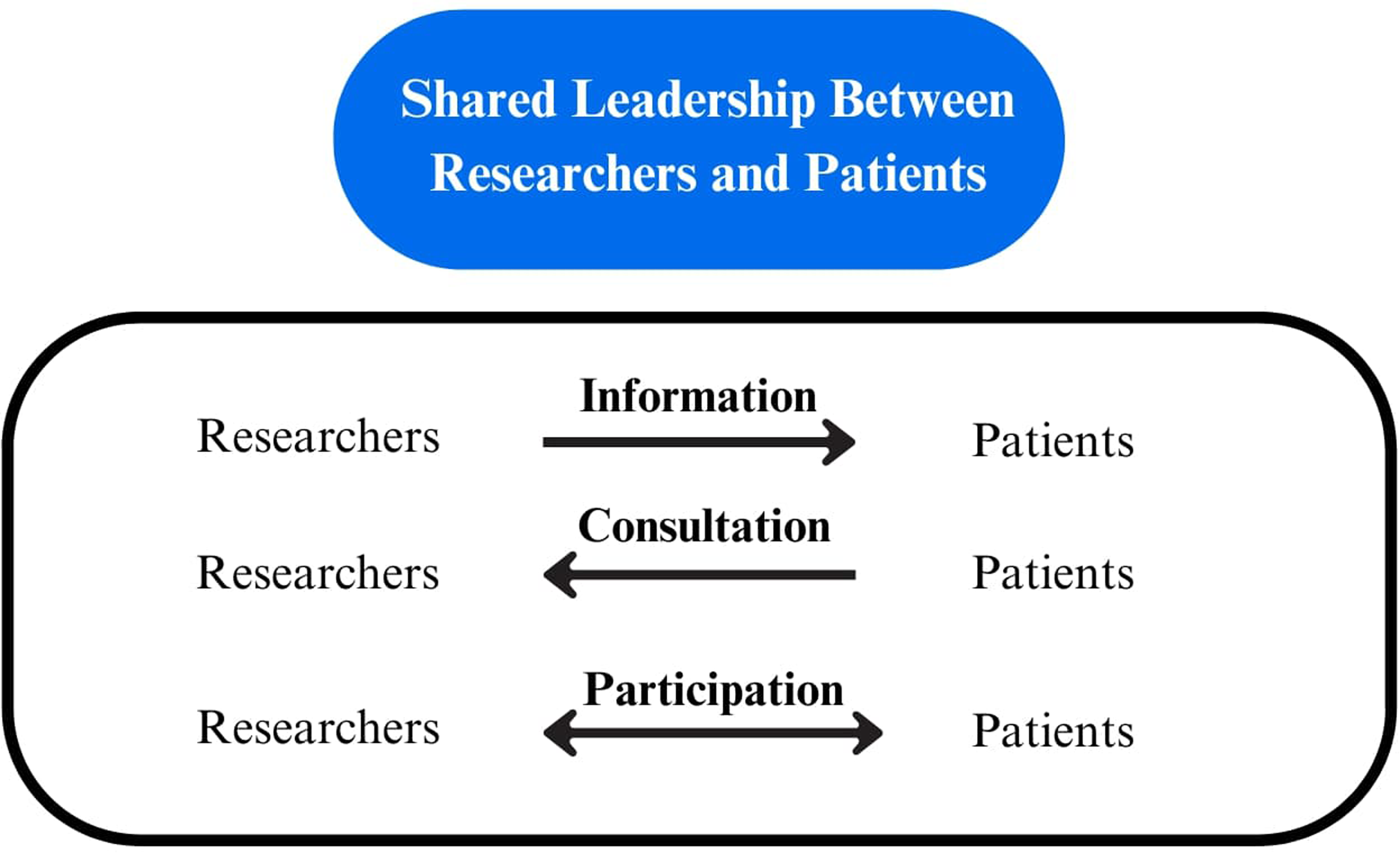
Patient engagement framework adapted from Abelson. 18
Results
The search identified 346 citations to be assessed after the removal of duplicates. A total of 49 full-text articles were assessed for eligibility and 40 were excluded due to: (a) not being created or facilitated by or for patients with diabetes; or (b) not including patients with diabetes. The final group of studies (n = 9) was included in our scoping review.25–33 Figure 2 summarizes the study selection process for this review.

PRISMA flowchart of included studies.
Characteristics of Included Studies
The group of included papers was mostly retrospective cross-sectional studies,25–27,30,32,33 with some being randomized controlled trials,28,29 and 1 study testing the piloting phase of their registry. 31 There were 4 registries based out of the United States,27,29,31,32 2 registries from Canada,30,33 and 1 registry from Australia, 28 Israel, 26 and Germany, 25 respectively. The study from Germany included a registry that was a subsample of a larger network of registries across Germany, Austria, Switzerland, and Luxembourg. 25 The registries were developed and utilized by researchers in multiple settings, including community-based,31–33 outpatient,25,27 and primary care settings.26,29 The number of participants within the registries varied from 19 patients for a study pilot testing a registry 31 to 3,936,800 patients for a government registry actively running for 12 years. 26 The goals of the registries were diverse and included: evaluating patient characteristics (blood pressure, lipids, physical activity),26,31,34 monitoring diabetes populations using EMR data 25 developing a standardized referral and follow-up system for primary care physicians using EMR data, 26 evaluating community-based 28 and clinical interventions, 29 improving access to care and patient empowerment, 32 and fostering diabetes friendly communities. 33 Some of the registries were described as web-based30,32,33 with data being submitted and stored electronically, and 1 registry offered opportunities to attend in-person educational events as a member of the online patient registry. 33 Patients were recruited through flyers, letters, emails, events, multimedia, social media, or in-person after a follow-up appointment.30,33 Healthcare providers were also invited to join certain registries to encourage their patients to practice self-management behaviors. 33 A summary of characteristics of the included studies can be found in Table 1, with detailed characteristics found in Supplemental Table S1.
Characteristics of Included Studies.

NR, not reported.
*Further details available in Supplemental Table.
Characteristics of Included Patients and Participants
Data on the characteristics of patients was collected within the registries for 7 of the 9 included studies.25–27,29,30,32,33 Specifically, the registries of these studies collected information on gender,25–27,30,32,33 age,25–27,29,30,32,33 race/ethnicity,25,27,29,30,32,33 location,25,26,30,33 and social determinants of health26,30,32,33 such as insurance type, education, and location. None of the included studies collected data on the characteristics of healthcare providers. Seven of the studies incorporated diabetes-related patient information within the registry.25–27,29,30,32,33 This included years of diagnosis and type of diabetes. Six studies report capturing HbA1c.25–27,29,30,32 Three studies also collected information on comorbidities28,33 and 5 reported self-management behaviors within the registry.25,27,30,32,33 A detailed outline of patient, provider, and disease characteristics within the registries can be found in Table 2.
Characteristics Within the Registry.
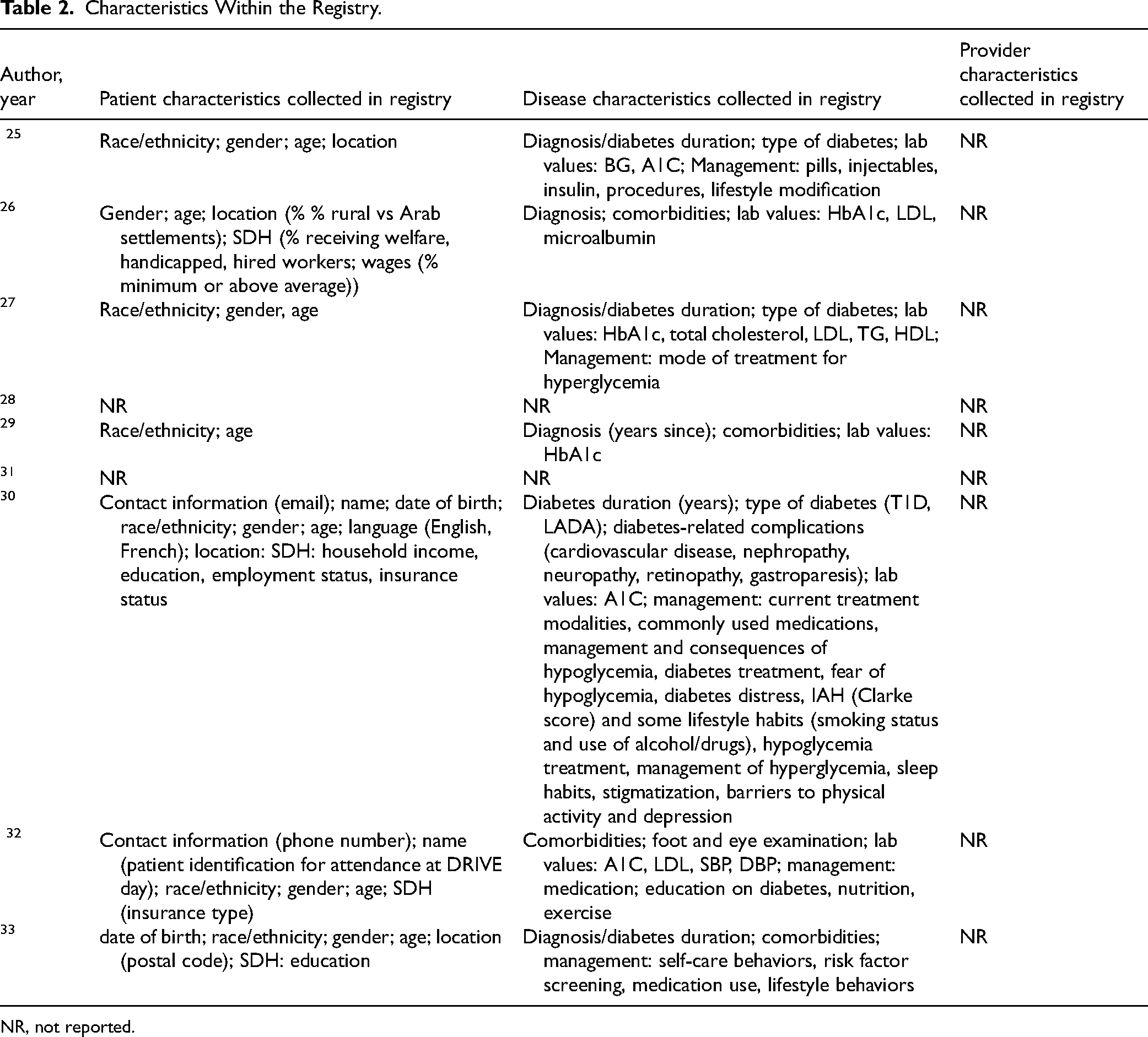
NR, not reported.
Degree of Patient Engagement
Patient engagement in the included registries was described in 4 studies.26,28,30,33 The degree of patient engagement varied, with 2 registries classified under the “participation” level of the patient engagement framework.18,30,33 One of these registries was codeveloped with patient partners 30 and another conducted a needs assessment with relevant stakeholders, including patients ahead of development. 33 The 2 registries classified under the “information” level of patient engagement 18 utilized the registries in different ways, including accessing subsidized products (eg, coupons for devices) 28 and attending events and workshops offered through the registry. 26 Resources available for patients within these registries include self-care kits, videos, and cookbooks, 26 educational websites,26,30,33 links to self-management services, 28 and newsletters. 33 An overview of patient engagement is summarized in Table 1.
Discussion
This scoping review aimed to assess the current state of patient diabetes registries. Our findings demonstrate the diversity of 9 diabetes patient registries of varying goals and purposes, that claim to be “patient-focused” in development and implementation. For multiple studies, the purpose of the registry was not disclosed.25,27,29,31 Through our scoping review approach, we included studies where the diabetes registry was a main component of a trial or a secondary analysis to highlight the different uses of patient registries across the diabetes landscape. Communicating the purpose of a registry is an important component of registry development, as it allows the data collection to be purpose-driven, identifies important stakeholders, 4 and supports the ability to obtain funding. 35 For the included papers that did describe the purpose of their registries26,28, 30, 32 , 33 the variety of rationales behind creating a registry (ie, surveillance, clinical care, program evaluation, and community development) attests to how different stakeholders, including individuals with diabetes, utilize patient registries and maximize their value. 4
We also included registries where patient engagement was mentioned but was not the main focus of the registry. This emphasizes the discrepancies that currently exist in diabetes patient registries that report on patient engagement. Two of the included studies collected information from electronic health records (EMRs)25,26 rather than including an element of active data collection. Linking primary and secondary sources of data can help to enhance a registry and open up opportunities to explore primary and secondary objectives. 4 However, depending on the purpose of the registry and available funding, the information sources utilized in a registry can be customized to address specific research questions. 5
The degree to which patients were actively participating in engagement with researchers was reported in 2 of the included studies, with 1 study conducting a needs assessment with diabetes stakeholders (including those living with diabetes) ahead of inception, 33 and another study codesigning the registry with patient partners. 30 Involving participants in active participation at enrollment increases the likelihood of ongoing participation for the life of the registry.4,5 For registries including clinical data for individuals accessing care from multiple sources, or patient-reported outcome data, incorporating a plan that follows participants across their circle of care is recommended. 5 These 2 studies also relied on self-reported data to gather information from participants,30,33 emphasizing the knowledge transfer that was actively occurring between researchers and patients. 18
Limitations
Strengths of our review include our rigorous search strategy, strict inclusion criteria, and strong methodological approach to comprehensively assess the current literature on diabetes registries. A limitation of our review is that we only searched published literature. Although unlikely, we recognize that the existence of patient registries that enhance patient engagement may be available and could be assessed through internet searches. Additionally, we conducted a scoping review to explore this topic with an understanding that the term “registry” is not clearly defined. Our search strategy was broad and our inclusion criteria allowed us to capture the varying definitions and uses of registries in the diabetes context, which led to the inclusion of studies that did not describe the collection of data or omitted information that would help us better understand the level of patient engagement within the registry.
Our group aims to build on the findings of this review by developing a patient-led and reported diabetes registry with a focus on patient engagement, specifically for information and participation (eg, knowledge transfer). 18 The registry will provide an avenue for participants to engage with researchers, and access evidence-based information and resources on diabetes management. In alignment with the patient engagement framework, 18 registry participants will be actively involved in shared leadership within the registry and will contribute to an ongoing cycle of knowledge transfer. This will occur through self-reported data, feedback, and input in what information is offered to patients within the registry.
Conclusion
The results of our scoping review identified heterogeneity in the definition of patient-focused registries, goals, and purposes, with some registries providing limited patient engagement opportunities. As patient registries continue to evolve globally to integrate active participation, 7 our findings support the need for future patient registries to be developed that incorporate patient engagement from registry development to the ongoing management of the registry. Increased engagement will support individuals living with diabetes in monitoring information that is most relevant to them and adhering to long-term self-management.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251314620 - Supplemental material for Understanding Patient Registries for Diabetes: A Scoping Review of Published Literature
Supplemental material, sj-docx-1-jpx-10.1177_23743735251314620 for Understanding Patient Registries for Diabetes: A Scoping Review of Published Literature by Lana Moayad, Paige Alliston, Saira Khalid, Donna Fitzpatrick-Lewis, Hertzel C. Gerstein and Diana Sherifali in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735251314620 - Supplemental material for Understanding Patient Registries for Diabetes: A Scoping Review of Published Literature
Supplemental material, sj-docx-2-jpx-10.1177_23743735251314620 for Understanding Patient Registries for Diabetes: A Scoping Review of Published Literature by Lana Moayad, Paige Alliston, Saira Khalid, Donna Fitzpatrick-Lewis, Hertzel C. Gerstein and Diana Sherifali in Journal of Patient Experience
Footnotes
Acknowledgments
D.S. acknowledges the support of Heather M. Arthur, Population Health Research Institute/Hamilton Health Sciences Chair in Inter-Professional Health Research, and the support of the McMaster Evidence Review and Synthesis Team.
Author Contributions
LM, PA, DS, DFL, and HG contributed to the design of the review. PA, DS, DFL, and SK implemented the review (screening, data extraction, and synthesis). LM, PA, DS, and HG assisted in the interpretation and writing of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
There are no human participants in this article and informed consent is not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.