
Abstract
A common recommendation to improve the management of low back pain (LBP) is the use of interdisciplinary teams. However, many challenges remain in establishing interdisciplinary care, particularly in community-based primary care settings. This study explored patients’ experiences with interdisciplinary care for LBP using an applied phenomenological research approach. Semistructured open-ended interviews were conducted with fifteen adults enrolled in a 6-month interdisciplinary LBP program within an integrated care network. The analysis included detailed descriptions of participants’ experiences and interpretations by the researchers of the main themes: (i) challenging start—“It's intimidating,” (ii) desire for flexibility—“I didn’t need as much,” (iii) better collaboration—“They are all together,” (iv) grasping the pain issue—“They helped,” (v) care was responsive to needs and experience—“Always centered on me, not general,” (vi) meanings of recovery—“I’m able to function.” Participants viewed the interdisciplinary LBP program as the culmination of a long journey toward recovery. The findings identified as important to patients contribute to our understanding of how to optimize patient-centered care for individuals living with chronic pain.
Keywords
Introduction
Healthcare support for people living with chronic health conditions remains far from optimal, with many reporting insufficient care and resources to manage their condition effectively. 1 This is also the case for individuals living with chronic pain.2,3 Low back pain (LBP) is the most common nonspecific chronic pain conditions, leading to disability and substantial public health costs due to medical expenses, work absence, and reduced quality of life.4,5 Managing LBP often requires a combination of nonpharmacological and pharmacological approaches.6-8
Clinical guidelines for managing LBP recommend nonpharmacological approaches such as self-management education, cognitive-behavioral therapy, exercise, and appropriate complementary and alternative medicine, followed by cautious medication use and potential surgery.6-10 Multidisciplinary and interdisciplinary programs are advised for those unresponsive to standard treatments. 10 While multidisciplinary approaches involve various healthcare providers, interdisciplinary approaches emphasize coordinated services by a cohesive team in a single facility, improving patient outcomes.11,12
Pain is a common reason for medical consultations, accounting for an estimated 40% of primary care visits.2,13 Primary care, offering better health outcomes and cost control, should ideally manage LBP early to prevent chronicity and optimize outcomes.14-17 However, primary care faces service gaps in managing chronic pain, including insufficient self-management support and inadequate education for primary care clinicians.18-20
Interdisciplinary programs, endorsed by multiple guidelines, present a solution but face challenges in community-based settings.18,20,21 There is a need for effective implementation strategies and measurement of patient experiences to inform program efficacy. 22 Understanding patient experiences through patient-centered care (PCC) can enhance the design and implementation of interdisciplinary chronic pain management.23-26 Existing patient experience frameworks and measures often overlook aspects critical to chronic disease management in primary care.24,27-29 Therefore, qualitative research focusing on patient experiences is essential. 30 This study aims to investigate patient experiences with an interdisciplinary program for LBP by exploring: what are the individual experiences of people living with chronic pain being treated for LBP using an interdisciplinary team (IDT) care approach?
Method
To better understand IDT care, we employed an applied qualitative phenomenological approach, studying the lived and prereflective experiences of individuals with LBP. 31 We followed the Standards for Reporting Qualitative Research guidelines to report the study. 32
Study Design
Phenomenology is a philosophy of understanding that explores and gains deeper insight into human experiences. 33 In this way, “phenomenologists seek to reunite science with life and to explore the relationship between the abstract world of the sciences and the concrete world of human experience.” 34 This approach allows clinicians and researchers to “enter the world of illness as lived by patients” to explore their experience of illness or of healthcare. 34 We built on the assertion that preexisting ideas and experiences are essential to understanding a phenomenon. 35 Our preunderstandings of the phenomenon included prior work, 12 lower support for team-based care from the public and physicians compared to other health professionals, 36 and the asymmetrical patient-physician relationship.
Settings
This research inquiry was conducted within an interdisciplinary primary care program for individuals with LBP, part of a larger initiative on chronic pain care (Quebec, Canada).37,38 Four clinics participated, delivering a 6-month interdisciplinary care program with contributions from a nurse, physician, physiotherapist, and psychologist.
Participants and Sampling
The research participants were adults diagnosed with subacute or chronic LBP who were referred by primary care physicians. We used purposive criterion-based sampling to ensure maximum variation across several characteristics (Table 1).39,40 In applied phenomenological research, sample size prioritizes the quality and depth of participants’ narratives. Considering population heterogeneity, selection criteria, and available resources, 15 participants were recruited for this study (Table 2).41-43
Criteria-Based Selection.

Risk factor for chronicization of acute and subacute low back pain and psychosocial barriers to recovery.
Physical and psychosocial risk of poor prognosis.
Characteristics of Participants.
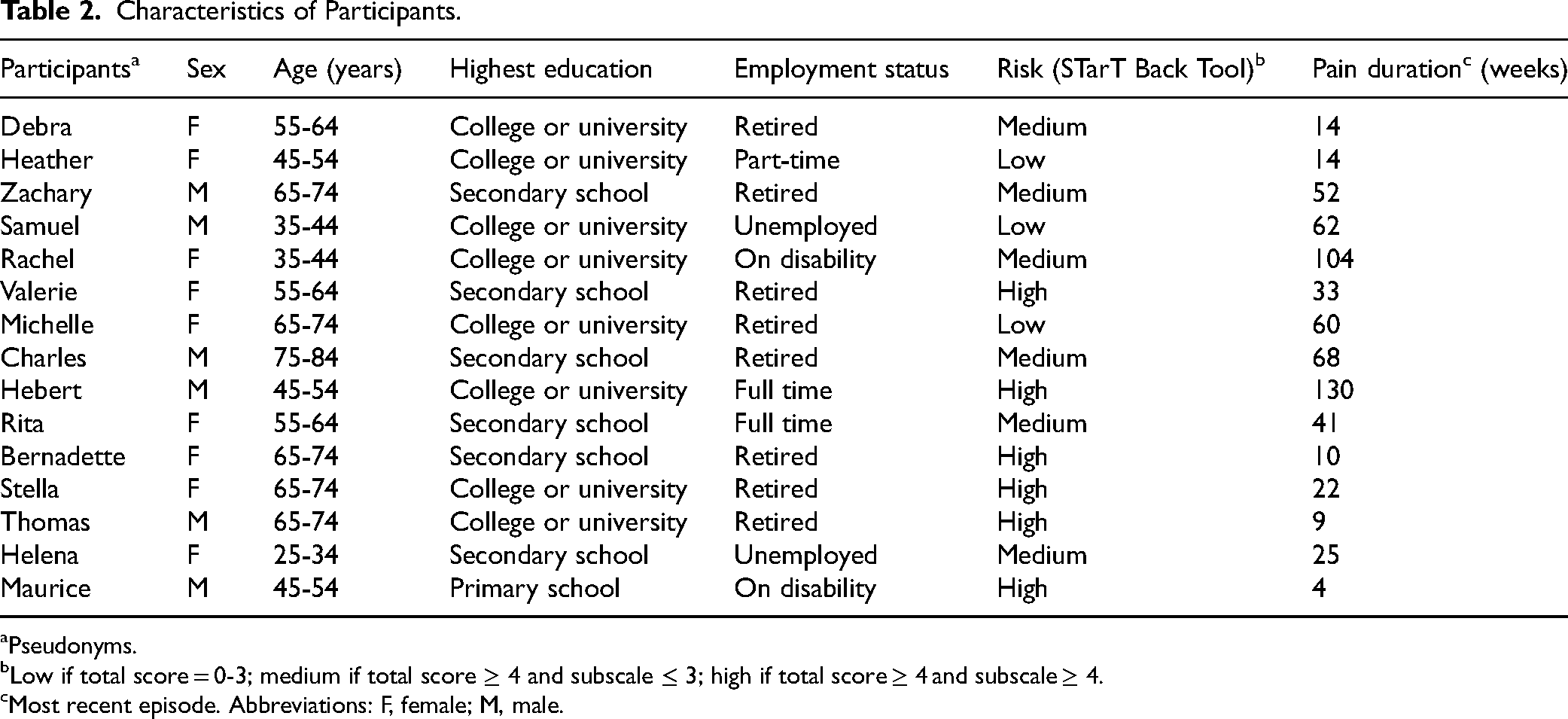
Pseudonyms.
Low if total score = 0-3; medium if total score ≥ 4 and subscale ≤ 3; high if total score ≥ 4 and subscale ≥ 4.
Most recent episode. Abbreviations: F, female; M, male.
Data Collection
An interview guide (Supplementary File S1), developed in English and translated into French, was based on literature review and program objectives. Mock pilot interviews were conducted with 2 individuals, not part of the study participants, including one with a Quebec native French speaking person to ensure the clarity of the interview questions once translated into French. Participants detailed their pain history and IDT care experience.
Recruitment was facilitated by the IDT clinics and through the identification of patient profiles using the REDCap system. 60 Each IDT clinic was contacted to obtain the REDCap IDs for patients scheduled for their 3- and 6-month visits. Once their eligibility was assessed compared with the selection criteria (Table 1), the IDs of selected patients were communicated to the IDT clinic staff. The staff of the clinics contacted the selected patients and confirmed their willingness to participate and their availability for a 30-to-60-min interview after their visit. This approach ensured that participants would be prepared and able to discuss their experiences in depth. Eligible individuals who agreed to participate were interviewed at 3- and 6-month visits or at 6-month visit only, for practical reasons. Interviews, conducted at clinics or by phone, ensured participants’ comfort and willingness to share their experiences, and were audio-recorded. Information from participants who withdrew from the program was also collected. 37
Data Analysis
Interviews were transcribed verbatim, anonymized and entered into Qualrus software, then analyzed using an interpretative phenomenological approach, combining description and interpretation. 61 This involved extracting significant data units expressions, sentences, or paragraphs that highlight key elements of the phenomenon, capturing essential aspects of the participants’ lived experiences related to the subject under study, formulating meaning observations by answering the question “What does this sentence/segment reveal about the experience being described?” through an iterative process, and grouping similar themes into meta-themes. The 5 steps of the analysis are summarized in Supplemental Figure S2 (Supplementary File S2). Various strategies were used to enhance trustworthiness and credibility of the research findings: review of the transcripts to ensure their accuracy, continuing conversation with experts (MH, RH) during the analysis process, maintenance of a reflexive log.
Findings
The participants described their experience of IDT care as the culmination of a long journey to recovery in their search for a solution to their LBP condition. Participant synopses are provided to convey their stories (Table 3). Selected verbatim quotes illustrate the analysis.
Synopses of Participants.

Abbreviations: LBP, low back pain; IDT, interdisciplinary team.
Challenging Start: “It's Intimidating”
Two participants described their first IDT meeting as intimidating due to the presence of all 4 clinicians in the same room. Michelle reported: “It looked like an office where you would meet with bosses when applying for a job. But that's okay; it lasted how long? A second? The time it took to recognize the faces, to know who does what; it's always a bit intimidating [but] I’ve nothing negative to say.” Maurice also noted: “I was … a bit nervous. At first, I didn’t know anyone, not 1 person in the group of 4, but after that, like yesterday, we met again all together sometimes for the group of 4, then I was all alone with them. It wasn’t long before my nervousness disappeared.”
The presence of all clinicians and the delineation of their roles during the first IDT evaluation helped mitigate feelings of intimidation and nervousness. Michelle shared: “They explained the program to me, they explained each person's function, from then on I trusted them.” Two participants echoed this sentiment: “At first, I was a bit nervous but after that I understood that it was a group of people who wanted to help me and treat my pain.” (Maurice); “Usually (because) I get to know the person, and I get to know what they do, and I know that they're there to help. So that … makes it a little easier on me.” (Helena).
Desire for Flexibility: “I Didn’t Need as Much”
Participants acknowledged the importance of all clinicians but expressed a desire for flexibility to “use” them as needed. For example, some participants felt they did not need the services of a psychologist. Debra mentioned: “I didn't need as much from the psychologist … I mean, I am still trying to figure out the role of the psychologist in this program.” Zachary simply stated: “No, I don't need [a] psychologist.” In contrast, Michelle praised the psychologist's contribution: “She gave some tips because it's the stress too; I didn’t have to see the doctor.” Rita expressed a need for more time with the physiotherapist: “I would have liked to have a bit more time with the physiotherapist.”
The role of the nurse was also not well understood by 2 participants. Helena noted: “I don’t see a difference, to me they’re just health care professionals so I don’t know the difference between a nurse and a physician is because they’re both there to help you with medical problems.” Participants did not perceive a hierarchy within the team but some suggested adding a nutritionist and alternative medicine specialists, such as acupuncture and osteopathy.
Better Collaboration: “They Are All Together”
Participants appreciated the advantages of having all clinicians work together, noting benefits such as input from different providers and alternative solutions when needed. Heather remarked: “It was nice to have everybody's input … So, for me that was very helpful. And if you have any questions, you have more than one person there to answer them, you know.” For example, Rachel described what she appreciated about the program: “What I liked, I think I said it the last time, … , it's that they’re all together.” Charles even stressed the financial aspect of having all the care providers in the same location and that this arrangement avoided unnecessary costs for patients: “Perhaps it's better to have several at the same place … because in reality it costs nothing. When you go to [different] places, there's no improvement but it costs me hundreds of dollars.”
Grasping the Pain Issue: “They Helped”
Almost all participants felt that they were “helped” to better understand their condition, to learn what to do or not to do, or to “see light again.” There are various ways to analyze the participants’ use of “help.” (i) Some participants had already accepted their condition before joining the program and sought help to better manage their pain. For example, Stella stated that “I would like something that would … not cure it [LBP], but that I’m able to cope with it. You have to learn to cope with something. And I think a lot of things is right here” (Stella). (ii) Some participants were seeking help to understand their health problem. A participant expressed that in her account: “I appreciate them taking time out of their busy day to help me. They are all very nice, I really appreciate everything they were doing for me, they were able to answer pretty much any question I had to ask them. It did help quite a bit, and I would definitely refer, if anybody else had any problems, to come here” (Helena). (iii) Some participants sought people who would listen to them. Valerie shared this perspective: “In fact, it's just knowing that you are being followed, that you can talk to someone if things aren’t going well, that's like 50% of the cure right there because if I hadn’t had those people, as I said 2 or 3 times, I don’t know where I’d be.”
Care Was Responsive to Needs and Experience: “Always Centered on Me, Not General”
Participants praised the personalized approach of the IDT program, describing several meaningful facets: being listened to and understood, being asked relevant and individualized questions, and being treated kindly, with politeness and attentiveness. Helena noted: “They were all very nice to me and answered all my questions and everything.” Stella described the individualized approach: “I felt that from A to Z, I had very good, personalized care.” Samuel echoed: “I never felt as if we were in a general situation … ; I mean I always felt as if we were talking about me, that we found explanations, solutions, things improved … In all the interventions I felt as if it was always centered on me, not general.”
Participants also highlighted the completeness of care, the team taking sufficient time and not acting hurried, and how IDT care decreased feelings of isolation. Debra stated: “The difference (with usual care) I know is like I'm not alone to fight my problem. That's the first difference.” Some participants described IDT as unique. Heather stated: “You can’t compare the difference” between unidisciplinary (physician only) and IDT care. Rachel summed up her experience: “I mean the family doctor, it's not that he wasn’t good but he wasn’t a back specialist … I recommend it to everyone who has back pain: ‘Go to the [interdisciplinary] clinic’.” One participant expressed a negative experience of being seen during a follow-up visit with another patient in the room: “It's just the whole situation with bringing another patient in with the physician, like I would prefer that not to happen in my case. I wasn’t told ahead of time that it was going to happen. So, I would have preferred they ask me if I was comfortable with something like that first. Then I would have honestly said I would much prefer if it was just one-on-one” (Helena). This account underscores the importance of patient preference in person-centered care.
Meanings of Recovery: “I’m Able to Function”
Most participants viewed recovery as regaining function and managing pain rather than total pain mitigation. They described recovery in terms of performing daily activities and experiencing less pain. Valerie shared: “I’m able to function; which wasn’t the case when I got here; I really didn’t function, I had zero functioning. Now I think that I function at least 60%; that's a lot.” Rita expressed a similar sentiment: “It's fantastic. You see, I feel a bit like crying when I say that because before and after … oh my God … I used to be very active before. When I fell, I had difficulty moving, what's happening to me … Then having the tools, understanding my body, functioning … For me, it's marvelous.”
Some participants, particularly older ones, seemed to have accepted their pain and sought ways to better live with it. Stella stated: “You know, something that's totally worn can’t be cured. It can be calmed, but not cured. It can improve, by exercise, by walking more, by just training. Wear and tear.” Others reached this conclusion through interactions with IDT members. Valerie noted: “They taught me to manage this pain, that's the most important thing, to manage it and live with it.”
Discussion
The findings from this study contribute to the growing body of knowledge on the benefits of team-based care for managing chronic conditions, particularly LBP. They also revealed the meaning of recovery in this inquiry where the use of phenomenological approach enhanced the exploration of the subjectivity of human experience with living with chronic pain and IDT care. Among the participants, those who accepted their condition before joining the IDT program were mostly looking for help to learn how to live better with their pain. These participants tended to be older and have had lived with their pain for a longer time. In contrast, the participants who were younger or with a shorter pain duration, sought to gain understanding of the cause of the pain and to be relieved from it.
While a team-based approach is recommended by pain treatment guidelines, the optimal composition or content of interdisciplinary care remains unclear.8,62,63 The composition of the primary care IDT with a nurse, physician, physiotherapist, and psychologist seemed adequate for several participants; only 2 suggested adding a nutritionist and alternative medicine specialists. However, participants appreciated the roles and importance of different clinicians differently, with some desiring flexibility in clinician involvement. Being treated by an IDT composed of several healthcare members is relatively infrequent in the context of ambulatory and chronic disease management settings in Canada and other high-income countries.20,64,65
A singular finding from this inquiry is the intimidating aspect of the first IDT evaluation, similar to experiences in hospital ward rounds of health professionals and residents. 66 Providing information to patients before their first visit about the program, team members, and their roles could help reduce uncertainty and anxiety.67,68 Tools like animated videos, interactive quizzes, or leaflets on IDT care and team roles might be helpful. The presence of all team members at the initial evaluation is warranted to help patients mitigate this feeling and better understand the roles of different professionals.
The participants in our study suggested that there were advantages of IDT care. Having all the care providers in the same location prevented the participants from needing to start over and over to tell their story to each of the clinicians. Participants also saw IDT as an opportunity to be heard and IDT appears to fulfill this need with the combined contributions of a group of health care professionals (synergistic effect). The desire to be heard was so intense for some participants that sometimes the interviewer was thanked for his time during the interview as if he was part of the care team. This aspect of listening has been highlighted by several authors particularly with respect to alleviated suffering.69-72 Even IAPO calls on healthcare stakeholders to listen to and engage with patient populations affected by chronic pain. 73 By attempting to suspend and set aside preconceptions, clinicians can better understand and appreciate the world of illness inhabited by their patients. 71
Participants also saw IDT as very responsive to their needs and personalized in its approach. This is consistent with the conclusion from Foster et al that “Patients viewed the combined contributions of a GP [general practitioner] and other health professionals in team care as thorough and reassuring.” 74 This finding also supports many carative factors of Watson's theory of human caring.75,76 The importance of understanding the patient's lived experience is fundamental to PCC.75,77 Several elements of PCC 26 emerged from the participants’ accounts: the importance of respect for patients’ values, preferences and expressed needs; information, communication, and education; and emotional support. The findings seem to confirm the belief that team-based care is the primary and immediate healthcare setting where PCC occurs. 78
For most participants, recovery meant regaining function and managing pain, rather than total pain mitigation. They provided examples of functioning (eg, walking, moving, managing daily routines) that align well with the components of the International Classification of Functioning, Disability and health. 79 Similar findings were reported for individuals living with myalgic encephalomyelitis and chronic fatigue. 80 For Zhong Hui, the process of recovery begins with self-cultivation (learning about one's condition and taking steps to improve it). 81 In this sense, IDT care helped the participants to better understand their condition. The IDT program appeared to be facilitating, for some participants, response shifts in their expectations from seeking cure to learning to cope with their pain condition. Response shift is defined as a change in the meaning of one's self-evaluation in terms of values, standards of measurement, or redefinition of constructs. 82
Finally, our assumption that the particular patient–physician relationship may constitute a barrier to IDT care was not supported by our participants’ accounts. The traditional paradigm of medical care has been based on a dyad of one doctor and one patient. This construction, and associated expectations of clinicians and health professionals, however, does not seem to have been an impediment to an IDT care approach for our participants. Possible implications for IDT programs, based on our findings and conclusions, are summarized in Table 4. Clinical practice should assess patients’ readiness for IDT care, reduce anxiety through clear previsit information, and offer flexible follow-up tailored to patient needs. Emphasizing person-centered care and incorporating functional status alongside pain assessments are essential to improving outcomes for individuals with LBP.
Implications for IDT Programs.
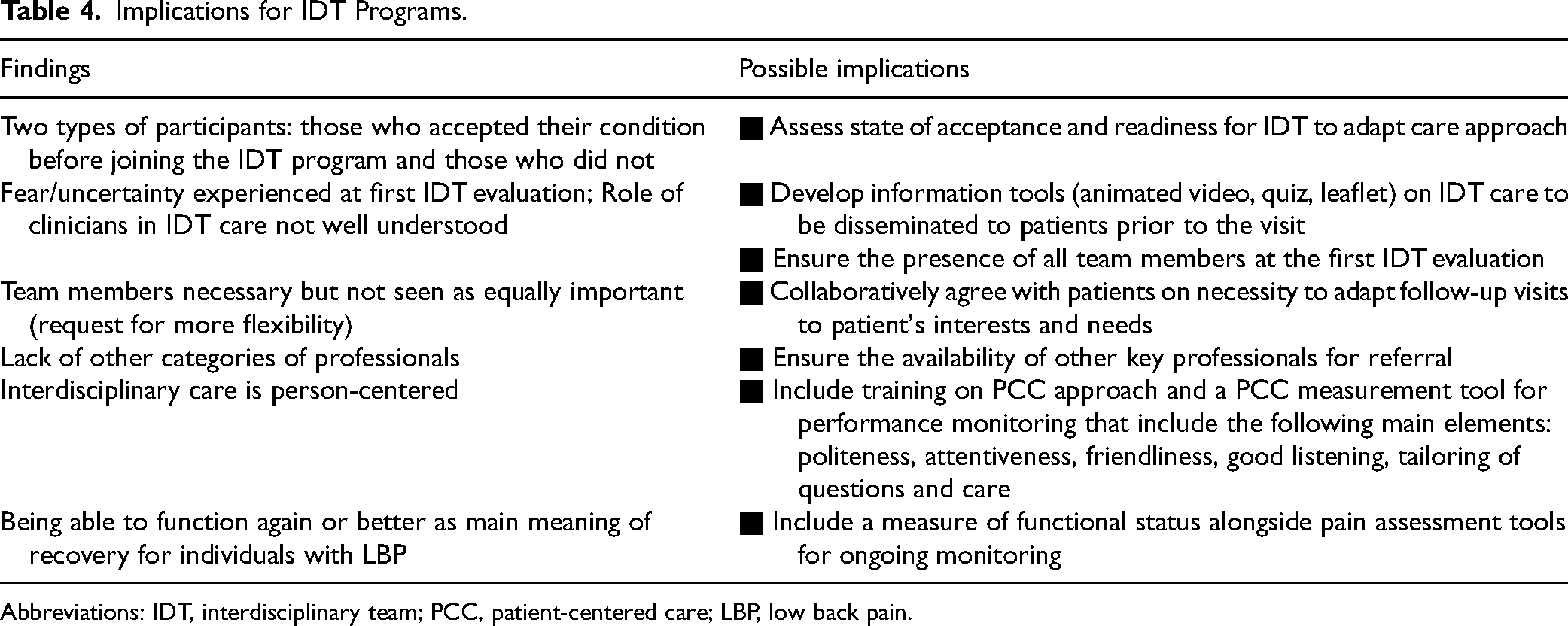
Abbreviations: IDT, interdisciplinary team; PCC, patient-centered care; LBP, low back pain.
Limitations
Participants in this inquiry only included individuals who remained in the IDT program. Due to practical reasons, all but 4 interviews were conducted at the clinics. However, we used dedicated rooms to conduct the interviews in and we can confirm that there was an environment of trust between the participants and the research team. We were not able to conduct interviews with people who withdrew from the IDT program. Among those participants who withdrew, some might not have felt ready or been interested to participate actively in a self-management oriented program, or were expecting a program that offered a ready-made solution by the team to rid them of their pain. As documented in the literature,83,84 sex and gender affect pain perception, pain coping, pain reporting, and pain-related behaviors. Although 9 of the participants were female, we did not explore the impact of sex on the findings, and we did not collect gender specific information. As pointed out by van Manen, “it should be acknowledged that phenomenological research is always incomplete and tentative because the researcher cannot possibly capture a given experience in its entirety nor describe how all people will experience a particular event.” 85
Conclusion
This inquiry to explore patients’ experiences while participating within an interdisciplinary care team is part of an integrated and interdisciplinary primary care program for the prevention and the management of LBP. Consequently, the findings may assist clinicians to understand patients’ perspectives and help improve the process of care; to inform the design and implementation of IDT programs, and to devise patient and interprofessional education programs on team-based care. Integrating constructs and concerns that are important to patients is essential for efforts to improve the delivery of care and patient health outcomes.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735241311752 - Supplemental material for Patients’ Experiences Participating Within an Interdisciplinary Primary Care Program for Low Back Pain
Supplemental material, sj-docx-1-jpx-10.1177_23743735241311752 for Patients’ Experiences Participating Within an Interdisciplinary Primary Care Program for Low Back Pain by Amédé Gogovor, Matthew Hunt, Richard Hovey and Sara Ahmed in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735241311752 - Supplemental material for Patients’ Experiences Participating Within an Interdisciplinary Primary Care Program for Low Back Pain
Supplemental material, sj-docx-2-jpx-10.1177_23743735241311752 for Patients’ Experiences Participating Within an Interdisciplinary Primary Care Program for Low Back Pain by Amédé Gogovor, Matthew Hunt, Richard Hovey and Sara Ahmed in Journal of Patient Experience
Supplemental Material
sj-docx-3-jpx-10.1177_23743735241311752 - Supplemental material for Patients’ Experiences Participating Within an Interdisciplinary Primary Care Program for Low Back Pain
Supplemental material, sj-docx-3-jpx-10.1177_23743735241311752 for Patients’ Experiences Participating Within an Interdisciplinary Primary Care Program for Low Back Pain by Amédé Gogovor, Matthew Hunt, Richard Hovey and Sara Ahmed in Journal of Patient Experience
Footnotes
Acknowledgments
The authors would like to thank the participants who contributed to this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Research Ethics Board of the McGill University Health Centre (#MPCUSM-12-220 GEN).
Funding
The interdisciplinary primary care program was supported by the Fonds Pfizer-FRQS-MSSS sur les maladies chroniques. AG was supported by an FRQS doctoral award.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Research Ethics Board of the McGill University Health Centre (#MPCUSM-12-220 GEN) approved protocols.
Statement of Informed Consent
Written informed consent was obtained from the participants at their first visit at the start of the program for anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.