
Abstract
Aim
The COVID-19 pandemic has seen hospitals isolating suspect cases. Geriatric populations are at a risk of severe COVID-19 disease and often present with concomitant geriatric syndromes requiring holistic interdisciplinary care. However, isolation of older people poses challenges to care delivery. This study shares the experience of Singapore’s first acute geriatric isolation facility geriatric PARI (Pneumonia-Acute Respiratory Infection) ward and describes the geriatric-related outcomes and pitfalls in care delivery.
Methods
This is a retrospective cross-sectional study performed in 7 negative pressure isolation rooms in an acute care public hospital in Singapore. 100 patients admitted consecutively to the geriatric PARI ward were included. Patient demographics, presenting symptoms and geriatric-related adverse outcomes associated with hospitalisation were collected and analysed.
Results
Patients’ mean age was 86.4 years (standard deviation
Conclusions
The geriatric PARI ward is essential for curbing nosocomial transmission of COVID-19. This is important in the older people with comorbidities who are more likely to develop morbidity and mortality. Our study reveals challenges in delivering person-centred care to the older patients in isolation rooms, especially in the management of delirium and falls prevention. Innovative strategies should be developed to minimise isolation-related adverse outcome.
Introduction
In light of the COVID-19 pandemic caused by the novel SARS-CoV-2 virus, public health agencies worldwide have adapted directives such as self-isolation and social distancing to limit interaction within communities to control the spread of the disease. In hospitals, early isolation of patients with acute respiratory infections or pneumonia has been implemented to reduce the likelihood of nosocomial transmission of the SARS-CoV-2 virus, as it has similar clinical manifestations as the common respiratory viruses.1,2 This is exemplified in a case report in a tertiary hospital in Singapore whereby a patient who presented late with respiratory symptoms after admission was eventually diagnosed with COVID-19 infection, exposing multiple patients and healthcare workers. 3 A respiratory surveillance ward has since been successfully implemented in a tertiary hospital as a strategy to reduce nosocomial transmission of COVID-19 in Singapore. 1 Furthermore, there is substantial concern with regards to frail older patients presenting atypically, with features such as delirium, abdominal pain and low-grade fever instead of respiratory symptoms.4,5
Older patients with COVID-19 are associated with higher mortality; especially for those with comorbidities such as hypertension, cardiovascular disease, diabetes, chronic respiratory disease and renal disease. 6 In Singapore, all nursing home patients with respiratory symptoms are isolated and tested for the SARS-CoV-2 virus so as to prevent the risk of nosocomial transmission in the nursing home. 7 Therefore, it may be logical to over-screen older patients for the novel SARS-CoV-2 virus rather than to miss out on them, potentially leading to catastrophic outcomes.
Previous study has patient-reported anxiety, fear and loneliness as a result of staying in isolation care units. 8 While current literature is lacking in terms of the impact on elderly patients in geriatric isolation facility, one has to be mindful that older patients often present with syndromes such as immobility, impaired cognition, postural instability and incontinence. Failing to address the above geriatric giants during admission may result in adverse clinical outcomes, and add further strain to hospital resources from iatrogenicity and prolonged hospitalisation.9,10 Strict isolation protocols, restriction of family visitation and reduced physical contact with healthcare staff result in a difficult care environment for the vulnerable older patients. 7 This hinders the delivery of holistic care for these older patients.
This conundrum of isolating and treating older patients in such facilities therefore needs meticulous planning and execution.
This cross-sectional study serves to share our experience in the implementation of Singapore’s first acute geriatric-respiratory isolation facility, also termed as the geriatric PARI (Pneumonia-Acute Respiratory Infection) ward, as well as describe the patient clinical profiles and geriatric-related adverse outcomes.
Material and Methods
Purpose of Study
This is a cross-sectional study investigating the challenges experienced in managing older patient in the acute geriatric-respiratory isolation facility. Geriatric-related adverse outcomes including inpatient falls, acute urinary retention and use of intravenous hydration were obtained.
Isolation Facility
The acute geriatric PARI ward comprises seven single-bedded isolation rooms with double automatic doors whereby only one door can open at a time to maintain negative pressure, situated in Changi General Hospital (CGH), a public tertiary hospital in the eastern region of Singapore. There is a toilet with grab bars in every room, but no window. Real-time camera monitoring is employed from the nursing counter. Three nurses are based in the ward per shift, with a full-time medical officer and a consultant geriatrician providing medical care.
Selection and Transfer Out Criteria
Patients who were above 65 years of age and presented with either clinical or radiological signs of pneumonia or acute respiratory symptoms were eligible for admission to this surveillance unit. 100 consecutive patients were recruited from 2 March to 14 April 2020. The patients could be admitted directly from the emergency department or transferred from the general ward and ambulatory specialist clinics. A total of two SARS-CoV-2 viral swabs were obtained 24 h apart, and patients were transferred out to geriatric acute care wards once both viral swabs were negative, in accordance to hospital policy. They lodged between 24–48 h in this isolation facility.
The SARS-CoV-2 viral swabs were performed via combined nose and throat swabs in universal transport media and then tested via an in-house laboratory-developed real-time PCR assay to detect the SARS-CoV-2 virus. The assay utilises two separate targets: one detects the N gene, and the second detects the ORF gene of the 2019-nCoV virus. 11
Patient Data Collected and Analysis
De-identified patients’ characteristics were collected from hospital electronic data. They included age, gender, place of residence, comorbidities, baseline function (Barthel Index), 12 Morse Falls Scale, 13 presenting complaints and geriatric syndromes (delirium [diagnosed based on DSM-V by geriatrician], 14 previously diagnosed dementia and behaviour and psychological symptoms of dementia (BPSD), falls history and bowel and urinary incontinence). The incidences of adverse outcomes such as mortality, inpatient fall, transfer to intensive care unit/high dependency ward, acute urinary retention and use of intravenous hydration were collected from the hospital electronic data. The SARS-CoV-2 viral swab results were also collected.
Univariable logistic regression was performed for the individual parameters. Odds ratios (OR) and its corresponding p-values were reported.
STATA version 14.0 (STATA Corporation, College Station, Texas) was used for statistical analysis.
Delirium and Fall Prevention Protocol
The nurse-driven hospital delirium protocol was enforced for all patients admitted with delirium. Established care bundles such as the Hospital Elderly Life Program (HELP) model have demonstrated great efficacy in preventing delirium and functional decline in hospitalised older patients.15 Our protocol includes assessing 4AT which is a rapid clinical test for delirium, 16 frequent orientation, monitoring for constipation and urine retention, scheduled toileting, early mobilization, sleep hygiene and pain assessment. This is implemented for both patients with delirium as well as dementia with BPSD.
A multifactorial intervention fall prevention protocol was implemented for patients with fall risk.17,18 This included a comprehensive fall assessment via a comprehensive fall history and detailed physical examination that includes functional mobility assessment tools such as short physical performance battery to elicit falls risk factors. All patients in the geriatric PARI ward had access to a multidisciplinary team of physiotherapists, occupational therapists, speech therapists and dieticians. Patients were also assessed for presence of osteoporosis and fracture risk.
Both the delirium and fall prevention protocols are established protocols that are currently used in the general geriatric ward.
Implementation of physical restraints should be avoided unless a patient is assessed to have high risk of self-harm 19 despite all measures taken. In our hospital, nurses have the autonomy to initiate physical restraints but require mandatory acknowledgement from the physician in charge, as well as from family members. Strict monitoring and regular review are also part of the hospital restraint policy.
Patient and Public Involvement
Patients or the public were not involved in the design conduct, reporting or dissemination plans of our research.
Results
Demographics and Comorbidities of Patients.

The mean premorbid 20-point Barthel Index was 8.6 (SD 7.4); the mean Morse Falls Scale was 42 (SD 27.8). The average length of acute hospitalisation was 12.2 days (SD 9.9), inclusive of the time spent in the PARI ward (Table 1).
The majority of patients admitted to the acute geriatric PARI ward had pre-existing comorbidities, of which the most common were that of hypertension (81%), hyperlipidaemia (74%) and renal disease (70%). About half of the patients admitted had cardiac disease. 35% of the patients had diabetes, and 17% had prior lung disease. 77% of the patients had ≥3 comorbidities (Table 1).
Presenting Symptoms, Geriatric Syndromes to the Geriatric PARI (Pneumonia-Acute Respiratory Infection) Ward. This Table Also Shows the Type of Interventions Rendered.
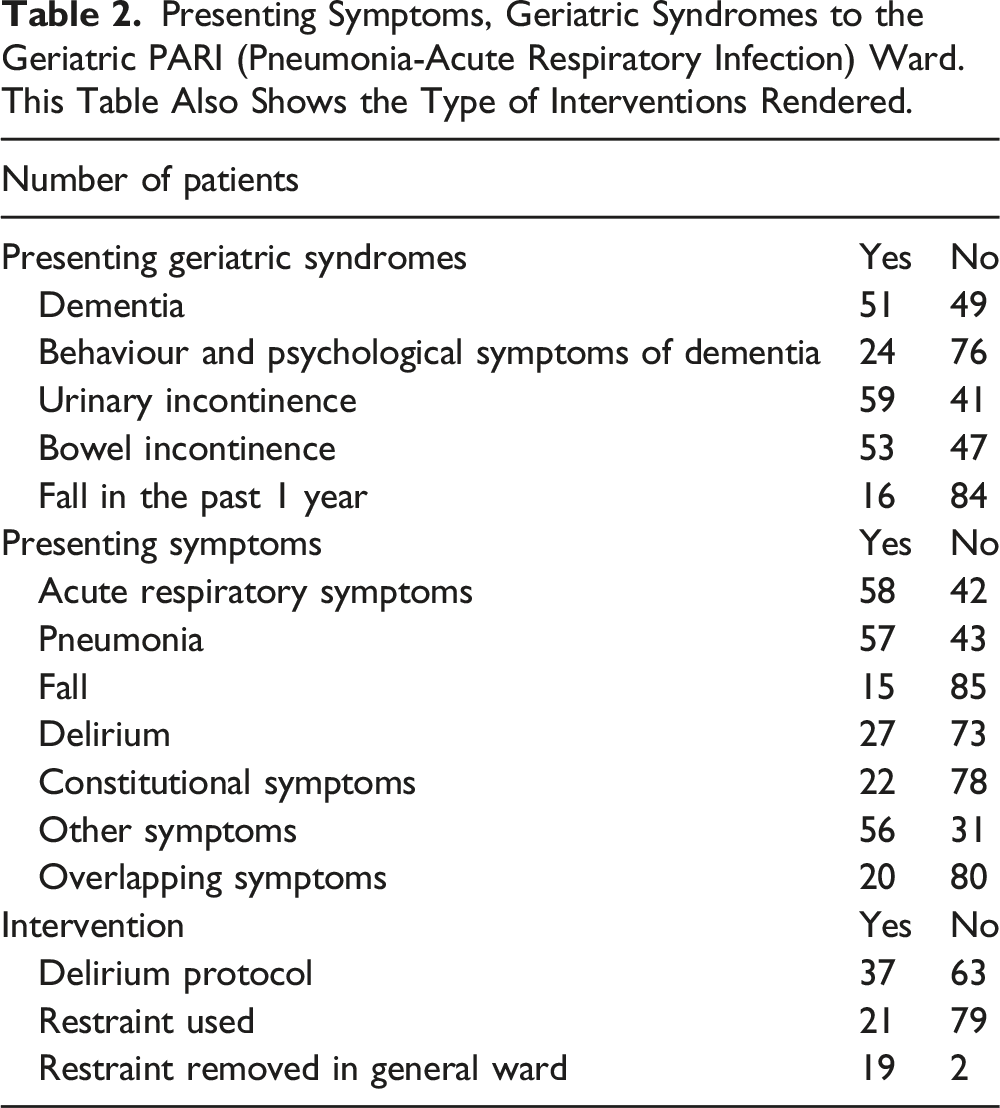
58% and 57% of patients admitted to the acute geriatric PARI ward presented with acute respiratory symptoms and pneumonia, respectively. About half of the patients presented with urinary and bowel incontinence. 15% of patients presented with a fall, and 27% presented with delirium. 22% of patients presented with non-specific constitutional symptoms such as lethargy and poor appetite. 56% of patients presented with other symptoms such as pain, dysuria, dysphagia, nausea, vomiting, giddiness, diarrhoea, constipation, stroke and gastrointestinal bleed. 20% of patients also presented with ≥1 overlapping non-respiratory symptoms (fall, delirium, constitutional symptoms and other atypical symptoms) (Table 2).
Univariable Analysis of Factors Associated with the Use of Physical Restraint.

Out of the 100 patients admitted, one patient tested positive for the SARS-CoV- 2 virus. In terms of adverse outcomes, there was one inpatient fall in the geriatric PARI ward, resulting in an overall fall rate of 1.64 per 1000 occupied bed days for the cumulative hospitalisation episode. 11 patients developed acute urinary retention, and 37% of patients were prescribed some form of intravenous hydration. The inpatient mortality rate was 14% (Figure 1). Shows the Adverse Outcomes of Patients and COVID Swab Results.
Discussion
Importance of Isolation Facility in Geriatrics Population During COVID-19 Pandemic
The mean age of patients admitted to the acute geriatric PARI ward was 86.4, of which a large proportion of the patients had significant comorbidities. The majority of our patients presented with ≥3 comorbidities. Many studies have since predicted severe disease and poorer outcomes in COVID- 19 patients with comorbidities.20,21 It is therefore imperative to isolate and screen older patients for COVID-19 to avoid delay in detection and treatment.
In addition, there was a notable number of referrals from nursing homes (13%) who were admitted to the acute geriatric PARI ward. Pro-active surveillance of nursing home patients with respiratory symptoms for the SARS-CoV-2 virus is important as any nosocomial spread within the nursing home would have grave consequences, 7 as nursing homes may not have developed capability for managing them on-site.
56% of patients presented with non-respiratory symptoms such as pain, dysuria, urinary incontinence, dysphagia and constipation on admission. Only slightly more than half of our patients presented with respiratory symptoms or pneumonia. In addition, 20% of our patients presented with overlapping symptoms, which made diagnosis and proper selection of older patients for this isolation facility challenging.
Amongst the 100 patients admitted to the geriatric PARI ward, one tested positive for the SARS-CoV-2 virus. This underlines the importance of early isolation and screening of high-risk older patients to render early treatment and prevent nosocomial transmission within the hospital.1,7 This low positive rate was likely attributable to the absence of widespread community transmission in Singapore at the time of this study. 22
Challenges to Patient-Centred Care Delivery in an Isolation Facility
Delirium and Dementia with Behaviour and Psychological Symptoms of Dementia
To our knowledge, there is currently no published study that investigates the effect of isolation facilities on the care of acutely ill older patients. There is a definite concern with regards to how care could be provided to older patients with geriatric syndromes in such facilities. 23 Existing studies have shown that 20–30% of COVID-19 patients develop delirium during the course of their hospitalisation, with rates of 60–70% in cases of severe illness at all ages.24,25 This is similar to our study for which 27% of our patients presented with delirium. Our study also showed that 51% of the patients admitted to the acute geriatric PARI ward had dementia of which 24% had BPSD. Out of the 27 patients who presented with delirium, 23 of them had underlying dementia. A total of 36 patients had the delirium protocol implemented as the hospital utilises the same protocol for both management of delirium and dementia with BPSD.
In addition, delirium can also be aggravated by the isolation environment and lack of physical and emotional contact with staff donning personal protective gears. Frequent transitions from the emergency department to the isolation ward and subsequently to the general ward may also exacerbate delirium. 26
In spite of the restrictive infection control measures, the principles of person-centred care for the older adult should be practised as much as possible. Evidence-based strategies in managing patient with delirium and dementia with BPSD include non-pharmacological measures as a cornerstone of care. These include frequent re-orientation, addressing pain, promoting sleep hygiene, maintaining regular bladder and bowel function, optimising oral intake, promoting sleep hygiene and early mobilisation. 27 However, our experience was that it was challenging to implement these non-pharmacological measures in the isolation facility.
Our study showed delirium as the main factor associated with physical restraint use (univariable odds ratio of 3.88; p-value 0.01). There were 21% of older patients restrained in the acute PARI ward. At present, there is no study available for head-to-head comparison of restraint use in isolation wards. Nonetheless, the frequency of physical restraint use in our acute geriatric PARI ward exceeded international-published studies of average of 4–13% in geriatric wards 28 and a local Singapore acute care ward of 8%. 29
This discordance is likely attributable to the sense of insecurity among the geriatric team regarding patient’s safety. 30 The isolation room which is operated by a single opened door at a time hinders the implementation of the delirium protocol. In addition, the extra time required to don personal protective equipment by the geriatric team further exacerbates the fear of not attending to the patient in time. Hence, it was not surprising for the geriatric team to prioritise patients’ safety, hence instituting physical restraints as a last resort. 30
A stark contrast could also be seen whereby 19 of the 21 restrained patients had their restraints removed once they transitioned to the geriatric care wards. Furthermore, none of the patients were given pharmacological treatment for delirium in our study.
Falls
16% of patients admitted to the geriatric PARI ward had a prior fall within the past 1 year, and 15% of patients had a fall as the presenting complaint. The mean Morse Fall Scale of 42 is close to the standard cutoff of 45 for fall risk. 31
Multifactorial interventions significantly reduce risk and rate of falling in hospitals. 31 With the implementation of the fall prevention protocol, one patient sustained a fall in the geriatric PARI ward which translated to an overall inpatient fall rate of 1.64 per 1000 occupied bed days for the cumulative inpatient stay of this group. This is much lower as compared to the published literature of 5.71–17.1 falls per 1000 bed days occupied in general wards. 17 However, this could also be contributed to the higher physical restraint used in our acute geriatric PARI ward.
It was notable that the patient who fell was the third patient admitted to this facility. This may have inevitably evoked a further sense of insecurity among the geriatric team to use physical restraints especially when staffing for acutely ill patients in this facility is stretched. 30
Existing meta-analysis has revealed that non-pharmacological interventions are effective in preventing falls. 32 However, such interventions have not been studied particularly in isolation settings. Many studies have also demonstrated the negative impact of physical restraints. 27 We believe that it is not the lack of knowledge or convenience that led to the use of physical restraints. 30 Prioritisation of patient safety, the fear of inpatient falls and physical limitations (double door rooms) are likely contributors to the use of physical restraints. This should be further explored via focus-group discussions with the geriatric team.
Acute Urinary Retention and Use of Intravenous Hydration
36% of patients were prescribed intravenous hydration. Besides definite medical indications for instituting intravenous hydration, we postulate that the limited accessibility to patients due to the isolation room setup may have also influenced clinical decisions to prescribe intravenous drips to avoid dehydration.
Similarly, 11% of patients developed urinary retention requiring catheterization during the short time spent in this ward, despite scheduled voiding and screening of post-void residual urine with bladder scans. Possible contributory factors include immobility and limited accessibility.
Moving Forward with the Pandemic
In this pandemic, one aspect of the care continuum involves restrictions and isolation measures to curb the spread of COVID-19. On the other side of the continuum, care of older patients emphasises person-centred care. In order to achieve both, a high staffing to patient ratio is required. The presence of a caregiver within the isolation facility could facilitate person-centred care for delirium, reduce falls risk and minimise restraint use. However, caregivers may be unnecessarily exposed to infected patients and require strict adherence to infection control protocols.
The availability of real-time camera monitors and bed sensors also helped nurses to monitor the well-being of the patients by detecting patient’s movements in and out of bed, hence enabling nurses to act swiftly. However, limitations include delayed response time, manpower required to monitor the screen and creation of a false sense of safety.
The use of visual stimulation could also serve as a distractor and keep patients occupied while in the isolation room. With technological advances, the use of tablets with video calling capability could be implemented so that older patients could communicate with their family to allay the fear of being in an isolation facility. Simulated presence therapy involving family has been successful in decreasing agitation in dementia and delirious patients in nursing home and hospital. 33 We could also implement other forms of non-pharmacological interventions such as music therapy, 34 light therapy 35 and robotic pet therapy. 36
Our study showed a positive screening rate of 1% which is similar to the data presented by another Singapore acute tertiary hospital of 1.61%. 1 Care for older patients is resource-intensive and requires a fine balance of managing acutely ill patients in this pandemic whilst also delivering geriatric-oriented care. Many studies have showed healthcare workers developing mental health issues such as depression and anxiety during this pandemic. 37 Therefore, psychological support should be offered to healthcare workers via individual counselling or group training. 38
At the time of this study, the turnaround time for PCR assay testing of the SARS-CoV-2 is a few hours. The importance of rapid development of point-of-care devices for the diagnosis of SARS-CoV-2 can provide a shorter turnaround time 39 and hence decrease the duration of isolation.
Strengths and Limitations
The strength of this study is that based on our knowledge, this is the first study that describes the challenges faced in managing older patients especially those with geriatric syndromes in an isolation facility.
The limitation of this study is that of the small sample size.
Conclusion
We have illustrated the challenges faced in managing older patients in a geriatric acute care isolation facility in the current COVID-19 pandemic. Such facilities are likely to be required for as long as the pandemic continues. While we acknowledge the immense difficulties in managing sick older patients with complex needs in this setting, we do not condone the use of physical restraints as a means of fall prevention. Quality improvement measures such as allowing stay-in care givers could be implemented, along with innovations in technology to augment the delirium and fall prevention protocols.
Footnotes
Acknowledgments
We would like to thank the support of Changi General Hospital and all staff involved in the care of the patients in the geriatric PARI (Pneumonia-Acute Respiratory Infection) isolation ward during this study and pandemic.
Author Contributions
K.S.G. and K.C.B.Y. were involved in the study concept/design, data acquisition, analysis and interpretation of data and writing up of the manuscript.L.H.K., M.K.J.K., S.Y.O., G.K.P., F.L., S.S. and B.A.L. were involved in the study concept/design and writing up of manuscriptW.D.V.E. was involved in data acquisition and writing up of the manuscript.
Availability of Data and Materials
The datasets generated and/or analysed during the current study are available from the corresponding author in an encrypted file.
Ethical Approval
This is a descriptive study based on routine hospital surveillance data. There were no patient identifiers involved, and exemption was granted from full ethics review by the Singhealth Centralized Institutional Review Board.
Informed Consent
Informed consent was also waived by the ethics committee
Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.