
Abstract
The purpose of this study was to describe family engagement practices in a cardiovascular intensive care unit (CVICU) and to explore their relationship with patient outcomes. Observations were conducted on 104 patients, with most (n = 61; 58%) having family members present. On average, 1.3 ± 0.6 family members were present per observation period per patient, spending 69% of the observation time at the bedside. The most common forms of family engagement included communication (n = 61; 100%), active family presence (n = 36; 59%), and direct contribution to care (n = 35; 57%). Patients with family present were 3 times less likely to be re-admitted to the hospital within 30 days compared to those without family present (5% vs 16%; P = .05). This study offers valuable insights through direct observations of family engagement practices in a CVICU setting, offering a foundational understanding of family engagement patterns and their associations with patient outcomes. These findings establish a basis for developing targeted interventions, policies, and training programs aimed at enhancing family engagement and improving outcomes for both patients and their families in critical care settings.
Keywords
Introduction
Family engagement in care is a collaborative approach wherein family members are actively involved in patient care as partners alongside the healthcare team. 1 Engaging families in care is recommended by cardiovascular and critical care professional societies and is recognized as a fundamental component of healthcare delivery.2,3 In critical care settings, where acute illness, sedation, and analgesia may limit the patient's ability to be involved in their own care, family involvement is particularly important. 4 Family may play a role in providing physical and emotional support to patients, communication with the healthcare team, surrogate and shared decision making, and even providing care directly to their loved ones. Family involvement in intensive care has been shown to improve care quality and lead to improved patient- and family-centred outcomes. 5
Prior studies exploring patient- and family-centred care strategies have reported on overall unit practices and policies in intensive care unit (ICU) settings.6,7 However, there is limited data on how family members actually engage in care in the ICU. There is also a need to understand the relationship between family engagement practices and patient outcomes. Insufficient knowledge of the actual engagement practices of family members in the ICU setting is a gap in our understanding of family engagement in patient care.8,9
The purpose of this study is to describe the actual engagement practices of family members in a cardiovascular ICU (CVICU) and to explore the relationship between family engagement and patient outcomes. Understanding how family members engage in care is crucial for developing targeted strategies and interventions and, ultimately, improving patient- and family-centred outcomes in intensive care.
Method
Study Design and Setting
This was a prospective naturalistic observational study in the CVICU of the Jewish General Hospital (JGH), an academic tertiary care center in Montreal, Canada. The study was performed as a quality improvement (QI) project and was approved by the institutional QI department. As such, participants’ consent was not required. Institutional research ethics approval was subsequently obtained for retrospective patient data for this study. The reporting of this study was done in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.10,11
The JGH is situated in an urban setting and has a catchment area of considerable ethnic, cultural, and linguistic diversity. The JGH's CVICU has 16 beds equipped for advanced hemodynamic and ventilator support and admits adult patients with medical and surgical cardiovascular conditions. The CVICU has an open visitation policy and allows family presence at all times. As part of usual care, family visitors receive information from the nursing and allied healthcare providers regarding the ways in which they can assist with the care of their loved one (ie, assistance with mobility, oral care, or nutrition). Other family engagement strategies, which are not considered part of the usual standard of practice, include family presence during daily team rounds, resuscitation, or invasive procedures, and routine structured family care conferences to establish goals of care.
Population
Patients and family members admitted to the CVICU between October and December 2022 were eligible for observation. A “family member” was defined as anyone who was present in the patient's room and was involved in their care. 12 Patients admitted to the CVICU for short periods (less than 12 h) of postprocedure monitoring were excluded. No formal sample size calculation was required due to the nature of this observational study.
Data Sources and Measurement
Observation sessions took place on weekday mornings (7:30am-11:30am), afternoons (11:30am-3:30pm), and evenings (3:30pm-7:45pm). There were no observation sessions overnight, during weekends, or during statutory holidays. The dates of observation sessions were discontinuous and were based on study personnel availability. Each observation period was carried out in time blocks lasting approximately 2 to 4 h. During these time blocks, study personnel walked through the CVICU at 15min intervals. For each walk-through of the CVICU, study personnel recorded: (1) whether family was present in the patient's room (yes/no); (2) if yes, the number of family members present; (3) the specific engagement activities and behaviors observed. Mean times are reported to reflect engagement time across observations, rather than a period of continuous observation. For example, if a family member participated in an engagement behavior during 2 consecutive intervals, their engagement would be recorded as lasting 30 min. In order to conduct observations as unobtrusively as possible, family members were not approached by study personnel. Bias was minimized by including all admitted patients and their family members who were present during observation periods.
The type of family engagement in the ICU was categorized by domains based on Olding and colleagues’ classification system: family presence, family needs, communication, decision making, and direct care contribution. 13 Within each domain, specific engagement behaviors were identified based on our prior research (Supplemental Table S1). 14 However, only activities that could be directly observed within the context of our study were included in our observations. Family presence included behaviors such as active family presence during rounds or procedures, personalization of the patient's room, and passive in-room presence. Communication behaviors included interactions with the patient, nurses, physicians, and other healthcare providers, as well as family members facilitating patient communication with other family members (phone and video calls). Direct contribution to care included mobilizing the patient, grooming and hygiene, feeding, and assisting with medication administration. Decision-making behaviors involved participation in surrogate or shared decision-making processes. Surrogate decision making was determined when a family member was involved in decisions regarding the patient's care, which was evident either through observations of the patient's incapacitation or direct inquiries with nursing staff about the family member's role. Shared decision making was observed when the family member actively engaged in discussions with the medical team regarding care options for the patient. Family needs included visitation with the presence of other family members, involvement with social workers, and engagement in educational or informational activities like reading leaflets or watching videos. While family engagement activities have been defined by category for classification purposes, the categories of involvement are not mutually exclusive and family engagement activities may fit into more than one category. 13 For example, within the active family presence domain, a family member attending physician rounds could also be engaging in communication as the family member receives and exchanges information with the healthcare team. At the same time, the family member may participate in decision making by contributing to discussions about the patient's care plan. This overlap demonstrates that families could engage in multiple activities at once, both within and across domains.
To account for this overlap, study personnel developed a checklist to record specific engagement behaviors, allowing for double coding when necessary. For instance, if a family member was seen interacting with a social worker about psychosocial support, this could be recorded under both communication and family needs, while discussions with the medical team involving both information exchange and decision making could be recorded under both communication and decision making.
The same patient and family members could be observed over multiple sessions. If a family member exhibited the same behavior or engagement strategy multiple times across different observation periods, all occurrences were counted.
Data Collection
Study personnel prospectively collected the following data: observation duration, time of day of observation (morning, afternoon, and evening), family visitor presence, number of family members present per patient, family engagement type, and specific family engagement behaviors or activities. During the data collection process, any behaviors that did not fit into the engagement categories were documented as “other.” This ensured that all observed engagement behaviors were captured and included in the analysis.
The following patient data were collected from the electronic health record: age, sex, admission for a medical or surgical condition, length of CVICU and overall hospital stay, discharge location, death in hospital, emergency room visit within 30 days or 1 year, and re-hospitalization within 30 days or 1 year.
Statistical Analysis
Categorical data are presented as frequencies and percentages, and continuous data are presented as mean with standard deviation. Subgroup analyses were performed by categorizing patients into groups based on observations with family present versus those without family present. For categorical data, chi-squared tests were used, and Fisher's exact test was employed when 2 or more cells had expected counts less than 5 to ensure robust statistical analysis. For continuous data, between-group differences were tested with the independent samples t-test. All P values are 2-sided with values ≤ .05 indicating statistical significance. Statistical tests were done using the SPSS 29.0.1.1 statistical software (IBM Corp, Armonk, New York).
Results
Observation Sessions
There were 104 patients observed over 151 observation sessions (morning, n = 47; afternoon, n = 50; and evening, n = 54). Seventy-four patients were observed for only 1 session; 30 patients were observed over multiple sessions (range 2-6 observation periods). The mean observation time per period per patient was 161.2 ± 47.9 min. Most patients (n = 61; 59%) had family members visit during the observation period. Family was present for 49% of patients in the morning, 62% of patients in the afternoon, and 54% of patients in the evening. The mean number of family members present per period per patient was 1.3 ± 0.6. Family members were present, on average, for 69% of the observation period.
Family Engagement Practices
The most common types of family engagement domains were communication (n = 61; 100%; mean time = 74.5 ± 39.1 min), active family presence (n = 36; 59%; mean time = 24.7 ± 14.1 min), and direct contribution to care (n = 35; 57%; mean time = 27.8 ± 16.1 min; Figure 1). The most common communication activity was communication with the patient (n = 61; 100%; mean time = 70.8 ± 39.6 min; Table 1). The most common active family presence activity was presence for physician rounds (n = 20; 33%; mean time = 23.3 ± 10.6 min). The most common direct contribution to care activity was assisting with feeding behaviors (n = 23; 38%; mean time = 25.8 ± 15.1 min).

Percentage of patients observed by family engagement domain.
Family Engagement Domain and Activities.
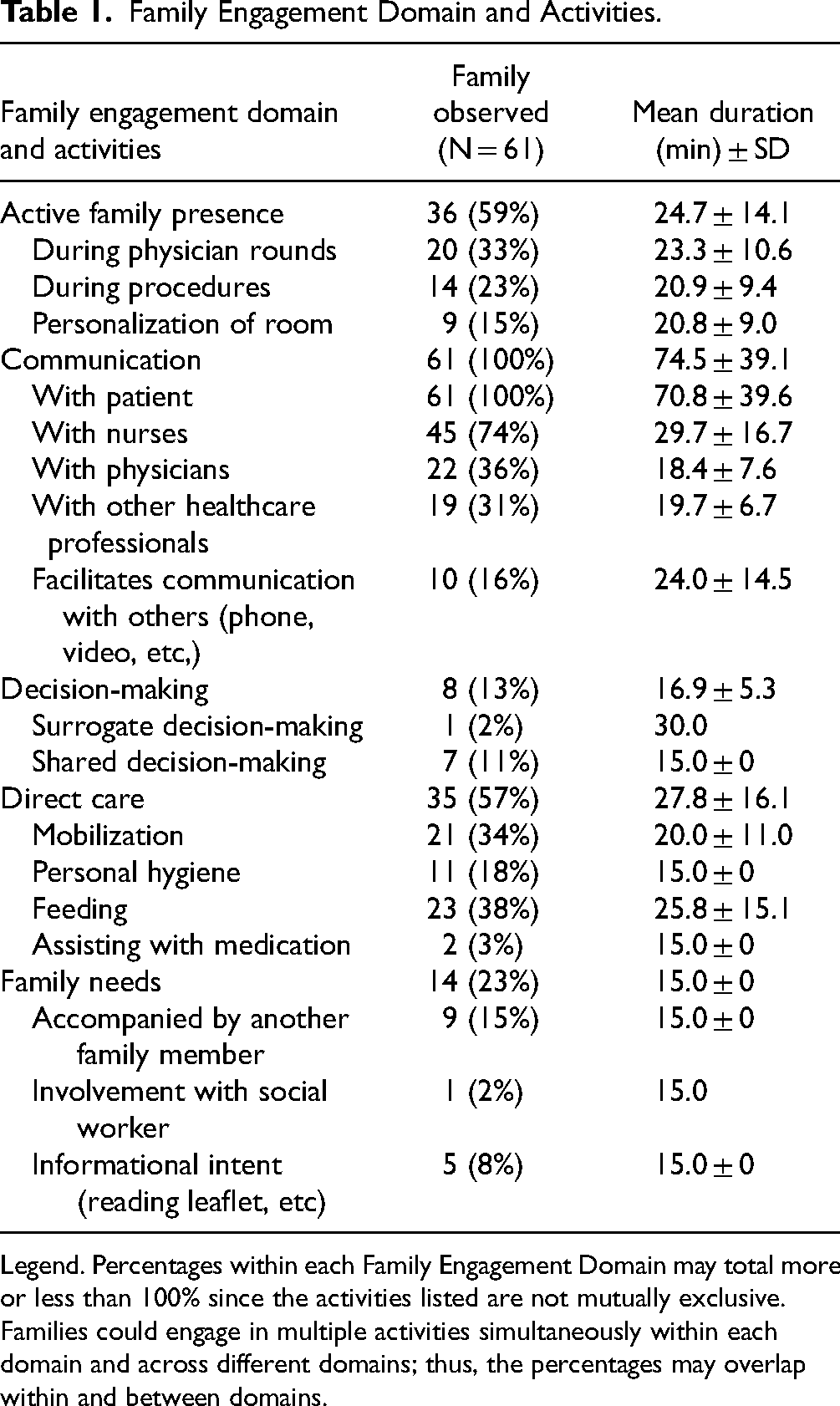
Legend. Percentages within each Family Engagement Domain may total more or less than 100% since the activities listed are not mutually exclusive. Families could engage in multiple activities simultaneously within each domain and across different domains; thus, the percentages may overlap within and between domains.
Associations Between Family Presence and Patient Outcomes
There were no differences in patient age, CVICU length of stay, or hospital length of stay for patients who had family present compared to those who did not have family present during the observation period (all P > .05; Table 2). Patients who had family present were more likely to die in the hospital as compared to those without family present (10% vs 0%, P = .04) but, when discharged, were 3 times less likely to be re-admitted to the hospital at 30 days (5% vs 16%; P = .05). There were no differences in 1-year re-admission rates or emergency room visits between the groups.
Comparison of Patient Outcomes With and Without Family Present.

Abbreviations: CVICU, cardiovascular intensive care unit; ER, emergency room.
For patients with family present, males were less likely to die and more likely to be discharged home than females (P < .05 for both; Supplemental Table S2). For patients without family present, there were no sex-specific differences in demographic and clinical characteristics.
Discussion
The purpose of this study was to observe family engagement practices in a CVICU and explore the relationship between family presence and patient outcomes. We found that family presence was common, with 59% of patients observed having family present during an observation period. Family members were primarily engaged in communication, active family presence, and direct contribution to care. Family presence was not associated with CVICU or hospital length of stay but was associated with a reduced likelihood of hospital re-admission.
Prior studies on family engagement in the critical care setting have reported the landscape of family engagement policies and practices but have not described the actual performance of family engagement practices. A survey from the World Federation of Societies of Intensive and Critical Care Medicine of 345 ICUs in 40 countries reported the frequency of how often family engagement strategies were fully, somewhat or not in place. 6 Another survey of 39 cardiac ICUs in the United States and Canada similarly reported on the frequency of family engagement strategies in their institutions. 8 However, neither of these studies reported on how family members were actually involved in care. There was one observational study of 7 ICUs in Canada that found that a family member was present in 23% of rounds. 15
To our knowledge, there has been only one prior study reported in the literature of naturalistic observations of family engagement practices in a critical care environment. Papautsky and colleagues observed family activities in a single medical ICU. 16 The focus of this study was to characterize the interactions of visitors with the clinical care team, as well as the location of these interactions, and to categorize the engagement activities performed. Visitor activities were considered as either information exchanges with the healthcare team or as nonclinical patient care, and then further divided into subcategories. Like our study, a trained observer visualized the presence and activities of family members unobtrusively from outside the patient room. Similarly, observations did not take place overnight or during statutory holidays. However, there were several key differences as compared to our study. The study by Papautsky and colleagues qualitatively described the type of engagement activities performed and developed a new categorization scheme of engagement activities based on their observations, whereas our study quantified the time spent performing each engagement activity in a cardiac ICU using established engagement categories. Our study also included patient outcomes, which allowed us to explore the relationship between family engagement and patient outcomes. The current study thus complements and adds to the only prior reported observational study of this population in the ICU setting.
Prior studies of family involvement in the ICU setting primarily obtained insight into family experiences and involvement in care once the patient (along with their family member) had already left the ICU. 17 These studies are likely subject to recall bias and may not adequately capture how family members actually spend their time interacting with team members and being involved in patient care-related activities. In addition, studies exploring family involvement have largely been qualitative in nature.16,18 While qualitative studies are important and needed to gain insight into the family experience, quantitative efforts, such as in our study, can provide more objective data that can allow for comparisons, be generalized to a larger population, and be more actionable in terms of effecting policy and culture change.
The most prevalent engagement activities observed were communication with the patient and healthcare team members, active presence during rounds, and direct contribution to patient care. Evidence-based family engagement strategies can be implemented into standard critical care practice to support the performance of these activities. ICU communication facilitators have been shown to reduce family depression. 19 Family participation in ICU rounds is another engagement strategy that has shown promise but has not been widely implemented.6,8,20 Novel strategies can also be developed to target areas where engagement may be lacking, such as decision making about treatment and goals of care. In addition, many family members may wish to be more involved in care but do not have the knowledge or opportunity to increase their level of participation. 21 Further research is needed to understand which engagement strategies are accepted by family members, and which strategies family members wish to be more involved in.
Our study advances the understanding of family engagement in ICUs by linking family engagement with patient factors and outcomes. We identified an association between family being present during an observation period and reduced likelihood of re-admission following hospital discharge. It is possible that family members who were present were more likely to act as caregivers for ICU survivors, and that ICU survivors who have caregivers were less likely to require hospital re-admission. A recent study found that family caregiver involvement for ICU survivors is associated with reduced hospital re-admission. 22 In addition, we found that patients who had family present were more likely to die in the CVICU than those without family present. Family may be more likely to be present when their loved ones are critically ill or in a palliative state, either to spend more time with them or to participate in shared decision making. Given the observational nature of the study, these findings should be viewed cautiously, as a causative relationship between family presence and patient survival or hospital re-admission cannot be established. Generating evidence that links family engagement in ICU care to improved patient outcomes is crucial, as the lack of convincing evidence may be a limiting factor for family engagement uptake in routine critical care delivery. The relationship between family engagement and patient outcomes needs to be explored further in future studies.
Patient and family interactions in the ICU likely vary across different cultural backgrounds and languages. Indeed, a study of 226 family members in 3 ICUs found that families identifying as Black or a race other than White were more likely to participate in personal care, touch, or spiritual care. 23 As our study did not collect detailed demographic information on family members, the impact of linguistic and cultural differences in family involvement could not be evaluated. There is a need for additional research on how language and cultural considerations might influence family engagement patterns in care. Tailored approaches to family involvement in care may be developed to address any differences in language or cultural expectations.
Our findings support efforts to encourage policymakers and hospital leadership to increase implementation of family engagement strategies in routine practice. Specifically, these findings, in conjunction with the growing evidence base, support changes in ICU visitor policies, staff training programs, and strategies for integrating families into the decision-making process.
Limitations
There were several limitations to this study. First, this was an observational study performed in a single CVICU, which limits the generalizability of the findings to other critical care settings or geographic regions. Studies in other ICU settings and locations are warranted to improve the characterization of family involvement in care. Second, detailed family member demographic data was not collected; approaching family members to collect this data could influence their behavior and skew the naturalistic observations. Third, observations were only conducted on weekdays during daytime hours, potentially overlooking variations in family engagement practices on weekends, evenings, or holidays. Future studies could consider longitudinal data collection spanning multiple days or weeks to provide a more comprehensive understanding of family engagement patterns. Fourth, certain aspects of family engagement, such as private conversations or interactions behind closed curtains, may not have been fully captured during observations. Fifth, the noncontinuous nature of the observations may result in both underestimations and overestimations of actual family engagement time. Behaviors observed during a single interval were rounded to a full 15 min, leading to potential overestimations of engagement time. Conversely, if family members engaged in activities between observation intervals that were not captured, this could result in underestimations of their actual involvement. Finally, as an observational study, no determination can be made regarding causality between engagement practices and patient outcomes.
Conclusion
Our study represents an initial effort to characterize actual family engagement behaviors in an intensive care setting. This information can be used to plan engagement strategies within ICUs. Further studies are needed to better characterize family engagement across a broad range of ICU types and settings.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251330463 - Supplemental material for Direct Observation of Family Engagement Practice in a Cardiovascular Intensive Care Unit
Supplemental material, sj-docx-1-jpx-10.1177_23743735251330463 for Direct Observation of Family Engagement Practice in a Cardiovascular Intensive Care Unit by Jillian Kifell, Douglas Slobod, Krystina B. Lewis, and Michael Goldfarb in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735251330463 - Supplemental material for Direct Observation of Family Engagement Practice in a Cardiovascular Intensive Care Unit
Supplemental material, sj-docx-2-jpx-10.1177_23743735251330463 for Direct Observation of Family Engagement Practice in a Cardiovascular Intensive Care Unit by Jillian Kifell, Douglas Slobod, Krystina B. Lewis, and Michael Goldfarb in Journal of Patient Experience
Footnotes
Authors’ Contributions
JK and MG conceptualized and designed the study, analyzed the data, performed statistical analyses, and interpreted the results. They also wrote the manuscript and performed manuscript revisions. JK was responsible for data collection. DS and KL assisted with interpreting the results and revising and editing the manuscript. All authors reviewed and approved the final manuscript.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Goldfarb is supported by a Clinical Research Award from the Fonds de recherche du Québec.
Ethical Considerations
This study received ethical approval from the Medical/Biomedical Research Ethics Committee (REC) of CIUSSS West-Central Montreal Research Ethics Board (REB) (approval #20224-4011) on December 01, 2023.
Consent to Participate
All procedures in this study were conducted in accordance with the approved protocols of Medical/Biomedical Research Ethics Committee (REC) of the CIUSSS West-Central Montreal Research Ethics Board (REB) (approval #20224-4011). This is an IRB-approved retrospective study. Informed consent for publication of patient information was not obtained because all patient information was de-identified, presented as grouped data, and consent was not required. Patient data will not be shared with third parties.
Data Availability
The data supporting this study's findings are available upon request from the corresponding author. Due to ethical and privacy considerations, the data cannot be publicly shared. Researchers who wish to access the data must contact the corresponding author with a detailed request outlining their intended use of the data. Data sharing will be subject to approval by the relevant ethics committee.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.