
Abstract
People with cystic fibrosis (PwCF), families, and clinicians, partner to co-produce care, navigate access barriers, address mental health and social factors, follow specific infection prevention and control practices, and share decision-making regarding treatments and daily care. Standard patient satisfaction and experience of care surveys are not tailored to return relevant, actionable data for specific populations. To improve the care experience, the U.S. CF Foundation committed to fielding a national survey in 2015. In 2020, the onset of the COVID-19 pandemic prompted revisions to capture virtual care experiences, a mode of care delivery not previously offered to PwCF. Leveraging this opportunity, the CF Foundation also reorganized how stakeholders are engaged in survey design, implementation, and improving the care experience. These changes resulted in a focused survey instrument as well as equitable and transparent data reports available to all stakeholders.
Keywords
Key points
Involving stakeholders in codesigning surveys ensured important disease-specific aspects of the care experience were included.
Engaging stakeholders to design data collection processes resulted in a system that responded to user needs and preferences.
Making data transparent and accessible to all stakeholders motivates engagement to improve the care experience.
Introduction to the Issue
Cystic fibrosis (CF) is a life-limiting, genetic disease. 1 People with CF (PwCF) receive care 4 or more times a year from a multidisciplinary healthcare team at 1 of 286 U.S. CF Foundation accredited programs. It has been long understood in the CF community that leveraging partnerships with PwCF and families is vital to improve care processes and outcomes. 2 Yet standardized patient satisfaction and experience surveys issued by most hospitals are not customizable to collect actionable data to improve disease-specific care.
In 2015, the CF Foundation designed, piloted, and deployed a national patient and family experience of care (PFEC) survey. 3 This 30-question survey was customized to cover topics relevant to CF, such as infection prevention and control, access to discipline-specific clinicians, and patient and family centered care. PwCF and families were invited by email or phone to complete a survey every 6 months. Survey results were used by programs to drive changes in local care processes and by the CF Foundation to understand national trends. 4 Program-specific and national reports were generated quarterly and distributed to clinical leaders.5,6
In 2020, with the onset of the COVID-19 pandemic, most routine CF care transitioned to telehealth. Telehealth experience data were not captured in the PFEC survey, prompting the CF Foundation to pause data collection. Foundation leaders leveraged this interruption to commission an external assessment of data collection processes, the survey instrument and reporting, and the initiative's oversight and governance. The aim was to develop a user-friendly, representative, and actionable survey and reports accessible to all stakeholders.
Description of the Interventions
The CF Foundation formed a task force of PwCF, families, and clinicians to codevelop a request for data collection proposals from commercial vendors. Taskforce members were identified and invited from programs actively engaged in the PFEC survey process, ie, those with high response rates, active interventions to improve the care experience, and sharing work nationally at conferences and in publications. Geographic location, pediatric and adult care experience, and clinical role were also considered.
The taskforce's work involved reviewing current data collection processes, including data collection flowcharts, instruction guides provided to programs, privacy, and compliance material, and features and functionality associated with completing the survey and accessing reports.
To organize revising the survey instrument and to establish oversight of the survey's implementation at care programs across the US, the CF Foundation formed a steering committee. Three community members: a parent of a child living with CF, a dietitian from an adult care team, and a pediatric pulmonologist were invited to serve as chairs. Six additional stakeholders: a person with CF, a social worker, a respiratory therapist, a parent, and an adult pulmonologist were recruited and asked to serve for 2 years.
The committee convened monthly to develop survey questions. A literature search of patient experience surveys, a review of prior versions of PFEC (2015–2020), and a telehealth survey fielded by 11 programs in 2020 7 were conducted. The committee also codesigned a dissemination and implementation plan to support the capacity of programs to execute data collection, access to program-level reports, and apply quality improvement (QI) methods 8 to improve the care experience, see Figure 1.

Cystic fibrosis (CF) experience of care survey initiative timeline.
Evidence of Impact
A Data Collection and Reporting System That Works for All Stakeholders
Data collection using the revised survey launched in October 2021. Taskforce members participated in evaluating the vendor proposals, attended interviews, and contributed feedback to help the CF Foundation make a final selection. PwCF and families stressed the need for data collection to align with current technologies, eg, use of apps and short message service (SMS) messages. Clinicians recommended process automation, eg, leveraging contact information already available and sharing with the CF Foundation to avoid duplicative data entry. These criteria were used to develop the request for proposals and subsequent evaluation of vendor submissions. This work resulted in utilizing patient/family contact information on file with the CF Foundation and PwCF and families receiving an SMS message with an invitation and link to complete a survey. An email invitation is sent if the patient/family only provides that form of contact.
The new survey data system also offered the opportunity for the steering committee to codesign report dashboards. PwCF and families stressed the importance of transparency and closing the loop to show that the feedback they provide drives improvement for themselves, their program, and the CF community, and that the effort they put into responding to the survey is meaningful and does not exist in a digital void. Clinicians sought to have reports available alongside other data reports the CF Foundation provides programs. The resulting reports are available in real time and hosted on a CF Foundation platform that PwCF, families, and clinicians can access.
A Short and Purposeful Survey to Quickly Turn Data Into Insights
During the codesign of the survey, the committee identified 16 concerns with past surveys. The most salient of these were survey length, difficulty of use, question relevancy, language barriers, lack of cultural awareness, and survey fatigue.
The committee prioritized the following goals:
keeping the survey short (5 min or less to complete) easy to access (survey invitations sent as an SMS or email link) anonymous responses (responses not linked to a PwCF or families) inclusive of Spanish speakers (survey and supporting material available in Spanish) culturally aware (demographic questions) overall quality of care infection prevention and control scheduling access to clinicians (captured in PFEC and slightly revised in XoC) shared decision-making communication well-being
The following topics were identified as priorities:
Recognizing that PwCF and families have a long-standing relationship with CF professionals, and many might not want to say anything for fear of upsetting or offending anyone, the survey responses are anonymous. The committee prioritized providing ample space for respondents to share verbatim, narrative comments directly describing the experience of CF care (see Survey Instrument in Supplemental Appendix).
To guarantee identified goals were met, drafts were presented to CF Patient and Family Advisory Boards, as well as the CF Foundation Committee of Black, Indigenous, and People of Color for feedback.
Patients, Families, and Clinicians as XoC Champion Partners
The committee's dissemination and implementation plan called for programs to assign up to 3 members as XoC Champions who would have access to their program's reporting dashboard, drive patient and family engagement, and initiate QI work to improve the care experience.
Programs are encouraged to have at least 1 person with CF or a caregiver named as an XoC Champion. Of the 175 programs fielding the survey, there is a community of 357 Champions including 297 clinicians and 60 PwCF and families (32 PwCF and 28 families). Pediatric and adult programs are evenly represented with 175 champions (49%) representing pediatric programs and 161 champions (45%) representing adult programs. Due to the smaller size and capacity of these programs, the smallest representation comes from affiliate CF programs with only 21 champions (6%) represented, see Figure 2.
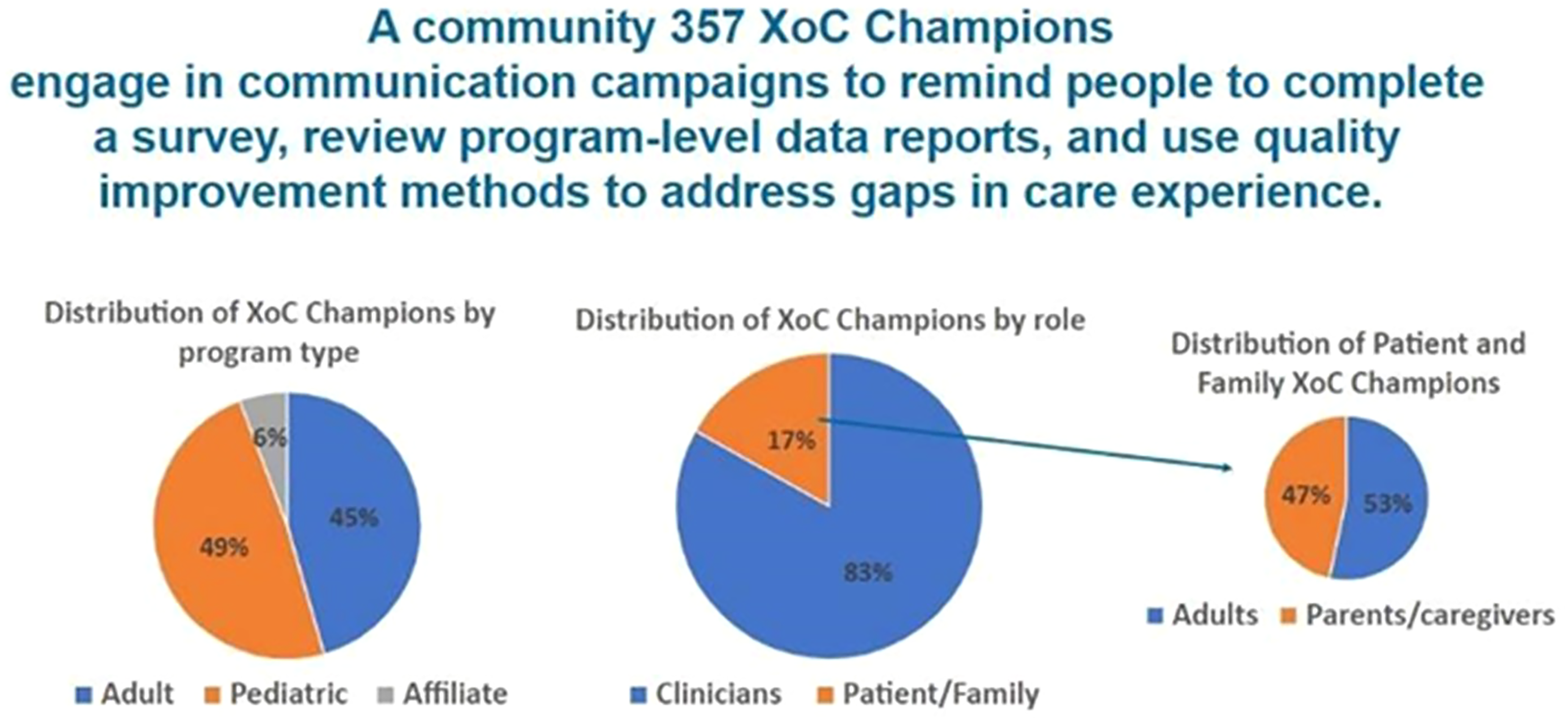
Cystic fibrosis (CF) experience of care champions.
A series of XoC Champion peer-learning sessions featured members of the committee speaking on their local processes for raising awareness about the survey, inviting PwCF and families to participate, and routinely reviewing results. Example program champions were also invited to share their work to provide insights that varied by geographical location and patient population. Subject matter experts were also invited to present to champions. Members of the CF Foundation's Partnership Enhancement Program and the QI and Innovation team provided expertise in communication skills and trust building as well as applying QI methods and preparing data-driven abstracts and presentations.
Survey data are also shared nationally. Steering committee members and individual programs have used the survey data to prepare abstracts for poster and oral presentation at the annual North American CF Conference. Annual, national reports are also prepared and distributed to all champions and programs. CF Foundation-accredited programs undergo a peer review visit every 1–5 years. Program-level survey data are shared with site visitors alongside data from the CF Foundation Patient Registry and other narrative reports to help them identify opportunities for overall improvement to raise with the program. These efforts keep the priorities of PwCF and families front and center in the community to drive improvement.
Conclusions
There are limited examples of codesigned patient experience surveys.9,10 The U.S. CF community successfully implemented a co-led redesign and transition to a shorter, less burdensome survey for PwCF and families. The XoC survey has incorporated PwCF and families in the design, implementation, and oversight of local care programs and a national initiative. Our learning has empowered CF programs to improve the quality of care and provided the CF Foundation opportunities to innovate patient experience with PwCF, families, and clinicians as equal partners. This work can be tailored to other chronic conditions.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735241302739 - Supplemental material for Cystic Fibrosis Experience of Care Survey: Patient–Caregiver–Clinician Collaborative Design and Implementation
Supplemental material, sj-docx-1-jpx-10.1177_23743735241302739 for Cystic Fibrosis Experience of Care Survey: Patient–Caregiver–Clinician Collaborative Design and Implementation by Stacy Allen, Maxwell Vetter, David W. Davison, Gemma Cochrane, Ahmet Uluer, Deidre Jennings, Fadi Asfour, Kathryn A. Sabadosa and Julianna Bailey in Journal of Patient Experience
Footnotes
Acknowledgments
The CF Foundation Experience of Care Survey initiative would not be possible without people with CF, families, and clinicians contributing their time.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Kathryn A. Sabadosa is an employee of the CF Foundation. All other authors received an honorarium from the CF Foundation to recognize their contributions to the Experience of Care Survey initiative.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.