
Abstract
Given the complexities of healthcare provision, it is imperative to understand how single adults experience their interactions with medical professionals and health care organizations, manage care and treatment, and navigate the barriers encountered. This study's purpose is to understand physical and mental health experiences in consideration of social determinants of health, barriers, and coping strategies for single adults diagnosed with COVID-19. An interpretive phenomenology study design was used with 12 individuals who were single and living alone during the COVID-19 pandemic. Semi-structured, open-ended interviews revealed important aspects of the COVID-19 illness experience. Interviews were transcribed for coding and thematic analysis. Analysis of patient interview data identified 4 themes: Dealing with Isolation, Dying Alone, Managing Stigma, and Making a Support Plan. The findings offer insight into what it means to have COVID-19 for single adults who live alone. These findings can be used to help improve the illness experiences of those with COVID-19 and other serious or complex conditions.
Key Points
It is imperative to understand how single adults living alone manage care and treatment during illness.
This study's purpose is to understand physical and mental health experiences in consideration of social determinants of health, barriers, and coping strategies for single adults, living alone, who were diagnosed with COVID-19.
Analysis of patient interview data identified 4 themes: Dealing with Isolation, Dying Alone, Managing Stigma, and Making a Support Plan.
The findings of this qualitative study can be used to help improve the illness experiences of single adults living alone with COVID-19.
Introduction
According to the United States Census, an ever-greater proportion of the population is single or un-partnered, less likely to live near family, or maintain multi-generational households.1,2 These demographic changes mean that during illness, single adults may have few resources available for social support. It has been hypothesized that because of social support, married individuals live longer and have fewer complications of disease.3–5 Conversely, single people experience diminished health on several measures including self-reported health, mobility limitations, depression, and lowered life expectancy.3–5 In serious or complex chronic conditions such as cardiovascular disease or cancer, social support has been shown to affect self-management behaviors and improve self-efficacy.6–8
In December 2019, reports of a new respiratory illness surfaced. By March 2020, the COVID-19 virus had spread to 114 countries and was declared a pandemic by the World Health Organization. 9 In subsequent months, COVID-19 proved to be one of the most contagious and deadly viruses in human history. What followed could best be described as social upheaval, with negative effects on individuals, communities, culture, and economies10,11
Beginning in June 2020, guidance for individuals with suspected or confirmed COVID-19 included isolation in the home without visitors for a minimum of 10 days after onset of symptoms, plus at least 3 more days once symptoms disappeared. 12 Later, the recommendation was reduced to 5 days of isolation unless symptomatic. 13 Social distancing measures and lockdowns restricted travel, leisure activities, and limited social activities, leading to disruption of community life. Although social isolation measures seemed necessary to halt the spread of the disease, health scholars voiced concerns about the unintended effects of social isolation. 14
Yang et al 15 found that individuals who reported less social support or those who were single were more likely to report higher psychological stress early in the COVID-19 pandemic. Loneliness and social isolation during the pandemic were found to be risk factors for psychiatric disorders including depression, especially in older patients. 16 Younger adults were also at risk for loneliness and depression during the COVID-19 pandemic particularly when they perceived a lack of social support. 17
Social determinants of health are non-medical factors that influence health outcomes. Greater understanding of the impacts of single adult status together with other social determinants of health is needed. 18 Compounding the obstacles to health communication, health literacy, successful treatment, and self-care, are systemic biases associated with age, life experiences, sexual preferences, social class, gender, and race/ethnicity.19–21 Thus, our research fills an important gap, given the significant health disparities associated with COVID-19, the implications of facing COVID-19 with limited support, and the paucity of research focusing on single adults who lived alone and contracted COVID-19. Understanding their experiences could help us better prepare for future outbreaks of infectious diseases, especially those requiring isolation. Additionally, our research could be used to enhance adaptability and coping strategies to promote well-being in single adults living alone.
Methods
Design
This study incorporated an interpretive phenomenology research design to explore the physical and mental health experiences and concerns for single adults living alone who had been diagnosed with COVID-19. The design was chosen to explore their experiences in a natural environment. Interpretive phenomenology helps gain understanding of a phenomenon that is not well understood with the central focus on the lived experience of individuals in the world of everyday life.22–24 The lived experiences give meaning to an individual's perception of a phenomenon. Considering the purpose of the study and lack of literature exploring the physical and mental health experiences of single adults with COVID-19 living alone, an interpretive phenomenological method was used.
Participants
The study took place in the southern United States, a region that ranked comparatively low for COVID-19 vaccination rates. 25 A convenience sample of participants was recruited by word-of-mouth, a university listserv and email, and flyers posted in community areas. Further participants were identified by a snowball sampling technique. Participants were invited to participate if they were at least 18 years of age, had a confirmed case of COVID-19 per self-report, and lived alone. Exclusion criteria included those not aged 18 years, not living alone, or not having COVID-19. A total of 12 participants contacted the research team about participation and were recruited. No further interviews were conducted once thematic saturation was achieved, and no new themes emerged during data collection and analysis.
Data Collection and Analysis
Ethical approval to conduct the study was obtained from the researchers’ university Institutional Review Board (approval code IRB-FY22-16). After verifying eligibility conditions and all criteria for informed consent were read and explained to the participant, verbal informed consent from each participant was obtained as a recording before data collection began. Individual, semi-structured, open-ended interviews were conducted in person or remotely on Microsoft Teams, per participant's preference. Each interview location was mutually agreed upon by the researcher and participant. Eight of the participants opted to be interviewed via Teams and the others chose face-to-face venues.
Using a semi-structured interview guide with a predetermined set of questions, interviews began with broad questions designed to elicit the participant's understanding of the problems faced with the diagnosis. For example, a participant would first be asked to tell the researcher about their experiences with COVID-19. Further questions were asked about their perception in terms of what went well and what did not go well during the diagnostic process, health care encounters, course of the disease, and thereafter. Subsequent questions were directed to enhance and clarify the narrative description of the COVID-19 illness experience. Interviews were face-to-face or via Microsoft Teams, audio-recorded, and lasted approximately 75 min. Interviews took place in April and May 2022, on average,18 months after COVID-19 diagnosis.
All interviews were audio-recorded and transcribed verbatim. Results of this participation were de-identified, kept confidential, and maintained by the researchers in a password-protected location. The participants received a $25 gift card incentive after the interview. Transcriptions were made for coding and thematic analysis.
To enhance credibility and trustworthiness of the interpretations, methodological strategies were used. A team approach was used to analyze data as identified by Guba. 23 The team included 3 doctoral educators in nursing and sociology with experience in qualitative analysis to ensure credibility through peer-checking. Data collection and interpretation occurred at the same time. The team met regularly to analyze and discuss the interpretations of each transcript and transcripts as a whole, to immerse themselves in the data and to allow new insights to emerge. An inductive approach was used during data analysis in which coding of the transcripts was guided by the data's content instead of preconceived theoretical perspectives. 24 Qualitative data were organized by line-by-line coding of each transcript, and themes were then identified according to this study's purpose. During the analysis of the final interview, no new codes or themes were identified ensuring data saturation. The research team analyzed the transcripts and reached agreement among interpretation of data and themes. Triangulation among researchers helped to enhance trustworthiness of the findings. 24
Results
A total of 12 participants completed the study. Demographic characteristics including age, gender, ethnicity, education, and relationship status, are described in Table 1. All participants lived alone at the time of their COVID-19 diagnosis. Primary physical symptoms included exhaustion, weakness, fatigue, and loss of taste and smell (Table 2). One participant required hospitalization for severe weakness and dehydration. Many participants experienced fear, anxiety, and concerns for their own health and the health of others who might have been exposed. Diagnostic testing was obtained through drive-up testing centers, doctor's offices, clinics, and using at-home testing kits. One participant was not tested until hospitalization. Another was asymptomatic, but was tested so they could join their family for Christmas. They tested positive for COVID, delaying holiday plans.
Sociodemographic Characteristics of Participants.

COVID-19 Symptoms with Quotes from Participants.

Navigating the diagnostic system was challenging for some due to lack of available appointments, while others had difficulties obtaining at-home test kits. One participant attempted to walk into a drive-up testing facility but was turned away until they could obtain vehicular transportation. Nine of the adults in the study were diagnosed with COVID-19 prior to vaccine availability (75%) and 3 contracted COVID-19 after vaccination availability (25%). Two of these individuals had been vaccinated prior to getting COVID-19. Of the participants, 3 had COVID-19 more than once.
Participants’ coping strategies included allowing themselves to rest when needed, watching television, playing video games, reaching out to others, and as allowed, getting fresh air. In addition to information on physical and emotional symptoms and coping strategies, several themes emerged from the interviews: Dealing with Isolation, Dying Alone, Managing Stigma, and Making a Support Plan. In Table 3, examples of quotes are described for each theme.
Themes and Examples Quotes from Participants.
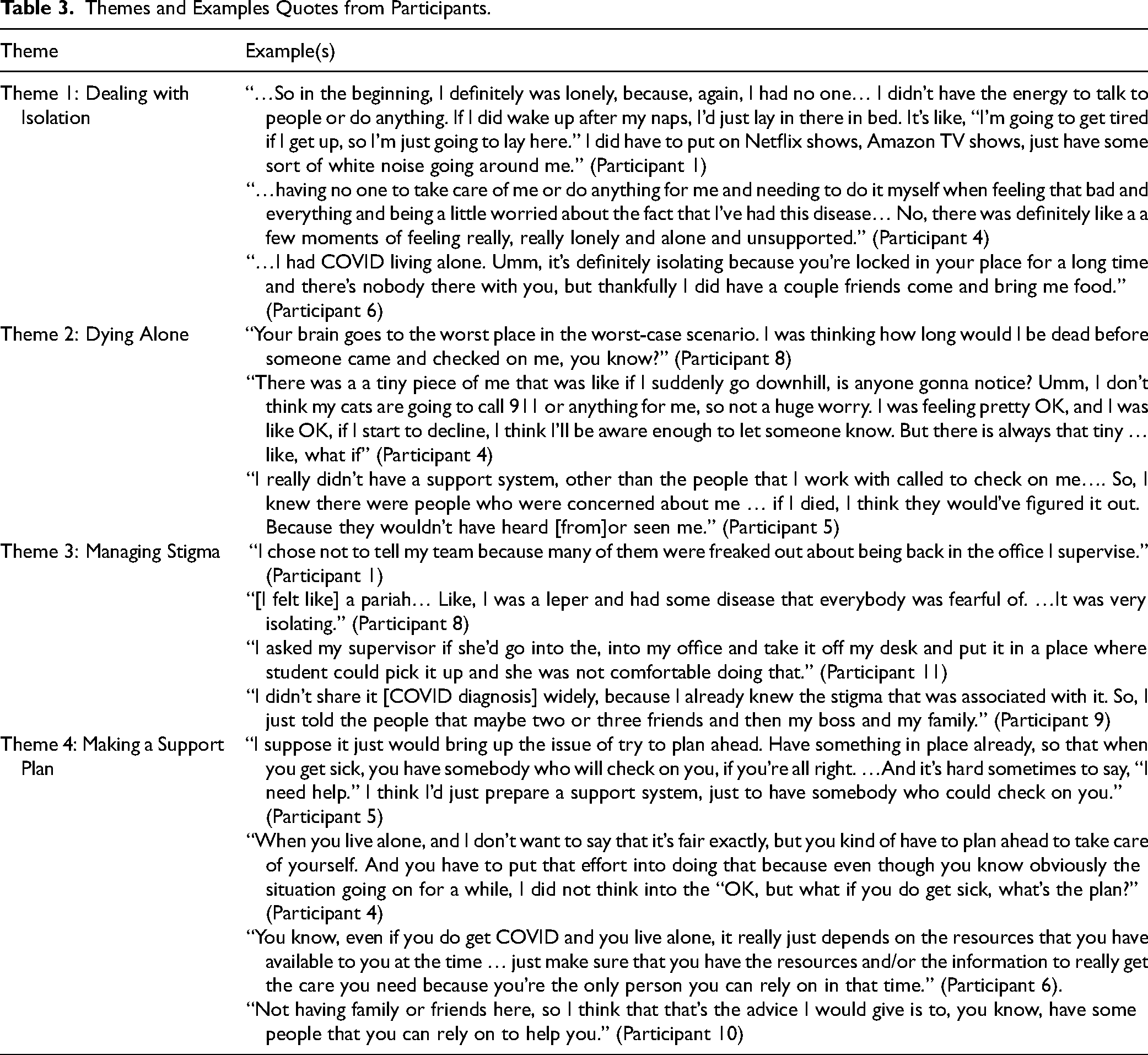
Theme 1: Dealing with Isolation
Many of the single adults in the study did not have family members living nearby. Most had little or no access to physical support or hands-on caregiving during the illness. As a result, they often sought the help of neighbors, friends, romantic partners, and delivery services to obtain food, medicine, and other supplies. Likewise, the single adults in our study had no close face-to-face social contact with other people while they had COVID-19, leading to feelings of loneliness and isolation, and putting them at risk for negative health outcomes. Communication with others came from texting, phone calls, and internet communication platforms. For some, pets helped them deal with being sick and alone. Paradoxically, some participants reasoned that having COVID-19 while living alone could be an unexpected benefit. The advantages included being able to self-manage their illness and recover on their own timetable without the fear of passing the virus to others.
Theme 2: Dying Alone
The fear of dying alone was expressed by many of the participants, particularly those individuals who had few or no family members nearby or had contracted COVID-19 prior to vaccine availability. During the early days of the epidemic, media reports often stressed how suddenly COVID-19 could turn from mild to serious. Participants often expressed fear or concern that their COVID-19 symptoms could worsen and that perhaps they would die alone, only to be discovered later. Most admitted that this was the kind of negative thinking they tried to avoid, but that sometimes the fears resurfaced, especially when they encountered negative media reports or when their symptoms worsened.
Theme 3: Managing Stigma
Most participants experienced stigma throughout their illness, including when communicating the news of their diagnosis to others and upon return to work and social activities. For many, the stigma of having COVID-19 was intensified because they were single and had no one living with them. Some were hesitant to let others know that they had COVID-19. Others found that returning to daily activities after the quarantine period was unexpectedly difficult as reintegrating back into social and work-related activities was met with stigma. Some internalized feelings of self-blame and guilt for contracting the disease as if they should have been able to prevent it. Many worried about potentially passing COVID-19 to others before they found out they had it.
Theme 4: Making a Support Plan
Once participants in our study first realized they had COVID-19, they had to find ways to get the physical and emotional support they needed. Drawing on their own experiences, most suggested making a support plan to cope with illness before becoming ill. Several of the participants described how they had to venture out on their own despite feeling ill because they had run out of supplies. Participants cautioned against doing this because they had put themselves and others in harm's way. In one case, the participant drove to a shopping center to pick up groceries and collapsed in the parking lot, resulting in hospitalization. Participants advised others to make sure they had enough food, over-the-counter medications, and fluids. They recommended reaching out to others for social support early and often throughout the illness period. Participants advised others to make sure there was someone in their social networks, whether it be family, friend, or work colleague, who would periodically check on them.
Discussion
This study fills an important gap by providing an understanding of the experiences of single adults living alone with COVID-19. Their stories revealed unique concerns and coping strategies. The themes that emerged were Dealing with Isolation, Dying Alone, Managing Stigma, and Making a Support Plan. Consistent with other studies,26,27 participants in our sample expressed fear and psychological distress about dying from COVID-19; however, rather than just the fear of dying, they reported that their distress was increased because nobody was with them to know if their condition worsened or if they had died. This supports the findings of Yang et al 15 that lack of social support during the pandemic was more likely to cause higher psychological stress.
A surprising finding was that some participants thought that being alone with COVID-19 was better because it reduced the chance of spreading the virus to family or friends. This supports the findings from Sloan et al 26 that during the pandemic, people displayed altruistic fear, which is fear about significant others contracting the virus. This finding adds an additional dimension to findings that loneliness and social isolation during the pandemic have been found to be risk factors for psychiatric disorders.16,17
Many studies document widespread stigma associated with COVID-19.10,11 Likewise, participants in this study experienced various forms of stigma, which they felt intensified their isolation and loneliness. While stigma was a common phenomenon experienced by those with COVID-19 whether living alone or with a partner, this finding among study participants is important because those who live alone have a significantly higher incidence of psychiatric disorders.28–30 Participants also reported feelings of shame and guilt likely resulting from internalization of social stigma. This finding was not unique to those living alone.26,28 Participants reported various strategies for dealing with loneliness. Planning for social and physical support during illness was a coping mechanism identified by participants.
Studies have reported social support as an essential coping strategy in stressful situations.26,30 While all participants in this study had access to communication with others via texting, phone calls, and video communication platforms, some reported that they lacked the energy to communicate with family and friends.
Implications
This study highlights unique challenges for people who live alone. Our research suggests that there is a need for health systems to consider forms of support for patients who live alone during a public health emergency that requires isolation. Social isolation has been associated with a substantial increase in risk of premature mortality from all causes. 30 Additionally, research indicates that social isolation and loneliness are strongly associated with an increased incidence of psychological issues such as depression, anxiety, and suicidal ideation. 31 Health care providers should not assume everyone has family and significant others available for social and physical support.
When recommending isolation or quarantine, health care providers should assess patients for support. The potential problems associated with social isolation should be discussed and interventions should be recommended. There is a need for policy makers to consider added resources for people living alone in the case of a public health emergency that requires home isolation to curb disease spread.
Limitations and Future Directions
Limitations of this study include a small, homogenous sample. Most participants had some college education, which could positively affect their ability to make informed health care decisions. Although we did not ask about income and wealth, we recognize that education is linked to access to financial resources. Therefore, the transferability of our findings to less privileged groups is limited. This limitation highlights the need for future research to better understand the experiences for those with less education and affluence. The study was conducted in the southern United States, where vaccination rates tended to be low. 25 Future research might include other parts of the United States for comparison.
This study included single adults who were living alone and did not exclude those who had been divorced or widowed. We recognize that age and prior marital status could affect the experience of living alone with COVID. Future research might examine these groups separately to show commonalities and disparities between their experiences. Most of the participants contracted COVID-19 before vaccines were available to them, which might have contributed to their anxiety about having the illness while living alone. Those who initially contracted COVID-19 after being vaccinated tended to have less severe symptoms. Regardless of limitations, the findings have important implications for healthcare providers who care for single adults with COVID-19 who live alone.
Conclusion
In summary, our research offers insight into what it means to have COVID-19 for single adults who live alone and the associated risks for loneliness and social isolation. Participants sought social support by reaching out to others through telephone calls, facetime, texts, and other forms of electronic communication. Because they were single and living alone at the time of their COVID-19 diagnosis, they had to rely on people outside of their home for supplies, food, and medicine. As relatively well-educated individuals they had the financial resources and personal networks to aid in this goal. Many experienced a stigma associated with the illness and some were reluctant to disclose. Looking back on their experiences, all were able to offer advice to others who might find themselves in similar situations. Thus, we believe these findings add to our knowledge of the social determinants of health and can be used to help improve the illness experiences of those with COVID-19 and other health conditions.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735241302742 - Supplemental material for COVID for One: Identifying Obstacles to Self-Management of COVID-19 for Single Adults
Supplemental material, sj-docx-1-jpx-10.1177_23743735241302742 for COVID for One: Identifying Obstacles to Self-Management of COVID-19 for Single Adults by Linda Treiber, Christie Emerson and Jenna Shackleford in Journal of Patient Experience
Footnotes
Acknowledgments
We gratefully acknowledge the adults who participated in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Radow College of Humanities and Social Sciences, Kennesaw State University.
Ethical Approval
Ethical approval to report this case was obtained from Kennesaw State University Institutional Review Board (IRB-FY22-16).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Kennesaw State University Institutional Review Board (RB-FY22-16) approved protocols.
Statement of Informed Consent
Verbal informed consent was obtained from the participant(s) for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.