
Abstract
In an online, survey-based experiment, musculoskeletal surgeon members of the science of variation group (n = 243) and a group of consult-liaison psychiatrists (n = 18) read 5 hypothetical scenarios of patients recovering from musculoskeletal trauma, each containing 5 randomized patient variables, and indicated their recommendation for psychiatry consultation or not. Factors associated with recommendation for psychiatry consultation included younger age, history of a psychiatric disorder, and pre-injury use of antipsychotic medications, and scenarios involving psychosis, suicidality, hallucinations in the setting of substance withdrawal, and questionable capacity for informed consent, but not with sadness alone. Musculoskeletal surgeons can collaborate with psychiatrists to develop comprehensive care for inpatients with musculoskeletal trauma starting with relatively pressing mental health needs and perhaps expanding into treatment of sadness or worry that can manifest as greater symptom intensity and a delayed recovery trajectory.
Introduction
There is evidence that psychological and social factors have notable associations with levels of mental and physical discomfort after musculoskeletal trauma. 1 Important barriers to addressing psychosocial factors identified in previous work include a sense that it will take too much time, lack of awareness of psychosocial aspects of illness, discomfort with screening for and discussing psychological aspects of illness, and the stigma associated with mental health. 2 Among people injured severely enough to be admitted to a hospital, there is an opportunity for social work, psychology, or psychiatric consultation to help optimize recovery. However, these resources are limited and many health systems rely upon the surgeon to recognize psychosocial barriers to recovery, understand the importance of these opportunities for improved health, and ask for help from colleagues. 1
In a recent pilot study, orthopedic surgery residents and psychiatry residents agreed on thresholds for suicidality, drug misuse, and capacity to consent that merited psychiatry consultation. 3 However, they disagreed about schizophrenia and delirium. Reasons for these differences, based on qualitative data, may include a lack of experience with antipsychotic medications and orthopedic resident confidence in the management of delirium. 3 It is unknown if these findings are generalizable or institution-specific or if the respondents’ status as trainees affected the results.
The purpose of this study was to determine which patient scenarios (eg, age and psychiatric symptoms) and physician factors (including being a surgeon or psychiatrist) were independently associated with the recommendation for a psychiatry consultation in a multiinstitutional survey of orthopedic surgeons and psychiatrists.
Methods
Study Design
This survey-based, study of randomized aspects of common clinical scenarios was approved by the Institutional Review Board. The Science of Variation Group (SOVG) is an international collaborative of musculoskeletal surgeons who study variations in care using online, survey-based, experiments that measure associations, often by randomizing the material presented to participants. This study was designed by 2 members of the SOVG and their research teams, none of whom participated in the study. In addition to the SOVG, we invited faculty from all psychiatry departments with consult-liaison fellowship programs in the United States (publicly available contact information). 4
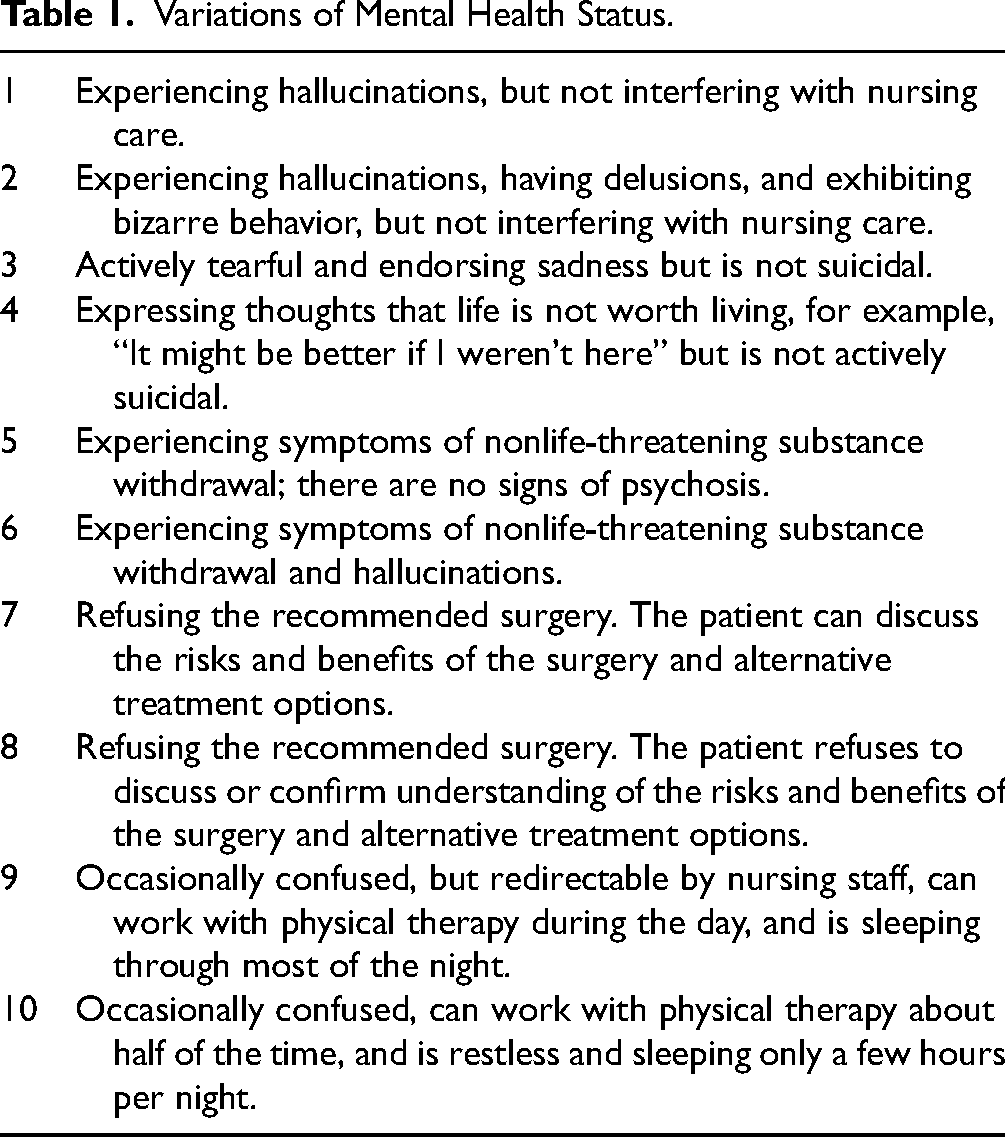
We used SurveyMonkey© (San Mateo, CA, USA) to develop the survey. 4 Participants were asked about their sex, years in independent practice, practice location, supervision of trainees, surgeon or psychiatrist, subspecialty [for surgeons only], and availability of an inpatient psychiatry consultation service and inpatient musculoskeletal trauma team at their institution. We presented each participant with 5 of 10 hypothetical scenarios involving patients recovering from musculoskeletal trauma (Table 1). The scenarios also randomized the following 4 elements based on a survey piloted in previous work: 3 patient age (25 vs 75 years old), sex (man/woman), history of psychiatric disorder (present or absent), and the use of psychiatric medication (none, antipsychotics, anxiolytics, or antidepressants). Each variable in each scenario was randomly assigned for each participant (50%: 50% in case of 2 options and 25% each for variables with 4 options). Participants were asked to indicate whether or not they, as the treating surgeon or consulting psychiatrist, would recommend a psychiatry consultation for each fictitious patient.
Variations of Mental Health Status.
Between August 9 and September 5, 2018, all members of the SOVG were sent an invitation to participate in this study, with 2 reminder emails if they did not respond. Because SOVG experiments do not report rates and other survey information that would not be represent the average musculoskeletal surgeon or psychiatrist, and because we have a list of emails of several hundred musculoskeletal surgeons some of which may be inactive, we do not track response rates. Two-hundred-forty-three surgeons and 18 psychiatrists completed the survey-based experiment, of which 220 (91%) and 11 (61%) were men, respectively. The majority resided in the United States (US; 50%) and Europe (33%; [Table 2]). There were significantly more women in the psychiatrist group and all of them were from the United States.
Surgeon and Psychiatrist Characteristics and Baseline Differences.

Discrete variables as number (percentage). Bold = P < .05.
Statistical Analysis
We performed a multilevel multivariable logistic regression analysis, with random intercepts at the level of the cases and the physicians, seeking patient and physician factors (including being a surgeon or psychiatrist) associated with the recommendation for a psychiatric consultation. Discrete data are presented as proportions. Odds ratios (OR), 95% confidence intervals (CI), and standard errors (SE) are reported. A P value < .05 was considered statistically significant.
Results
Factors independently associated with the recommendation of a psychiatric consult included younger age (OR 1.6; P = .004), history of psychiatric disorder (OR 4.7; P < .001), and preinjury use of an antipsychotic medication (OR 2.3; P < .001; [Table 3]). Factors independently associated with not recommending a psychiatric consult were (compared to “experiencing hallucinations, but not interfering with nursing care”) “being actively tearful and endorsing sadness, but not suicidal” (OR 3.8; P < .001), “experiencing symptoms of nonlife-threatening substance withdrawal, but no signs of psychosis” (OR 4.5; P < .001), “refusing the recommended surgery, but can discuss the risks and benefits of the surgery and alternative treatment options” (OR 4.5; P < .001), “being occasionally confused, but redirectable by nursing staff, can work with physical therapy during the day, and is sleeping through most of the night” (OR 14; P < .001), and “being occasionally confused, can work with physical therapy about half of the time, and is restless and sleeping only a few hours per night” (OR 2.9; P = .001; [Table 3]). This means that scenarios 2, 4, 6, and 8 (hallucinations and bizarre behavior, suicidality, substance withdrawal with hallucinations, and questionable capacity for informed consent) were associated with psychiatry consultation comparable to scenario 1 (“experiencing hallucinations not interfering with care”). None of the physician variables were associated with a recommendation for a psychiatry consultation (Table 3).
Multilevel Logistic Regression Analysis of Factors Associated With Recommendation for a Psychiatry Consultation.

Abbreviation: CI, confidence interval.
Bold indicates a statistically significant difference.
Patient sex and some psychiatric/psychological statuses are not displayed since they are not significant.
Physician gender, years in practice, and availability of inpatient psychiatry consults or a trauma team are not displayed since they are not significant.
Discussion
A better understanding of the current factors associated with recommendations for psychiatry consultation for inpatients recovering from musculoskeletal trauma could help inform more comprehensive, biopsychosocial care strategies. This survey- and scenario-based experiment tested randomized elements of patient scenarios in order to determine factors associated with the musculoskeletal surgeon and psychiatrist recommendations for a psychiatry consultation in this setting. A psychiatry consultation was more likely to be recommended for younger patients, those with a documented psychiatric disorder, and those taking antipsychotic medications (but not anxiolytics or antidepressants). Clinical scenarios more likely to generate a recommendation for a psychiatric consultation included delusions and bizarre behavior (psychosis), passive suicidality, hallucinations in the setting of substance use, and unwillingness or inability to discuss informed consent for a surgical procedure. Notably, scenarios involving delirium were less likely to result in a psychiatry consultation.
This study has a number of limitations. The percentage of psychiatrist participants was relatively small (18 total, 7%) compared to the orthopedic surgeons. The most likely reason for this is that surgeons were contacted via the robust and established SOVG, while psychiatrists were contacted via publicly available email addresses. This means there were fewer psychiatrists who sent the survey and those who received it were probably less likely to participate. The current study was, therefore, likely underpowered to detect a difference between the surgeon and psychiatrist groups. Additionally, the availability of psychosocial support resources is variable from hospital to hospital, and these differences may mean that these results are not completely generalizable or could have led to a bias among respondents with more (or less) availability of a psychiatry service at their hospital. Psychiatrists were also contacted via publicly available email addresses from academic institutions, further limiting the generalizability to the average psychiatrist who may be in community practice. We attempted to use clinical vignettes to impart a sense of a patient's overall clinical picture but may have left out important details or information that respondents use for their own decision-making; however, we did perform a pilot study with trainees to capture as many of these factors as possible. 3 The clinical scenarios we used incorporated symptoms reflective of major psychiatric diagnoses (psychosis, suicidality, delirium, etc), but we did not attempt to study other common and impactful psychosocial issues such as homelessness, less effective coping strategies, financial or employment insecurity, and family problems. We also studied the physician's understanding of the patient's behavior or capacity, which would likely vary by physician. This source of bias is partially accounted for by the large number of participants and the randomization of the material in the scenarios, but it is present in the wording of the scenarios by the authors.
The finding that bizarre behavior, suicidality, substance withdrawal with hallucinations, and questionable capacity for informed were associated with recommendation for a psychiatry consultation is consistent with a previous survey of trainees. That survey identified agreement between surgeons and psychiatrists with regard to a consultation threshold for suicidality, substance misuse, and capacity to consent and divergence regarding patients with delirium (surgeons less often) and schizophrenic psychosis (surgeons more often). 3 This is consistent with a recent study of patients in the intensive care unit that found that 68% developed delirium but psychiatry consultation was requested for only 1.7%. 5 Given the associated morbidity, greater attention to symptoms of delirium can be justified. One prospective study of 126 older-aged people with hip fractures found that delirium developed in 41% and persisted at one month postoperatively in 33%. 6 The development of delirium was independently associated with poor one-month outcomes controlling for baseline age and cognition. 6 Psychiatry consultation might have the potential to improve outcomes of the treatment of delirium.6–8
Musculoskeletal surgeons are somewhat cautious of psychosis. One previous retrospective study of people recovering from knee or hip arthroplasty found that patients with a history of bipolar disorder, schizophrenia, or antipsychotic use were significantly more likely to develop a complication postoperatively. 9 Surgeons can consider asking for help early in the hospital course.7–10
Conclusions
The finding that recommendation for psychiatry consultation is associated with specific mental health issues that can benefit from expertise has face validity. It also suggests that musculoskeletal surgeons may think of mental health mostly in relatively specific or extreme forms. Future research could address less apparent but common sources of psychosocial distress in the trauma population, such as financial or housing insecurity and unhelpful thinking or feelings of distress regarding symptoms.
Footnotes
Acknowledgments
We would like to thank all participating members of the Science of Variation Group.
Authors’ Contributions
Not applicable.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors certify that they have no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors. Informed consent was not required for this anonymous survey study. This study was performed in accordance with the ethical standards in the 1964 Declaration of Helsinki. This study has been carried out in accordance with relevant regulations of the US Health Insurance Portability and Accountability Act (HIPAA).
Statement of Human and Animal Rights
Not applicable.
Statement of Location
This study was performed at Stanford University Medical Center and The Dell Medical School of The University of Texas at Austin.
Patient Consent
Not applicable.
Informed Consent
Not applicable.